Download as pdf or txt
You might also like
- HF-2900D User Manual RevJ.-20200811Document49 pagesHF-2900D User Manual RevJ.-20200811Mansour Mohamed Jawhar50% (4)
- Level 2 Hospital Research WorkDocument25 pagesLevel 2 Hospital Research WorkRamces Soliman100% (1)
- Level 2 Hospital Research WorkDocument25 pagesLevel 2 Hospital Research WorkKobe Manalansan PinedaNo ratings yet
- BMJ - Hospitals-Without-WallsDocument4 pagesBMJ - Hospitals-Without-WallsZaw Win SandiNo ratings yet
- The Handbook For Hospital Planning and DesigningDocument24 pagesThe Handbook For Hospital Planning and Designingarch.anupNo ratings yet
- What Does It Take To Run An ICU or Perioperative Medicine ServiceDocument19 pagesWhat Does It Take To Run An ICU or Perioperative Medicine Servicefriday ChitsongaNo ratings yet
- A Logistics Approach For Hospital Process Improvements: Jan VissersDocument35 pagesA Logistics Approach For Hospital Process Improvements: Jan VissersKarina WirajayaNo ratings yet
- Predicting Hospital Capacity and EfficiencyDocument9 pagesPredicting Hospital Capacity and EfficiencyManager HR Hijaz HospitalNo ratings yet
- Hand Off CommunicationDocument6 pagesHand Off CommunicationALELAW100% (1)
- DocDocument26 pagesDocprojectnewmail.2023No ratings yet
- Nursing Management Planning: Namgay Lham M.SC 2 Year KconDocument30 pagesNursing Management Planning: Namgay Lham M.SC 2 Year KconNamgay Lham100% (1)
- Team Base Research (Assignment)Document3 pagesTeam Base Research (Assignment)Frank IbiokNo ratings yet
- Austin Journal of Medical OncologyDocument4 pagesAustin Journal of Medical OncologyAustin Publishing GroupNo ratings yet
- Trilling Et Al. WHCM 2010Document6 pagesTrilling Et Al. WHCM 2010Gloom GomsNo ratings yet
- Health Care MGTDocument13 pagesHealth Care MGTRicha SinghNo ratings yet
- Hospital Planning: Changing Concepts: January 2003Document15 pagesHospital Planning: Changing Concepts: January 2003omaro1966No ratings yet
- Safe HandoversDocument7 pagesSafe HandoversRobMarvinNo ratings yet
- IUI Paper Q2. ADocument5 pagesIUI Paper Q2. AMuhammad Ammar GhaniNo ratings yet
- Ontologies For Location Based Services Quality Enhancement: The Case of Emergency ServicesDocument8 pagesOntologies For Location Based Services Quality Enhancement: The Case of Emergency Serviceskhairul_fajar_3No ratings yet
- A Review of Emergency and DisaDocument35 pagesA Review of Emergency and DisaMario G CassarNo ratings yet
- E O - M A C N P A C N P: Ffect of An Utcomes Anaged Pproach To Are of Euroscience Atients by Cute ARE Urse RactitionersDocument12 pagesE O - M A C N P A C N P: Ffect of An Utcomes Anaged Pproach To Are of Euroscience Atients by Cute ARE Urse RactitionersFathchur RohmanNo ratings yet
- A Patient Assignment Algorithm For Home Care Services: A Hertz and N LahrichiDocument15 pagesA Patient Assignment Algorithm For Home Care Services: A Hertz and N LahrichiJackson TakahashiNo ratings yet
- Toward An Ultrasound Curriculum For Critical Care Medicine PDFDocument15 pagesToward An Ultrasound Curriculum For Critical Care Medicine PDFBasilia CahuichNo ratings yet
- From Solution Shop' Model To Focused Factory' in Hospital Surgery: Increasing Care Value and PredictabilityDocument10 pagesFrom Solution Shop' Model To Focused Factory' in Hospital Surgery: Increasing Care Value and PredictabilityDhruv JindalNo ratings yet
- The Modern Radiology DepartmentDocument5 pagesThe Modern Radiology DepartmentBeautederm ZamboangaNo ratings yet
- LorraineMajor PosterDocument1 pageLorraineMajor PosterNHS Leadership AcademyNo ratings yet
- Providing Higher Value Care Through Population Health Management: What Is The Radiologist 'S Role?Document2 pagesProviding Higher Value Care Through Population Health Management: What Is The Radiologist 'S Role?Camilo SotomayorNo ratings yet
- Optimizing Patient Flow: Innovation Series 2003Document16 pagesOptimizing Patient Flow: Innovation Series 2003Jeff SavageNo ratings yet
- Simulation-Based Verification of Lean Improvement For Emergency Room ProcessDocument10 pagesSimulation-Based Verification of Lean Improvement For Emergency Room Processalvamu3354No ratings yet
- Hospital Planning: Changing Concepts: January 2003Document15 pagesHospital Planning: Changing Concepts: January 2003Hp JarnoNo ratings yet
- Hospital Design Considerations: Hurricane Katrina: The Public Health and Medical Response, Examined TheDocument32 pagesHospital Design Considerations: Hurricane Katrina: The Public Health and Medical Response, Examined ThePhorum PatelNo ratings yet
- June 2000/vol. 43, No. 6 COMMUNICATIONS OF THE ACMDocument8 pagesJune 2000/vol. 43, No. 6 COMMUNICATIONS OF THE ACMDavis PunjilaNo ratings yet
- Brown y Gallant - 2006 - Impacting Patient Outcomes Through Design AcuityDocument16 pagesBrown y Gallant - 2006 - Impacting Patient Outcomes Through Design AcuityAUSTREBERTO LOPEZ SANCHEZNo ratings yet
- Designing Collaborative Healthcare Technology For The Acute Care WorkflowDocument8 pagesDesigning Collaborative Healthcare Technology For The Acute Care WorkflowNUR AFIQAH SHAFIENo ratings yet
- FB Abb 61680000000Document6 pagesFB Abb 61680000000Iqbal HarzikyNo ratings yet
- Operation Management Project FinalDocument19 pagesOperation Management Project FinalmujeebkabapNo ratings yet
- ICU Without WallDocument6 pagesICU Without WallFahmi AuliaNo ratings yet
- Postoperative Care: Who Should Look After Patients Following Surgery?Document5 pagesPostoperative Care: Who Should Look After Patients Following Surgery?kishanm77No ratings yet
- 2011 - Application of Queuing Theory in Health CareDocument11 pages2011 - Application of Queuing Theory in Health CareAneri JainNo ratings yet
- Modeling and Simulation of Patient Flow in Hospitals For Resource UtilizationDocument10 pagesModeling and Simulation of Patient Flow in Hospitals For Resource UtilizationIndra GunawanNo ratings yet
- Hospitals PDFDocument30 pagesHospitals PDFBachir lejlifaNo ratings yet
- BMJ j4328 FullDocument5 pagesBMJ j4328 FullVanessa De AguasNo ratings yet
- Clinical Pathways and Nurses.Document3 pagesClinical Pathways and Nurses.Natukunda Dianah100% (2)
- Hall Flows Hospitals Chapter1text PDFDocument45 pagesHall Flows Hospitals Chapter1text PDFShin BoyceNo ratings yet
- 3 Technologies That Improve Patient Satisfaction ScoresDocument4 pages3 Technologies That Improve Patient Satisfaction ScoresWebi HapsaraNo ratings yet
- BI&DV Cia1Document13 pagesBI&DV Cia1ATHIRA DENNY 2127958No ratings yet
- Book Main 1Document135 pagesBook Main 1Meghana NavuluruNo ratings yet
- Simulation-Based Evaluation of Operating Room Management PoliciesDocument13 pagesSimulation-Based Evaluation of Operating Room Management Policiessriyanto ibsNo ratings yet
- 1 Paper EmergencyDepartmentPatientProcessFlowDocument6 pages1 Paper EmergencyDepartmentPatientProcessFlowandika fahruroziNo ratings yet
- Building A Clinical Cardiothoracic Surgical Program: A Multi-Institutional ModelDocument4 pagesBuilding A Clinical Cardiothoracic Surgical Program: A Multi-Institutional Modelnouha jhiderNo ratings yet
- Innovation Value and Reimbursement in Radiation AnDocument10 pagesInnovation Value and Reimbursement in Radiation AnGregorius HocevarNo ratings yet
- 1 Paper EmergencyDepartmentPatientProcessFlowDocument6 pages1 Paper EmergencyDepartmentPatientProcessFlowYey PahmateeNo ratings yet
- A Teamwork Approach: To Quality Patient Care in The Operating RoomDocument14 pagesA Teamwork Approach: To Quality Patient Care in The Operating Roomjosephabram051590No ratings yet
- Jurnal 1 RimaDocument19 pagesJurnal 1 RimanellyNo ratings yet
- Journal of Biomedical Informatics: Jens Meier, Andreas Dietz, Andreas Boehm, Thomas NeumuthDocument12 pagesJournal of Biomedical Informatics: Jens Meier, Andreas Dietz, Andreas Boehm, Thomas NeumuthTanvin AyatNo ratings yet
- ICU Nurse PrivilegesDocument35 pagesICU Nurse PrivilegesSarah Alberto100% (4)
- Clinical Decision Support SystemDocument13 pagesClinical Decision Support SystemUdit Kheterpal100% (1)
- Stochastic Programming For Outpatient Scheduling With Flexible Inpatient Exam AccommodationDocument23 pagesStochastic Programming For Outpatient Scheduling With Flexible Inpatient Exam Accommodationnancy.vargasNo ratings yet
- Orp 3 CombDocument8 pagesOrp 3 CombControl de Equipos InternosNo ratings yet
- Business Analytics: Hospital - Facilities Management and Utilisation For A 100 Bedded HospitalDocument44 pagesBusiness Analytics: Hospital - Facilities Management and Utilisation For A 100 Bedded HospitalAswani AbayanNo ratings yet
- Emergent Vascular Access: A Guide for Healthcare ProfessionalsFrom EverandEmergent Vascular Access: A Guide for Healthcare ProfessionalsJames H. PaxtonNo ratings yet
- CHAPTER 2 Literature ReviewDocument15 pagesCHAPTER 2 Literature ReviewNSHIZIRUNGU OLIVIERNo ratings yet
- Daniel Hospital ProjectDocument9 pagesDaniel Hospital ProjectNSHIZIRUNGU OLIVIERNo ratings yet
- MUNEZERODocument9 pagesMUNEZERONSHIZIRUNGU OLIVIERNo ratings yet
- Modern Village 1Document7 pagesModern Village 1NSHIZIRUNGU OLIVIERNo ratings yet
- Gakwisi Eris English Assignment 3Document1 pageGakwisi Eris English Assignment 3NSHIZIRUNGU OLIVIERNo ratings yet
- BLTNDocument3 pagesBLTNNSHIZIRUNGU OLIVIERNo ratings yet
- Project Proposal On Design of A Modern HDocument87 pagesProject Proposal On Design of A Modern HNSHIZIRUNGU OLIVIERNo ratings yet
- Na Wang and Corresponding Author: Jinguo Wang: The Design Trend of Modern Hospital ArchitectureDocument3 pagesNa Wang and Corresponding Author: Jinguo Wang: The Design Trend of Modern Hospital ArchitectureNSHIZIRUNGU OLIVIERNo ratings yet
- Minimally Invasive Management of Uterine Fibroids Role of Transvaginal Radiofrequency AblationDocument5 pagesMinimally Invasive Management of Uterine Fibroids Role of Transvaginal Radiofrequency AblationHerald Scholarly Open AccessNo ratings yet
- ISPNO 2022 - Impact of The COVID-19 Pandemic On 30-Day Mortality and Unplanned Reoperation Rates For Pediatric Central Nervous System TumorsDocument2 pagesISPNO 2022 - Impact of The COVID-19 Pandemic On 30-Day Mortality and Unplanned Reoperation Rates For Pediatric Central Nervous System TumorsDiana SanchezNo ratings yet
- Uts Bahasa InggrisDocument8 pagesUts Bahasa InggrisBirat Atma DewaNo ratings yet
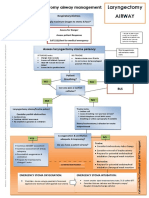
- Laryngectomy Airway: Emergency Tracheostomy Airway ManagementDocument1 pageLaryngectomy Airway: Emergency Tracheostomy Airway ManagementDana IlieNo ratings yet
- Mechanics To Enhance EstheticsDocument21 pagesMechanics To Enhance EstheticsTolly CNo ratings yet
- Conflicting Dermatome MapsDocument9 pagesConflicting Dermatome MapsAntonio ValentinoNo ratings yet
- Class X Eng - Worksheet Ch-1 (Book2) May 08,2020Document5 pagesClass X Eng - Worksheet Ch-1 (Book2) May 08,2020ANANYA CHUGH100% (1)
- CA OesophagusDocument47 pagesCA OesophagusAnsif KNo ratings yet
- Mobile Operating Tables For All Surgical ApplicationsDocument13 pagesMobile Operating Tables For All Surgical Applicationsibrahim hashimNo ratings yet
- C) Asa Iii: D) Left Lateral PositionDocument6 pagesC) Asa Iii: D) Left Lateral Positionmcshah19No ratings yet
- Post-Operative Instructions: Laparoscopic CholecystectomyDocument2 pagesPost-Operative Instructions: Laparoscopic Cholecystectomyrizwan234No ratings yet
- Truncus Arteriosus: J F. K D C. FDocument5 pagesTruncus Arteriosus: J F. K D C. FVictor PazNo ratings yet
- Development and Validation of A Bovine Castration Model and RubricDocument9 pagesDevelopment and Validation of A Bovine Castration Model and RubricMARIA CAMILA MENDEZ ARDILANo ratings yet
- Sistrunk Operation ArticleDocument4 pagesSistrunk Operation Articleআবু আব্দুল্লাহ শাদীদNo ratings yet
- KMM & Hyd Ehs Hospitals ListDocument5 pagesKMM & Hyd Ehs Hospitals Listraj kNo ratings yet
- SOP For Dermatologist For DOH PuplicationDocument13 pagesSOP For Dermatologist For DOH Puplicationhitham shehataNo ratings yet
- Central Bicol Masterlist Sort AddressDocument6 pagesCentral Bicol Masterlist Sort Addresskentclark03No ratings yet
- InnoFit® Lodestar Plus Kit (LR)Document12 pagesInnoFit® Lodestar Plus Kit (LR)Vishruti PobaruNo ratings yet
- Rehabilitation EngineeringDocument28 pagesRehabilitation EngineeringMuhammad MoazzamNo ratings yet
- Code Yellow - GnopDocument70 pagesCode Yellow - GnopLinda andayaniNo ratings yet
- Elbow Dislocation DR - Ahmed AbdaliDocument28 pagesElbow Dislocation DR - Ahmed Abdaliabbassi mohammedNo ratings yet
- GORDONS 11 HEALTH FUNCTIONAL PATTERNS DraftDocument8 pagesGORDONS 11 HEALTH FUNCTIONAL PATTERNS DraftJessa C. BorjaNo ratings yet
- Oral and Maxillofacial Osteosarcoma in Dogs A ReviDocument13 pagesOral and Maxillofacial Osteosarcoma in Dogs A ReviBim ShiddiNo ratings yet
- 10 14309@ctg 0000000000000156 PDFDocument6 pages10 14309@ctg 0000000000000156 PDFWebo WeboNo ratings yet
- The Cat With LUTD A Surgeons PrespectiveDocument3 pagesThe Cat With LUTD A Surgeons PrespectiveCabinet VeterinarNo ratings yet
- Catalog Nội Soi Khớp - RWDocument128 pagesCatalog Nội Soi Khớp - RWNguyên Phương Chi PhạmNo ratings yet
- Burn-Medical and Surgical ManagementDocument6 pagesBurn-Medical and Surgical ManagementCristina L. JaysonNo ratings yet
- Marinduque CS InstrumentsDocument6 pagesMarinduque CS InstrumentsJAMES ROD MARINDUQUENo ratings yet
- Vas Uhc Sample Letter Medical NecessityDocument5 pagesVas Uhc Sample Letter Medical NecessityJasonNo ratings yet