Download as pdf or txt
You might also like
- The Musculoskeletal SystemDocument23 pagesThe Musculoskeletal SystemEduardoAlejoZamoraJr.100% (5)
- Cal Dietz Advance Methods in Triphasic Training FinalDocument42 pagesCal Dietz Advance Methods in Triphasic Training FinalRyan Hicks100% (16)
- Maintenance FluidDocument27 pagesMaintenance FluidganeshyaeNo ratings yet
- WEEK 5 Management of Patients With Fluids and ElectrolytesDocument89 pagesWEEK 5 Management of Patients With Fluids and ElectrolytesErica P. ManlunasNo ratings yet
- Water BalanceDocument9 pagesWater BalanceKim Mae ComendadorNo ratings yet
- Serum Electrolytes-Part 1Document22 pagesSerum Electrolytes-Part 1Marwa 2002No ratings yet
- Aspect To Consider in Fluid TherapyDocument34 pagesAspect To Consider in Fluid TherapyhanifahNo ratings yet
- ELECTROLYTES (Na & K)Document3 pagesELECTROLYTES (Na & K)Alondra SagarioNo ratings yet
- DR - Sabah Noori 1Document26 pagesDR - Sabah Noori 1Mighty AbodyNo ratings yet
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- Supplementary Information To Chapter 30: Overview of Electrolyte BalanceDocument11 pagesSupplementary Information To Chapter 30: Overview of Electrolyte BalanceAaron JoseNo ratings yet
- Gangguan Keseimbangan Cairan Dan ElektrolitDocument45 pagesGangguan Keseimbangan Cairan Dan Elektrolitmulyo utomoNo ratings yet
- Water and Sodium 2024 PDFDocument61 pagesWater and Sodium 2024 PDFMpho MosehlaNo ratings yet
- Kuliah S2 Dasar Air-ElekDocument38 pagesKuliah S2 Dasar Air-ElekViany RehansyahNo ratings yet
- Electrolytes: Dedykusuma@ugm - Ac.idDocument20 pagesElectrolytes: Dedykusuma@ugm - Ac.idRama DhistaNo ratings yet
- Fluid and Electrolyte Imbalances Part 1Document34 pagesFluid and Electrolyte Imbalances Part 1Gabrielle Frances FernandezNo ratings yet
- Fluid & Electrolytes: DR Win Min OoDocument55 pagesFluid & Electrolytes: DR Win Min OoBiomedical Science MyanmarNo ratings yet
- Body Fluids: M. Alif Prizarky 04011381419173 GammaDocument7 pagesBody Fluids: M. Alif Prizarky 04011381419173 GammaAlviss RmidNo ratings yet
- ELECTROLYTES EditedDocument6 pagesELECTROLYTES EditedKrystel Bea DinqueNo ratings yet
- Electrolyte 1Document8 pagesElectrolyte 1Ylooner QuitsNo ratings yet
- 1 Fluid and ElectrolyteDocument51 pages1 Fluid and ElectrolyteSanjiv SharmaNo ratings yet
- Gangguan Keseimbangan Cairan Dan Elektrolit Pada PGKDocument89 pagesGangguan Keseimbangan Cairan Dan Elektrolit Pada PGKfransiska wijoyoNo ratings yet
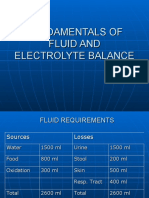
- Fundamentals of Fluid and Electrolyte BalanceDocument46 pagesFundamentals of Fluid and Electrolyte BalanceMelia Eka Rosita PharmacistNo ratings yet
- 1 Fluid and ElectrolyteDocument51 pages1 Fluid and ElectrolyteSanjiv SharmaNo ratings yet
- FLuid & Elect & Acid Base & Surg. Nutr.Document24 pagesFLuid & Elect & Acid Base & Surg. Nutr.anon_761270640No ratings yet
- Acid BaseDocument95 pagesAcid BaseMiracle For NursesNo ratings yet
- Composition of Fluid & ElectrolytesDocument33 pagesComposition of Fluid & ElectrolytesDwi SiregarNo ratings yet
- Hyponatremia: ElectrolytesDocument5 pagesHyponatremia: ElectrolytesCyreen Jill Aliling100% (1)
- Gangguan Dan Keseimbangan Cairan Dan ElektrolitDocument37 pagesGangguan Dan Keseimbangan Cairan Dan ElektrolitFyana PutriNo ratings yet
- Renal Physiology ReviewDocument7 pagesRenal Physiology ReviewHOD AnesthesiaNo ratings yet
- Phys Offluidselectrolytes7 121107201529 Phpapp02Document38 pagesPhys Offluidselectrolytes7 121107201529 Phpapp02Rehab weridaNo ratings yet
- Kuliah 8. Safety Handling of Infusion ProductDocument63 pagesKuliah 8. Safety Handling of Infusion ProductElva SorumbaNo ratings yet
- Management Terapi CairanDocument60 pagesManagement Terapi CairanHayat Hamzah DawiNo ratings yet
- MD-4 Body Fluid Compartments PlasmaaDocument24 pagesMD-4 Body Fluid Compartments PlasmaavincenzoNo ratings yet
- Fluid ElektrolitDocument63 pagesFluid ElektrolitsyifaNo ratings yet
- Fluids & ElectrolytesDocument18 pagesFluids & ElectrolytesBiway RegalaNo ratings yet
- FluidDocument31 pagesFluidZainab BasimNo ratings yet
- Intravenous Fluids: Composition & UsesDocument41 pagesIntravenous Fluids: Composition & UsesFathima BanuzNo ratings yet
- Water and ElectrolyteDocument26 pagesWater and ElectrolyteCarmen MolinaNo ratings yet
- Happy Valentine's DayDocument34 pagesHappy Valentine's Dayapi-19916399No ratings yet
- Sodium and PotassiumDocument4 pagesSodium and PotassiumLUALHATI VILLASNo ratings yet
- Dasar - Dasar Terapi: Cairan Dan ElektrolitDocument60 pagesDasar - Dasar Terapi: Cairan Dan ElektrolitdedeNo ratings yet
- Kuliah Mineral 2015-2016Document20 pagesKuliah Mineral 2015-2016molenNo ratings yet
- Acid-Base Interpretation: APRIL 4, 2017Document9 pagesAcid-Base Interpretation: APRIL 4, 2017mohamedsmnNo ratings yet
- Fisiologi Sel Dan Cairan Tubuh: M.Ihwan KusumaDocument20 pagesFisiologi Sel Dan Cairan Tubuh: M.Ihwan KusumaHenny AprianiNo ratings yet
- Serum Potassium: DR Sana Iqbal JanjuaDocument18 pagesSerum Potassium: DR Sana Iqbal JanjuahadibabaNo ratings yet
- Hypokalemia 2Document32 pagesHypokalemia 2aqilasafikaNo ratings yet
- Terapi Cairan Pada AnakDocument48 pagesTerapi Cairan Pada AnakAstri Novia RizqiNo ratings yet
- Blood Gas InterpretationDocument67 pagesBlood Gas Interpretationmajdy2006No ratings yet
- RCPCH TAS Renal Anatomy and Physiology Patrick DaviesDocument25 pagesRCPCH TAS Renal Anatomy and Physiology Patrick DaviesWaleed abdul hayeeNo ratings yet
- 1 Echilibrul HidroelectroliticDocument1 page1 Echilibrul HidroelectroliticStudiareRomaniaNo ratings yet
- Fluid and Electrolyte MGT in SurgeryDocument40 pagesFluid and Electrolyte MGT in SurgeryJohn AgamahNo ratings yet
- Elektrolit DisorderDocument2,743 pagesElektrolit DisordervioletaNo ratings yet
- Fluid and Electrolyte Balance in ICUDocument46 pagesFluid and Electrolyte Balance in ICUtapas_kbNo ratings yet
- Fluids: Presenter: Atwebembere Raymond Faciliitator: Dr. KibengoDocument34 pagesFluids: Presenter: Atwebembere Raymond Faciliitator: Dr. KibengoNinaNo ratings yet
- Normal Water Balance and ElectrolytesDocument47 pagesNormal Water Balance and ElectrolytesTheBoss 20No ratings yet
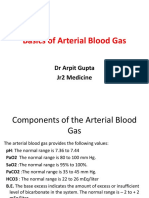
- ArpitDocument73 pagesArpitDurgesh PushkarNo ratings yet
- Fisiologi Cairan MikDocument18 pagesFisiologi Cairan MikRezky Prilya WidyastutiNo ratings yet
- Management Terapi CairanDocument60 pagesManagement Terapi Cairanpeter singalNo ratings yet
- Dr. Tiu - Electrolyte RequirementsDocument64 pagesDr. Tiu - Electrolyte Requirementshippypsyduck mdNo ratings yet
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansFrom EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpNo ratings yet
- Ojsadmin, 219Document5 pagesOjsadmin, 219AmnaNo ratings yet
- Rock Hard Training PlanDocument20 pagesRock Hard Training PlanPiyush Raj SinhaNo ratings yet
- CVP MonitoringDocument24 pagesCVP MonitoringChoji Heiwajima100% (1)
- RESPIRATIONDocument5 pagesRESPIRATIONShatviga VisvalingamNo ratings yet
- CV Examples PDFDocument5 pagesCV Examples PDFAsp Corp SlaveNo ratings yet
- Seventh Grade Circulatory SystemDocument8 pagesSeventh Grade Circulatory SystemCarlo MakilingNo ratings yet
- Scoring SleepDocument100 pagesScoring SleepWinnie MugoNo ratings yet
- Peripheral Nervous System & Autonomic Nervous SystemDocument28 pagesPeripheral Nervous System & Autonomic Nervous Systemobsgynunair januari18No ratings yet
- Procedure:: Pada HastasanaDocument11 pagesProcedure:: Pada HastasanaSidharth TaylorNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaloveummyabbyNo ratings yet
- Science 9 Module 1 Week 1 PDFDocument26 pagesScience 9 Module 1 Week 1 PDFMarco Angelo Lebios86% (7)
- Shock ManagementDocument17 pagesShock ManagementAmare EshetieNo ratings yet
- Diabetes InsidipusDocument2 pagesDiabetes InsidipusLena RoweNo ratings yet
- Acfrogclhto 41rcs7k2x9e9ozhxq6xpyvgxibnamac Wqxg3qiugn 4ovgkuedgemtgeegex2qkvdx2s2tntnpedoovxbx7hfd Okc69rl78zkapufum4ws5t7y1wsieja3x1yqkshoglfvwtjgDocument3 pagesAcfrogclhto 41rcs7k2x9e9ozhxq6xpyvgxibnamac Wqxg3qiugn 4ovgkuedgemtgeegex2qkvdx2s2tntnpedoovxbx7hfd Okc69rl78zkapufum4ws5t7y1wsieja3x1yqkshoglfvwtjgBoy MadNo ratings yet
- FORSCI313 - Questions and Answers - Group 2Document3 pagesFORSCI313 - Questions and Answers - Group 2Almarie Lyn LandaoNo ratings yet
- Acute Leukemia: Heart (Myocardial) InfarctionDocument4 pagesAcute Leukemia: Heart (Myocardial) InfarctionSisham SubediNo ratings yet
- Ketonuria 1Document10 pagesKetonuria 1Habib UllahNo ratings yet
- Chapter - 028.bridge To NCLEX Review Question AnswersDocument7 pagesChapter - 028.bridge To NCLEX Review Question AnswersJackie JuddNo ratings yet
- Adrenergic NS 2Document43 pagesAdrenergic NS 2Abdullah Muhammed khaleel HassanNo ratings yet
- Marcus Lo - Sleep Inducer - PaperDocument5 pagesMarcus Lo - Sleep Inducer - Paperagentdog175No ratings yet
- Module 5 HA Pain Assessment The Fifth Vital SignsDocument12 pagesModule 5 HA Pain Assessment The Fifth Vital SignsCalvo AdrianNo ratings yet
- Science Performance TaskDocument2 pagesScience Performance TaskJoshNo ratings yet
- Fdar HypertensionDocument12 pagesFdar HypertensionKasandra Dawn Moquia BerisoNo ratings yet
- Physiology Summary Chapter 32Document2 pagesPhysiology Summary Chapter 32gail018No ratings yet
- Science 10 Q3 Week 3Document10 pagesScience 10 Q3 Week 3John ver PitaoNo ratings yet
- The Neonatal Period (N2)Document25 pagesThe Neonatal Period (N2)api-3721542100% (1)
- Multiparameter Patient Monitors-1Document12 pagesMultiparameter Patient Monitors-1robert robNo ratings yet
- Makalah Basic Life SupportDocument22 pagesMakalah Basic Life SupportKustian PramuditaNo ratings yet