Download as docx, pdf, or txt
You might also like
- Chapter 4 VALUES, ATTITUDES AND JOB SATISFACTIONDocument30 pagesChapter 4 VALUES, ATTITUDES AND JOB SATISFACTIONChristian Yapchai Galolo78% (9)
- Safal Niveshak Mastermind Free ChaptersDocument31 pagesSafal Niveshak Mastermind Free Chaptersthisispraveen100% (2)
- Traffic Control Plan - SampleDocument23 pagesTraffic Control Plan - SampleSuriya Prakash.mNo ratings yet
- Benzene: 1. Purpose 2. ScopeDocument8 pagesBenzene: 1. Purpose 2. ScopeKandhasamy888No ratings yet
- Qcs 2010 Section 11 Part 2.3.11 She Procedures - Permit To Work SysteDocument20 pagesQcs 2010 Section 11 Part 2.3.11 She Procedures - Permit To Work Systebryanpastor106No ratings yet
- Olifantsvlei: General Site Operations - Flame CuttingDocument4 pagesOlifantsvlei: General Site Operations - Flame CuttinggrantNo ratings yet
- Occupational Health Saftey Management Plan (OHMSP) - NZDocument29 pagesOccupational Health Saftey Management Plan (OHMSP) - NZRam P0% (1)
- Protocol On Heavy Rainfall For The Private Sector 17.02.21 Revised FinalDocument9 pagesProtocol On Heavy Rainfall For The Private Sector 17.02.21 Revised FinalLe Mauricien100% (1)
- 2-Suspended Personnel PlatformsDocument14 pages2-Suspended Personnel PlatformsAlaa AllamNo ratings yet
- Chapter 1-Introduction To OshaDocument32 pagesChapter 1-Introduction To OshafettaneNo ratings yet
- Upload Cold StressDocument7 pagesUpload Cold Stresskpowers15No ratings yet
- Dosecc Health ManualDocument62 pagesDosecc Health ManualRachmad HazanNo ratings yet
- Electrical SafetyDocument17 pagesElectrical SafetymuhammadkashikNo ratings yet
- Safe Handling CylinderDocument7 pagesSafe Handling CylinderAbdulKatherNo ratings yet
- Right To Refuse or To Stop WorkDocument6 pagesRight To Refuse or To Stop WorkpsicologothNo ratings yet
- Toolbox Talks - Safety Data SheetsDocument1 pageToolbox Talks - Safety Data SheetsJerby GabrielNo ratings yet
- Elec Hazard Awareness Study GuideDocument5 pagesElec Hazard Awareness Study GuideBố Đăng KhánhNo ratings yet
- 11.2 Baseline Medical Surveillance ProcedureDocument18 pages11.2 Baseline Medical Surveillance ProcedureaceNo ratings yet
- (Insert Company Name) : Employee Safety & Injury Prevention ProgramDocument31 pages(Insert Company Name) : Employee Safety & Injury Prevention Programeliasox123100% (1)
- 13.2.11 RA SWP For Installation of Instruments and Instrument Tubing at DCLDocument17 pages13.2.11 RA SWP For Installation of Instruments and Instrument Tubing at DCLkeertiraj09100% (1)
- Hazard Communication ProgramDocument3 pagesHazard Communication ProgramindheatingNo ratings yet
- Confined Space Entry Program 11 2021Document16 pagesConfined Space Entry Program 11 2021zaka ullahNo ratings yet
- Sop Occupational Safety and Health Complaints Mechanism UnitDocument12 pagesSop Occupational Safety and Health Complaints Mechanism UnitEmdad YusufNo ratings yet
- Near Miss Toolbox TalkDocument2 pagesNear Miss Toolbox Talkpruncu.alianmNo ratings yet
- Safety - Preventing Serious Injury and Fatalities - Chevrons Field Guide - Part 1Document12 pagesSafety - Preventing Serious Injury and Fatalities - Chevrons Field Guide - Part 1Priyo Djatmiko100% (1)
- Confine Space Entry (Excavation)Document32 pagesConfine Space Entry (Excavation)Delta akathehuskyNo ratings yet
- Arkansas Kraft Division Contractor Safety OrientationDocument63 pagesArkansas Kraft Division Contractor Safety Orientationdavid_stephens_29No ratings yet
- 09 COMAH GuidanceDocument8 pages09 COMAH GuidanceSaad GhouriNo ratings yet
- Alexander County Government Housekeeping PolicyDocument3 pagesAlexander County Government Housekeeping PolicySol AbonNo ratings yet
- Confined Space SapDocument2 pagesConfined Space SapfairusNo ratings yet
- Tahmina-Zebin-General Risk Assessment FormDocument6 pagesTahmina-Zebin-General Risk Assessment FormTahmina L. ZebinNo ratings yet
- Personal Protective EquipmentDocument22 pagesPersonal Protective EquipmentAdam H100% (1)
- 25 - Welding, Cutting and Hot WorkDocument16 pages25 - Welding, Cutting and Hot WorkRicardo DalisayNo ratings yet
- Health & Safety Handouts ComDocument52 pagesHealth & Safety Handouts ComTyra GeorgesNo ratings yet
- Unsafe ActDocument1 pageUnsafe ActAnuj SinghNo ratings yet
- Safety & Health ProgramDocument2 pagesSafety & Health ProgramD.k. PathakNo ratings yet
- Confined Space - Introduction: Canadian Government Departments Responsible For OH&S Confined Space - ProgramDocument7 pagesConfined Space - Introduction: Canadian Government Departments Responsible For OH&S Confined Space - ProgramAnge JuanNo ratings yet
- SWP Fire PumpDocument6 pagesSWP Fire PumpbsynnottNo ratings yet
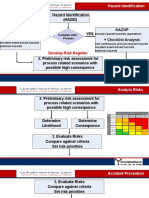
- Hazard Identification (Hazid) NO YES: Checklist Analysis Hazop + Checklist AnalysisDocument7 pagesHazard Identification (Hazid) NO YES: Checklist Analysis Hazop + Checklist AnalysisZeroRecoNo ratings yet
- Exit Route: A Continuous and Unobstructed PathDocument31 pagesExit Route: A Continuous and Unobstructed PathRudi Fajardo100% (1)
- Staff Safety InductionDocument5 pagesStaff Safety InductionAbuzar Khan Ameeni100% (1)
- Fire Emergency Evacuation Plan and The Fire ProcedureDocument6 pagesFire Emergency Evacuation Plan and The Fire ProcedurejohnnyroddNo ratings yet
- Risk Assesment Fab - Rev-07Document71 pagesRisk Assesment Fab - Rev-07Nikhil PuthiryNo ratings yet
- 5 Years Road Map: Objectives TargetDocument3 pages5 Years Road Map: Objectives TargetRajesh VermaNo ratings yet
- BGP Visitor HSE InductionDocument2 pagesBGP Visitor HSE InductionittehadNo ratings yet
- Department of Health.: Occupational Health & Safety PolicyDocument10 pagesDepartment of Health.: Occupational Health & Safety PolicyMuhammad SaeedNo ratings yet
- HSSE Statistics For The Past 5 YearsDocument4 pagesHSSE Statistics For The Past 5 YearsNikhil VermaNo ratings yet
- Aprile HSES PolicyDocument2 pagesAprile HSES PolicyAprile NetworkNo ratings yet
- Behavior Based Safety BBS Observation FormDocument1 pageBehavior Based Safety BBS Observation Formtony sNo ratings yet
- 0I. Accident Causes and PreventionDocument52 pages0I. Accident Causes and PreventionGregor Clegane100% (1)
- Safe Work Method For Peb Work: Procedure Possible Hazards Control MeasuresDocument35 pagesSafe Work Method For Peb Work: Procedure Possible Hazards Control Measuressandip patilNo ratings yet
- Presentation: "Emergency Preparedness"Document63 pagesPresentation: "Emergency Preparedness"vidhya sagarNo ratings yet
- Occupational HealthDocument16 pagesOccupational HealthfaarehaNo ratings yet
- Doe Guide To Good Practices For Lockouts and Tagouts Doe-Std-1030-96Document49 pagesDoe Guide To Good Practices For Lockouts and Tagouts Doe-Std-1030-96Titer100% (1)
- Machine Guarding Checklist: Questions Requirements For All SafeguardsDocument2 pagesMachine Guarding Checklist: Questions Requirements For All SafeguardsAVENON MardocheeNo ratings yet
- Employee Welfare Program Feb - 2010Document12 pagesEmployee Welfare Program Feb - 2010Javaid SalimNo ratings yet
- Plant Hazard and Vulnerability Analysis: InstructionsDocument7 pagesPlant Hazard and Vulnerability Analysis: Instructionsjohn doeNo ratings yet
- Health and Safety Management in HealthcareDocument6 pagesHealth and Safety Management in HealthcareDr.ManageNo ratings yet
- Econ 110: Principles of Microeconomics: Problem SetDocument8 pagesEcon 110: Principles of Microeconomics: Problem SetJoe OstingNo ratings yet
- The Nursing Code of Ethics Its Value, Its HistoryDocument14 pagesThe Nursing Code of Ethics Its Value, Its HistoryalifahNo ratings yet
- A Study On Impact of Rewards and Recognition in Hindustan Unilever Ltd.Document1 pageA Study On Impact of Rewards and Recognition in Hindustan Unilever Ltd.saikiabhascoNo ratings yet
- Performance Appraisal 8Document9 pagesPerformance Appraisal 8Pooja DemblaniNo ratings yet
- OJT Final Compilation Journal Accomplishment ActivitiesDocument14 pagesOJT Final Compilation Journal Accomplishment ActivitiesKenn Ian De VeraNo ratings yet
- Gamillo v. MariñoDocument10 pagesGamillo v. MariñoJoanna RosemaryNo ratings yet
- Directing: DIRECTING Is Said To Be A Process in Which The Managers Instruct, Guide and Oversee TheDocument36 pagesDirecting: DIRECTING Is Said To Be A Process in Which The Managers Instruct, Guide and Oversee Thekiran mahalNo ratings yet
- Shell Co. V VanoDocument1 pageShell Co. V VanoLouNo ratings yet
- SPEECH BY H.E. BENJAMIN WILLIAM MKAPA, FORMER PRESIDENT OF THE UNITED REPUBLIC OF TANZANIA, FOR THE 3RD GRADUATION CEREMONY AT MUNYONYO INTERNATIONAL RESORT, LAKE SIDE CAVENDISH UNIVERSITY UGANDA, 27TH NOVEMBER 2013Document7 pagesSPEECH BY H.E. BENJAMIN WILLIAM MKAPA, FORMER PRESIDENT OF THE UNITED REPUBLIC OF TANZANIA, FOR THE 3RD GRADUATION CEREMONY AT MUNYONYO INTERNATIONAL RESORT, LAKE SIDE CAVENDISH UNIVERSITY UGANDA, 27TH NOVEMBER 2013Muhidin Issa MichuziNo ratings yet
- 360 Degree Appraisal SystemDocument2 pages360 Degree Appraisal SystemHabibAfzalNo ratings yet
- Viernes Vs NLRCDocument1 pageViernes Vs NLRCpja_14100% (2)
- Human Capital Management - LupinDocument4 pagesHuman Capital Management - LupinLAKSHMI BALAKRISHNAN MBA19-21No ratings yet
- Test Bank For Human Resource Management Gaining A Competitive Advantage 9Th Edition by Noe Hollenback Gerhart and Wright Isbn 9780078112768 007811276 Full Chapter PDFDocument36 pagesTest Bank For Human Resource Management Gaining A Competitive Advantage 9Th Edition by Noe Hollenback Gerhart and Wright Isbn 9780078112768 007811276 Full Chapter PDFsimon.esche558100% (21)
- Tutorial 8 MCQ QuestionDocument2 pagesTutorial 8 MCQ QuestionMC SquiddyNo ratings yet
- Sta Lucia East Commercial Vs Secretary of Labor DigestDocument3 pagesSta Lucia East Commercial Vs Secretary of Labor DigestJay Ribs100% (1)
- Christina Pellegrino: ObjectiveDocument2 pagesChristina Pellegrino: Objectiveapi-269473546No ratings yet
- Recruitment Manual 2022 For Construction CompanyDocument18 pagesRecruitment Manual 2022 For Construction CompanyNgọc HuyềnNo ratings yet
- Selection of Dip Aprrentices For Adani EletricityDocument3 pagesSelection of Dip Aprrentices For Adani EletricityFiroz AminNo ratings yet
- Overhead DistributionDocument86 pagesOverhead DistributionEkta Saraswat VigNo ratings yet
- Good Job Application Letter SampleDocument7 pagesGood Job Application Letter Sampleidyuurvcf100% (2)
- Organizational Behavior: Moods and EmotionsDocument22 pagesOrganizational Behavior: Moods and EmotionsWasim Jamali100% (1)
- City of Glasgow College Full Time Prospectus 2013 - 2014 PDFDocument84 pagesCity of Glasgow College Full Time Prospectus 2013 - 2014 PDFCity of Glasgow CollegeNo ratings yet
- Hazard Pay LguDocument1 pageHazard Pay LgudhEnz JanNo ratings yet
- Introduction To Business Communication...Document50 pagesIntroduction To Business Communication...Shruti VermaNo ratings yet
- Motivational Factors and The Hospitality IndustryDocument7 pagesMotivational Factors and The Hospitality IndustryMã Lương Thiên NhiNo ratings yet
- VishakaDocument6 pagesVishakaRahul DubeyNo ratings yet
- Comparative Analysis of HRM StrategiesDocument15 pagesComparative Analysis of HRM StrategiesEva RlndnNo ratings yet
- MBA Assignment NIBMDocument48 pagesMBA Assignment NIBMimran abdul azizNo ratings yet