Download as pdf or txt
You might also like
- Ebook Developing Person Through Childhood and Adolescence 11Th Edition Ebook PDF All Chapter PDF Docx KindleDocument47 pagesEbook Developing Person Through Childhood and Adolescence 11Th Edition Ebook PDF All Chapter PDF Docx Kindlehazel.field513100% (31)
- OB 1st PNCUDocument8 pagesOB 1st PNCUAngelo Erispe100% (1)
- 2 - Pre Gestational ConditionDocument11 pages2 - Pre Gestational ConditionAngelica Dalit MendozaNo ratings yet
- CME Miscarriages Combined 1Document76 pagesCME Miscarriages Combined 1syawal zulfitriNo ratings yet
- Nle - High-Risk PregnancyDocument113 pagesNle - High-Risk Pregnancytachycardia01No ratings yet
- NCM 109 Problems With Power DraftDocument3 pagesNCM 109 Problems With Power DraftJP Porras Ali100% (1)
- Assessment of Fetal Well-Being 1. Fetal MovementDocument6 pagesAssessment of Fetal Well-Being 1. Fetal MovementClaire Julianne CapatiNo ratings yet
- Post TermDocument16 pagesPost Termahmed shorsh100% (1)
- Rachel PpromDocument15 pagesRachel PpromGeneNo ratings yet
- Placenta IsuogDocument40 pagesPlacenta IsuogKARINA BASTIDAS IBARRA100% (1)
- NCM 102 OB Abnormal 2Document113 pagesNCM 102 OB Abnormal 2Maria Garcia Pimentel Vanguardia IINo ratings yet
- Post Term PregnancyDocument12 pagesPost Term PregnancyRizky Putra Ismeldi100% (1)
- PaedsDocument72 pagesPaedsOlivia Genevieve El JassarNo ratings yet
- O&G LO SlidesDocument60 pagesO&G LO Slideskatherine nunnNo ratings yet
- By Gemechu M (MD)Document26 pagesBy Gemechu M (MD)Semon YohannesNo ratings yet
- Gestational 1Document8 pagesGestational 1RoseAngelyne VicenteNo ratings yet
- ? - PEDIA PRELIMS Lessons 1 and 2Document8 pages? - PEDIA PRELIMS Lessons 1 and 2ysabel.mendozaNo ratings yet
- ObsGyn RR @academycerebellumDocument180 pagesObsGyn RR @academycerebellumNeeladri DawnNo ratings yet
- Einc-Updates 231024 214348Document7 pagesEinc-Updates 231024 214348Alexander Nicole DomingoNo ratings yet
- High Risk Pregnancy:: A Woman Who Develops A Complication of PregnancyDocument79 pagesHigh Risk Pregnancy:: A Woman Who Develops A Complication of PregnancyMike Faustino SolangonNo ratings yet
- Preterm Labour and PROMDocument25 pagesPreterm Labour and PROMNinaNo ratings yet
- Bleeding During PregnancyDocument4 pagesBleeding During PregnancyCarl Andre ReyesNo ratings yet
- Obg AbortionDocument62 pagesObg Abortionkashyap priyankaNo ratings yet
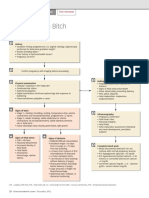
- Dystocia in The BitchDocument2 pagesDystocia in The BitchGissele ParaisoNo ratings yet
- Trans SaVi Lec08 Obstetrics Post Term Pregnancy 1st SemesterDocument7 pagesTrans SaVi Lec08 Obstetrics Post Term Pregnancy 1st SemesterAdrian CaballesNo ratings yet
- Jose, Leana Louisse D. Cornell Notes On Ncm109 Module 1 & 2 (Complications of Pregnancy) 02/18/21 Assessment For Risk FactorsDocument19 pagesJose, Leana Louisse D. Cornell Notes On Ncm109 Module 1 & 2 (Complications of Pregnancy) 02/18/21 Assessment For Risk FactorsLiana Louisse JoseNo ratings yet
- Antepartum HaemorrhageDocument21 pagesAntepartum HaemorrhageDavina DakapNo ratings yet
- Obstetric Highlights, Elmar P. SakalaDocument47 pagesObstetric Highlights, Elmar P. Sakaladukelist5660% (1)
- Abruptio Placenta and AbortionDocument10 pagesAbruptio Placenta and Abortiondanica grace gubaNo ratings yet
- Intrapartal ComplicationsDocument8 pagesIntrapartal ComplicationsLizeth Querubin100% (4)
- K-Medics Placental Previa - AbruptionDocument28 pagesK-Medics Placental Previa - AbruptionMichael AdjeiNo ratings yet
- GEMS Obstetrics and GynaecologyDocument59 pagesGEMS Obstetrics and GynaecologyUMARRA SHAFIQUENo ratings yet
- PromDocument26 pagesPromAhmed MohammedNo ratings yet
- Antepartum BleedingDocument37 pagesAntepartum BleedingMae Importers IncNo ratings yet
- 9 - Postterm PregnancyDocument22 pages9 - Postterm PregnancyMara Medina - BorleoNo ratings yet
- Usg Webinar Bioprofil Bayi PrintDocument36 pagesUsg Webinar Bioprofil Bayi PrintElfan WinotoNo ratings yet
- Multifetal Pregnancy: Herman Sumawan FK Unsoed/Rs Margono SoekarjoDocument70 pagesMultifetal Pregnancy: Herman Sumawan FK Unsoed/Rs Margono SoekarjoTitisPudyatikaDestyaAndiraNo ratings yet
- Umbilical Cord AccidentsDocument16 pagesUmbilical Cord Accidentschebetnaomi945No ratings yet
- HemorrhagesDocument3 pagesHemorrhagesARAugustoNo ratings yet
- MCN ReviewerDocument4 pagesMCN ReviewerMaria Arabella LanacaNo ratings yet
- Alarm-Perdarahan Antepartum PDFDocument5 pagesAlarm-Perdarahan Antepartum PDFUmmu Qonitah AfnidawatiNo ratings yet
- Case 2 TG Retype PDFDocument15 pagesCase 2 TG Retype PDFElma CorpusNo ratings yet
- ABORTIONDocument3 pagesABORTIONAngel MoncadaNo ratings yet
- Prolonged PregnancyDocument29 pagesProlonged PregnancyNur Agami100% (1)
- Maternity Nursing NotesDocument7 pagesMaternity Nursing NotesazitaaaaaNo ratings yet
- CH 5 MDocument6 pagesCH 5 MShaafieNo ratings yet
- Student Unit 2 Topic 2.5 Jan 2018 TAYLORDocument42 pagesStudent Unit 2 Topic 2.5 Jan 2018 TAYLORKrista KloseNo ratings yet
- Pedia GyneDocument13 pagesPedia Gynerjh1895No ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument94 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- Pprom 1 1Document20 pagesPprom 1 1Tehreem AzharNo ratings yet
- Gestational ConditionsDocument4 pagesGestational ConditionsHyacinth Mae Virtudazo RaganasNo ratings yet
- Abnormal Uterine Bleeding: Presented By: Shubhangi A Redij Guided By: Dr. Ashwini Morale MamDocument15 pagesAbnormal Uterine Bleeding: Presented By: Shubhangi A Redij Guided By: Dr. Ashwini Morale MamS RedijNo ratings yet
- Physiologic SignsDocument59 pagesPhysiologic SignsChari RivoNo ratings yet
- Abortion Chapter 18 Willobs 25th EdDocument40 pagesAbortion Chapter 18 Willobs 25th EdNabil MaulanaNo ratings yet
- 19 - Obstetric ImagingDocument12 pages19 - Obstetric ImagingAbhijith J PuttananickalNo ratings yet
- Antepartum Fetal Surveillance: Chandani PandeyDocument98 pagesAntepartum Fetal Surveillance: Chandani Pandeychandani pandeyNo ratings yet
- Management of Placenta Previa During Pregnancy: M Hadyan Syahputra 71 2016 055Document14 pagesManagement of Placenta Previa During Pregnancy: M Hadyan Syahputra 71 2016 055khaira_nNo ratings yet
- Ectopic Pregnancy: ObgyneDocument2 pagesEctopic Pregnancy: ObgyneLuis PadillaNo ratings yet
- OralsOB EctopicDocument2 pagesOralsOB EctopicKrista P. AguinaldoNo ratings yet
- AbortionsDocument25 pagesAbortionsaravindNo ratings yet
- It's Not Just a Heavy Period; The Miscarriage HandbookFrom EverandIt's Not Just a Heavy Period; The Miscarriage HandbookRating: 2 out of 5 stars2/5 (1)
- Pharma 2nd Sem Prelims RatioDocument11 pagesPharma 2nd Sem Prelims RatioicNo ratings yet
- OPIATESDocument2 pagesOPIATESicNo ratings yet
- Psych Finals CompiledDocument13 pagesPsych Finals CompiledicNo ratings yet
- Compiled Psych MidtermsDocument13 pagesCompiled Psych MidtermsicNo ratings yet
- Psych Finals PlatingsDocument13 pagesPsych Finals PlatingsicNo ratings yet
- Basic SuturingDocument14 pagesBasic SuturingicNo ratings yet
- Family Planning (Hormonal Contraceptives)Document2 pagesFamily Planning (Hormonal Contraceptives)icNo ratings yet
- Primary AmenorrheaDocument2 pagesPrimary AmenorrheaicNo ratings yet
- NRP ppt1Document29 pagesNRP ppt1sumana BanerjeeNo ratings yet
- Obstetrical Nursing AntepartumDocument28 pagesObstetrical Nursing AntepartumAyeza DuaNo ratings yet
- Pregnancy: Signs/Symptoms and Common Health ConcernsDocument5 pagesPregnancy: Signs/Symptoms and Common Health ConcernsTracy50% (2)
- Prenatal Period of Development EportfolioDocument4 pagesPrenatal Period of Development Eportfolioapi-367895274No ratings yet
- Grande MultiparaDocument6 pagesGrande MultiparaAgus Wijaya100% (2)
- Maternal HealthcareDocument124 pagesMaternal HealthcareEstellaNo ratings yet
- The Effect of Maternal - Fetal Attachment Education On Maternal MenDocument7 pagesThe Effect of Maternal - Fetal Attachment Education On Maternal MenNadia RifeldaNo ratings yet
- Prevention of Congenital Syphilis Through Antenatal Screenings in Lusaka, Zambia: A Systematic ReviewDocument11 pagesPrevention of Congenital Syphilis Through Antenatal Screenings in Lusaka, Zambia: A Systematic ReviewlianaNo ratings yet
- Lesson 4 Infancy by HurlockDocument44 pagesLesson 4 Infancy by HurlockJessica Recaido100% (1)
- Antecedents of CPDocument8 pagesAntecedents of CPЯковлев АлександрNo ratings yet
- Beversdorf 2018 DissDocument12 pagesBeversdorf 2018 DissJacob NotHank FrancisNo ratings yet
- High Risk Pregnancy HB TranxDocument11 pagesHigh Risk Pregnancy HB TranxangeliquepastranaNo ratings yet
- Advanced Maternal Age & PregnancyDocument67 pagesAdvanced Maternal Age & PregnancyMa Pilar Peñaflor AñonuevoNo ratings yet
- W1-L3-Human Development - Heredity and Environment200414060604044949Document14 pagesW1-L3-Human Development - Heredity and Environment200414060604044949Sachidananda AngomNo ratings yet
- NURS325 04 Antepartum PeriodDocument58 pagesNURS325 04 Antepartum PeriodaliNo ratings yet
- Human Development A Life Span View 8th Edition Ebook PDFDocument61 pagesHuman Development A Life Span View 8th Edition Ebook PDFnaomi.parker972100% (56)
- No. 197b-Fetal Health SurveillanceDocument25 pagesNo. 197b-Fetal Health SurveillanceMaríaNo ratings yet
- Care of New BornDocument14 pagesCare of New Bornshubham vermaNo ratings yet
- ANC Guideline PresentationDocument42 pagesANC Guideline PresentationDeepak BamNo ratings yet
- NSG Seminar Sas 1 13 CompilationDocument94 pagesNSG Seminar Sas 1 13 CompilationNiceniadas CaraballeNo ratings yet
- The Earliest Relationship Parents, Infants, and The Drama of EaDocument280 pagesThe Earliest Relationship Parents, Infants, and The Drama of EaBogdan BNo ratings yet
- Maternal NursingDocument48 pagesMaternal NursingMarwa DaghNo ratings yet
- Intellectual DiabilityDocument10 pagesIntellectual DiabilityAngelo PapimNo ratings yet
- Preterm and Posterm Birth: Oleh: DR Adi Setyawan Prianto SP - OG (K)Document31 pagesPreterm and Posterm Birth: Oleh: DR Adi Setyawan Prianto SP - OG (K)ATIKAH NUR HAFIZHAHNo ratings yet
- Fetal Growth RestrictionDocument56 pagesFetal Growth RestrictionKanika VermaNo ratings yet
- PDF Children Thirteenth Edition Edition John W Santrock Ebook Full ChapterDocument53 pagesPDF Children Thirteenth Edition Edition John W Santrock Ebook Full Chapterjoy.james964100% (2)
- Fetal DevelopmentDocument51 pagesFetal DevelopmentLhiet Aguilar Hipolito67% (3)
- Browne 2011Document11 pagesBrowne 2011Gisele Elise MeninNo ratings yet