Download as pdf or txt
You might also like
- Water Cures - Drugs Kill - How Water Cured Incurable Diseases (PDFDrive)Document244 pagesWater Cures - Drugs Kill - How Water Cured Incurable Diseases (PDFDrive)Mohammad0% (1)
- ACTIVITY 3 Identifying Sentence ErrorsDocument4 pagesACTIVITY 3 Identifying Sentence ErrorsApril MasongNo ratings yet
- My Lesson PlanDocument8 pagesMy Lesson Planapi-29785663293% (15)
- Oral Health in Asthmatic Patients: A Review: Clinical and Molecular AllergyDocument8 pagesOral Health in Asthmatic Patients: A Review: Clinical and Molecular AllergyJOSE VALDEMAR OJEDA ROJASNo ratings yet
- Endotype-Driven Treatment in Chronic Upper Airway DiseasesDocument14 pagesEndotype-Driven Treatment in Chronic Upper Airway DiseaseslockyNo ratings yet
- Articol Coacaz Negru PDFDocument5 pagesArticol Coacaz Negru PDFManu MandaNo ratings yet
- Effectiveness of FeNO Guided Treatment in Adult Asthma Patients A Systematic ReviewDocument11 pagesEffectiveness of FeNO Guided Treatment in Adult Asthma Patients A Systematic ReviewFikrieNo ratings yet
- WAO-ARIA Consensus On Chronic Cough - Part 3 Management Strategies in Primary and Cough-Specialty CareDocument20 pagesWAO-ARIA Consensus On Chronic Cough - Part 3 Management Strategies in Primary and Cough-Specialty CareNabilah AnandaNo ratings yet
- FULLTEXT01Document21 pagesFULLTEXT01mason.sadeghiNo ratings yet
- 2022 Lin Sun - Difference of Serum Cytokine Profile in Allergic A RetrieveDocument12 pages2022 Lin Sun - Difference of Serum Cytokine Profile in Allergic A RetrieveSteve aokiNo ratings yet
- The Heterogeneity of Chronic Cough: A Case For Endotypes of Cough HypersensitivityDocument11 pagesThe Heterogeneity of Chronic Cough: A Case For Endotypes of Cough HypersensitivityNadia hasibuanNo ratings yet
- KlasifikasiDocument8 pagesKlasifikasinurul sachrani putriNo ratings yet
- Evaluation of Antibiotics On Chronic Obstructive Pulmonary Disease Patient in Lung Hospital, West Sumatera, IndonesiaDocument4 pagesEvaluation of Antibiotics On Chronic Obstructive Pulmonary Disease Patient in Lung Hospital, West Sumatera, IndonesiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jaa 4 001 PDFDocument12 pagesJaa 4 001 PDFRulianti BarantiNo ratings yet
- Cough HipersensitivityDocument21 pagesCough HipersensitivityNabilah AnandaNo ratings yet
- NCM 112 Lec 2Document64 pagesNCM 112 Lec 2JIMENEZ, TRISHA MARIE D.No ratings yet
- Uric Acid, Blood Pressure, and Gout Management (PDFDrive)Document200 pagesUric Acid, Blood Pressure, and Gout Management (PDFDrive)Aurveda SE HealNo ratings yet
- The Prevalence of Allergic Rhinitis in Asthmatics and The Impact On Bronchial Asthma Control: A Single Center ExperienceDocument6 pagesThe Prevalence of Allergic Rhinitis in Asthmatics and The Impact On Bronchial Asthma Control: A Single Center ExperienceangelNo ratings yet
- Mometasone Furoate Nasal Spray-Systemic ReviewDocument5 pagesMometasone Furoate Nasal Spray-Systemic ReviewRobin ScherbatskyNo ratings yet
- Inhaled Corticosteroids Safety and Adverse Effects-DikonversiDocument8 pagesInhaled Corticosteroids Safety and Adverse Effects-DikonversiRachmi MerrinaNo ratings yet
- Treatment Trends in Allergic Rhinitis and Asthma: A British ENT SurveyDocument5 pagesTreatment Trends in Allergic Rhinitis and Asthma: A British ENT SurveyAndra LaszloNo ratings yet
- JurnalDocument8 pagesJurnalhidayatullahNo ratings yet
- 欧洲呼吸学会成人及儿童慢性咳嗽诊治指南Document31 pages欧洲呼吸学会成人及儿童慢性咳嗽诊治指南GaryNo ratings yet
- Asthma Dissertation IdeasDocument6 pagesAsthma Dissertation IdeasPaperWriterServiceSingapore100% (1)
- Feno Revision Sistematica Italia 2020Document20 pagesFeno Revision Sistematica Italia 2020Estefania Yu AcevedoNo ratings yet
- Asma RefractarioDocument9 pagesAsma RefractarioFlavio GuillenNo ratings yet
- Actual Concepts in Rhinosinusitis: A Review of Clinical Presentations, in Ammatory Pathways, Cytokine Profiles, Remodeling, and ManagementDocument18 pagesActual Concepts in Rhinosinusitis: A Review of Clinical Presentations, in Ammatory Pathways, Cytokine Profiles, Remodeling, and ManagementAurum MortNo ratings yet
- Allergy - 2008 - Sastre - Ebastine in Allergic Rhinitis and Chronic Idiopathic UrticariaDocument20 pagesAllergy - 2008 - Sastre - Ebastine in Allergic Rhinitis and Chronic Idiopathic UrticariaBabar TayyabNo ratings yet
- Buerger's DiseaseDocument8 pagesBuerger's DiseaseELSA HANA AL MUNAWAROHNo ratings yet
- Pi Is 1323893016301745Document27 pagesPi Is 1323893016301745Afria TikaNo ratings yet
- Asthma Term PaperDocument4 pagesAsthma Term Papereryhlxwgf100% (1)
- Asthma Case PresentationDocument3 pagesAsthma Case Presentationfernandezrachelle44No ratings yet
- Corticosteroids and Steroid Therapy 2015 Carmen Adkins PDFDocument129 pagesCorticosteroids and Steroid Therapy 2015 Carmen Adkins PDFSalahuddin ShikalgarNo ratings yet
- Copd Overlap AsthmaDocument8 pagesCopd Overlap AsthmaYaYakNo ratings yet
- ATCAM - Volume 1 - Issue Issue 1-2 - Pages 12-21 PDFDocument10 pagesATCAM - Volume 1 - Issue Issue 1-2 - Pages 12-21 PDFqalbiNo ratings yet
- A Review of The Metered Dose Inhaler Technique in Asthmatic and COPD PatientsDocument7 pagesA Review of The Metered Dose Inhaler Technique in Asthmatic and COPD PatientsselviaNo ratings yet
- B Russell e 2013Document10 pagesB Russell e 2013Arief Janurachman HakimNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- 9410 41584 6 PBDocument9 pages9410 41584 6 PBMuzaki AndiyantoNo ratings yet
- Severe Asthma in Primary Care: Identification and ManagementDocument8 pagesSevere Asthma in Primary Care: Identification and ManagementIzza UrfanNo ratings yet
- Dissertation Topics On AsthmaDocument8 pagesDissertation Topics On AsthmaWhereToBuyResumePaperCanada100% (1)
- Factors Related To Severe Acute Asthma Attack and Treatment: IJPSR (2012), Vol. 3, Issue 08 (Research Article)Document4 pagesFactors Related To Severe Acute Asthma Attack and Treatment: IJPSR (2012), Vol. 3, Issue 08 (Research Article)Tanvir HayderNo ratings yet
- Severe and Difficult-to-Treat Asthma in Adults: Review ArticleDocument12 pagesSevere and Difficult-to-Treat Asthma in Adults: Review ArticlePatricio MiguelNo ratings yet
- Rhinosinusitis: Alexi Decastro,, Lisa Mims,, William J. HuestonDocument15 pagesRhinosinusitis: Alexi Decastro,, Lisa Mims,, William J. HuestonkikoNo ratings yet
- Synopsis Submitted To: Application For The Registration of Subjects For Dissertation of TheDocument14 pagesSynopsis Submitted To: Application For The Registration of Subjects For Dissertation of TheAraafathNo ratings yet
- Asthama VireshDocument34 pagesAsthama VireshVarun MahajaniNo ratings yet
- 2023 Risk Factors of NSAID Exacerbated Respiratory DiseaseDocument22 pages2023 Risk Factors of NSAID Exacerbated Respiratory Diseasexiongmao2389No ratings yet
- Exacerbations of CopdDocument10 pagesExacerbations of CopdMelissa PeñataNo ratings yet
- Community-Acquired Pneumonia: Strategies for ManagementFrom EverandCommunity-Acquired Pneumonia: Strategies for ManagementAntoni TorresRating: 4.5 out of 5 stars4.5/5 (2)
- The Burden of Allergic Rhinitis and Asthma: Tunis Ozdoganoglu and Murat SonguDocument13 pagesThe Burden of Allergic Rhinitis and Asthma: Tunis Ozdoganoglu and Murat Songudanaagus81No ratings yet
- Ana Phy RespiratoryDocument5 pagesAna Phy Respiratorydayang ranarioNo ratings yet
- Ra 2 PDFDocument6 pagesRa 2 PDFRikaRistantiNo ratings yet
- BMJ Pediatric Asthma in A NutshellDocument14 pagesBMJ Pediatric Asthma in A NutshellarjumandNo ratings yet
- Treatment Strategies For Asthma: Reshaping The Concept of Asthma ManagementDocument11 pagesTreatment Strategies For Asthma: Reshaping The Concept of Asthma Managementtegarsh321No ratings yet
- Cough Management A Practical ApproachDocument12 pagesCough Management A Practical ApproachYohan YudhantoNo ratings yet
- Japanese Guidelines For Childhood Asthma 2017 PDFDocument15 pagesJapanese Guidelines For Childhood Asthma 2017 PDFcindy315No ratings yet
- Management - of - Chronic - Respiratory - and - Allergic - DisDocument20 pagesManagement - of - Chronic - Respiratory - and - Allergic - DisjoseNo ratings yet
- Children 10 01571Document9 pagesChildren 10 01571billyolivierapattiasina25No ratings yet
- 2000 Journal of The California Dental AssociationDocument20 pages2000 Journal of The California Dental AssociationUnyar LeresatiNo ratings yet
- Ers BeDocument24 pagesErs Bedicky wahyudiNo ratings yet
- EFFICACY OF HOMOEOPATHIC SIMILLIMUM IN TREATING ATOPIC BRONCHIAL ASTHMA WITH AN EVALUATION BASED ON IgEDocument13 pagesEFFICACY OF HOMOEOPATHIC SIMILLIMUM IN TREATING ATOPIC BRONCHIAL ASTHMA WITH AN EVALUATION BASED ON IgEAraafathNo ratings yet
- Primer: BronchiectasisDocument18 pagesPrimer: BronchiectasisAnanta Bryan Tohari WijayaNo ratings yet
- Orr 2019Document15 pagesOrr 2019abdi syahputraNo ratings yet
- Lag Aert 2017Document8 pagesLag Aert 2017abdi syahputraNo ratings yet
- Dyspareunia MacneillDocument14 pagesDyspareunia Macneillabdi syahputraNo ratings yet
- 192 2020 Article 4250Document7 pages192 2020 Article 4250abdi syahputraNo ratings yet
- Evaluation and Differential Diagnosis of DyspareuniaDocument10 pagesEvaluation and Differential Diagnosis of Dyspareuniaabdi syahputraNo ratings yet
- E836 FullDocument1 pageE836 Fullabdi syahputraNo ratings yet
- Asma 6Document39 pagesAsma 6abdi syahputraNo ratings yet
- Status EpilepticusDocument10 pagesStatus Epilepticusabdi syahputraNo ratings yet
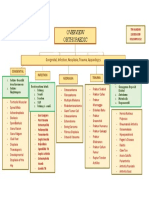
- Orthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesDocument1 pageOrthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesdinsNo ratings yet
- Ortho-Rheumatology Questions by DR - OkashaDocument136 pagesOrtho-Rheumatology Questions by DR - Okashamohammed okashaNo ratings yet
- Cumulative Lyme Disease (2013-2014) : Jayson Karuna Microbiology 1420-076 CenDocument2 pagesCumulative Lyme Disease (2013-2014) : Jayson Karuna Microbiology 1420-076 CenJayNo ratings yet
- MCN 2Document106 pagesMCN 2Nicole Dela TorreNo ratings yet
- Case Study NCPDocument6 pagesCase Study NCPEarl Joseph DezaNo ratings yet
- Seminar On Antigen-Antibody Reaction and Immunodeficiency DiseasesDocument28 pagesSeminar On Antigen-Antibody Reaction and Immunodeficiency DiseasesDr. Shiny KajalNo ratings yet
- Neurodevelopmental Disorders The History and Future of A Diagnostic ConceptDocument9 pagesNeurodevelopmental Disorders The History and Future of A Diagnostic Conceptmtkeniabianor_409003No ratings yet
- Record of Staff Toolbox Meeting TemplateDocument2 pagesRecord of Staff Toolbox Meeting TemplatemetaNo ratings yet
- De Thi Hoc Sinh Gioi Mon Tieng Anh Lop 9 Nam Hoc 2018 2019 So 12Document6 pagesDe Thi Hoc Sinh Gioi Mon Tieng Anh Lop 9 Nam Hoc 2018 2019 So 12Nhật VyNo ratings yet
- Gram Staining ProcedureDocument3 pagesGram Staining ProcedureCheska SillayuNo ratings yet
- Perdev 00Document2 pagesPerdev 00Nasser GementizaNo ratings yet
- Autosomal Dominant Polycystic Kidney DiseaseDocument11 pagesAutosomal Dominant Polycystic Kidney DiseaserutwickNo ratings yet
- Combining Scalp Acupuncture and Manual Therapy1Document26 pagesCombining Scalp Acupuncture and Manual Therapy1thesantorinimassageNo ratings yet
- An Investegatory Project ReportDocument17 pagesAn Investegatory Project ReportKhushi kapseNo ratings yet
- Deep Mycotic InfectionDocument5 pagesDeep Mycotic InfectionjalalfaizNo ratings yet
- Nosodes and Sarcodes - ClarkeDocument12 pagesNosodes and Sarcodes - Clarkemelos24No ratings yet
- Culture Bound: Illnesses in The PHDocument13 pagesCulture Bound: Illnesses in The PHMichael B.No ratings yet
- Human Cells Journey: Organ Syste MDocument7 pagesHuman Cells Journey: Organ Syste MArina CucuruzaNo ratings yet
- Hand Eczema TreatmentDocument9 pagesHand Eczema TreatmentCharcravorti AyatollahsNo ratings yet
- 50 bài tập Từ trái nghĩa Mức độ thông hiểu - phần 1Document13 pages50 bài tập Từ trái nghĩa Mức độ thông hiểu - phần 1huyentran2771996No ratings yet
- NSTP Notes - From ModuleDocument12 pagesNSTP Notes - From ModuleJulianna Jade Dela CruzNo ratings yet
- The Genetic Spectrum of Congenital OcularDocument12 pagesThe Genetic Spectrum of Congenital OcularKryssiaNo ratings yet
- REP8 Unit 8 Klucz OdpowiedziDocument4 pagesREP8 Unit 8 Klucz Odpowiedzipanna hanna19No ratings yet
- Nursing Case Presentation For A Patient With CABG: Subject: Medical Surgical Nursing-IIDocument10 pagesNursing Case Presentation For A Patient With CABG: Subject: Medical Surgical Nursing-IIanamika sharmaNo ratings yet
- Topic 11 - Certification and Legislation in Food and BeverageDocument35 pagesTopic 11 - Certification and Legislation in Food and BeverageEni Syafina RoslanNo ratings yet
- Final Graphic CommDocument46 pagesFinal Graphic Commatiq jalilNo ratings yet
- Ingles 4Document8 pagesIngles 4denisseNo ratings yet