Professional Documents
Culture Documents
Antiviral Treatment Failures After Transplantation
Antiviral Treatment Failures After Transplantation
Uploaded by
Rogelio MoscosoOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Antiviral Treatment Failures After Transplantation
Antiviral Treatment Failures After Transplantation
Uploaded by
Rogelio MoscosoCopyright:
Available Formats
Case Report
Antiviral Treatment Failures After Transplantation of
Organs From Donors With Hepatitis C Infection: A Report
of 4 Cases
Julie M. Steinbrink, Shanti Narayanasamy, Cameron R. Wolfe, Eileen Maziarz, Jennifer Byrns, Jennifer J. Kiser,
and Susanna Naggie
The transplantation of organs from donors with hepatitis C virus (HCV) infection into uninfected re- Complete author and article
cipients has expanded the available organ donor pool. With the advancement of direct-acting antivirals information provided before
references.
(DAAs), high rates of cure among transplant recipients are possible. Although DAAs are highly
effective, treatment failure can occur following an appropriate 12-week course of a pan-genotypic Am J Kidney Dis.
regimen. Here we describe 4 kidney transplant recipients of organs from donors with HCV infection 82(3):368-372. Published
online February 4, 2023.
(3 with genotype 3, 1 genotype 1a) in whom first-line DAA treatment with either glecaprevir-
pibrentasvir or sofosbuvir-velpatasvir was unsuccessful, started 22-35 days after the day of trans- doi: 10.1053/
plantation. All ultimately achieved sustained virologic response with second- or third-line therapy. j.ajkd.2022.12.006
Post-treatment resistance-associated substitutions were tested and noted to be present in 2 cases.
Additionally, antiviral levels were assessed in 2 cases and found to be therapeutic in each. This article
explores possible reasons for treatment failure, including medication interactions, bariatric surgery, viral
dynamics, and drug resistance.
© 2023 The Authors. Published by Elsevier Inc. on behalf of the National Kidney Foundation, Inc. This is an open access article
under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction daily replaced omeprazole 20 mg daily to avoid velpatasvir
interaction with proton pump inhibitors (PPIs).3 At end of
Treatment of hepatitis C virus (HCV) infection now results
therapy, HCV RNA was undetectable, though was subse-
in high cure rates owing to the availability of direct-acting
quently quantifiable on PTD 136. Famotidine was stopped
antivirals (DAAs). Early studies suggesting safety and effi-
and she then completed 12 weeks of sofosbuvir/velpa-
cacy of DAAs among transplant recipients have prompted
tasvir/voxilaprevir (400 mg/100 mg/100 mg daily). HCV
medical centers to transplant organs from donors with
RNA became undetectable with sustained virologic
HCV infection into uninfected recipients.1,2 While HCV
response at 12 weeks (SVR12). Resistance testing and drug
treatment guidelines are established for chronic HCV,
levels were not monitored.
transplant recipients with acute infection remain a unique,
diverse, and understudied population. We present 4 cases
Case 2
in which guideline-driven DAA therapy failed in recipients
of kidney transplants from HCV RNA+ donors. These cases A 66-year-old male patient who underwent DDKT for ESRD
highlight the complexity of HCV-RNA+ transplantation, secondary to diabetes, with a history of biliopancreatic
potential predictors of failure, and approaches to salvage diversion duodenal switch, was treated initially with 12
therapy. weeks of sofosbuvir/velpatasvir (400 mg/100 mg daily)
starting on PTD 28 for a pretreatment HCV RNA of 2,228
IU/mL, genotype 3. HCV RNA remained undetectable
Case Report through end of therapy but was subsequently quantifiable
The clinical characteristics of the 4 patients and their on PTD 123. Resistance-associated substitution (RAS)
clinical courses are depicted in Table 1 and Fig 1, testing of the NS5A gene demonstrated S62T and Y93H
respectively. All patients were administered DAAs as part of substitutions. (Resistance was only checked after DAA
clinical care, and this work was ruled as institutional re- exposure, and was not checked at baseline.) He subse-
view board exempt (Pro00112261). quently completed 12 weeks of sofosbuvir/velpatasvir/
voxilaprevir (400 mg/100 mg/100 mg daily), and HCV
Case 1 RNA was undetectable at end of therapy, but was again
A 68-year-old female patient, who underwent deceased subsequently quantifiable on PTD 250. He then completed
donor kidney transplantation (DDKT) for end-stage renal glecaprevir/pibrentasvir/sofosbuvir (300 mg/120 mg/
disease (ESRD) owing to polycystic kidney disease, was 400 mg daily) + ribavirin 200 mg twice daily for 24 weeks
treated initially with 12 weeks of sofosbuvir/velpatasvir and ultimately achieved SVR12. There was concern that he
(400 mg/100 mg daily, respectively) starting on post- had inadequate gastric absorption; however, plasma levels
transplant day (PTD) 28 for a pretreatment HCV RNA of of sofosbuvir and the active form of sofosbuvir circulating in
7,536,540 IU/mL, genotype 1a. Famotidine 20 mg twice plasma, GS-331007, were assessed under institutional
368 AJKD Vol 82 | Iss 3 | September 2023
Steinbrink et al
review board–approved protocol Pro00106012 while on
glecaprevir/pibrentasvir/sofosbuvir + ribavirin. Sofosbuvir
checked
checked
Y93H*
Y93Ha
A30K,
S62L,
S62T,
Never
Never
and GS-331007 levels were 351 ng/mL and 1,506 ng/mL,
RAS respectively, approximately 2-3 hours post dos-
e—consistent with adequate absorption.3
Thymoglobulin
Case 3
Induction
A 67-year-old male patient, who underwent DDKT for
ESRD owing to diabetes and a history of Roux-en-Y gastric
Yes
Yes
Yes
Yes
bypass, was treated initially with glecaprevir/pibrentasvir
(300 mg/120 mg daily) on PTD 22 for a pretreatment
duodenal switch
HCV RNA of >100 million IU/mL, genotype 3, while
Biliopancreatic
Laparoscopic
diversion w/
continuing omeprazole 40 mg daily. However, after initial
Roux-en Y
Bariatric
Surgery
reduction in HCV RNA, there was an increase on PTD 62
and glecaprevir/pibrentasvir was stopped. NS5a RAS
No
No
testing demonstrated A30K, S62L, and Y93H substitutions.
Omeprazole was discontinued, and he completed 24
Treatment stopped at 45 days, earlier than initially planned 84-day course, owing to treatment failure. All other DAA regimens were completed in full as planned.
Suppressor
H2 blocker
weeks of sofosbuvir/velpatasvir/voxilaprevir (400 mg/
inhibitor
100 mg/100 mg daily), with which he achieved SVR12.
Proton
pump
None
None
Acid
While on sofosbuvir/velpatasvir/voxilaprevir, sofosbuvir
and GS-331007 in plasma were below the limit of quan-
tification and 705 ng/mL, respectively, and velpatasvir in
Adherence
plasma was 40.8 ng/mL, 21 hours postdose. These con-
reported
centrations are consistent with historical data and are
100%
100%
100%
100%
Abbreviations: DAA, direct-acting antiviral; HCV, hepatitis C virus; POD, postoperative day; RAS, resistance-associated substitutions.
Self-
believed to be therapeutic.3
Day of DAA
Case 4
transplant
Initiation
A 44-year-old male patient who underwent DDKT for
POD 28
POD 22
POD 35
PD 28
ESRD owing to hypertension (same donor as in case 3) was
Post-
treated initially with 12 weeks of glecaprevir/pibrentasvir
(300 mg/120 mg daily) on PTD 35 for a pretreatment
2. Sofosbuvir-velpatasvir-voxilaprevir × 168
HCV RNA of 409,220 IU/mL, genotype 3. HCV viral load
3. Glecaprevir-pibrentasvir + sofosbuvir +
2. Sofosbuvir-velpatasvir-voxilaprevir × 84
2. Sofosbuvir-velpatasvir-voxilaprevir × 84
became undetectable by end of therapy and subsequently
1. Glecaprevir-pibrentasvir × 45 daysb
2. Sofosbuvir-velpatasvir-voxilaprevir +
1. Glecaprevir-pibrentasvir × 84 days
quantifiable on PTD 133. He completed a 24-week course
1. Sofosbuvir-velpatasvir × 84 days
1. Sofosbuvir-velpatasvir × 84 days
HCV Regimen for Treatment and
of sofosbuvir/velpatasvir/voxilaprevir (400 mg/100 mg/
100 mg daily) + ribavirin 600 mg daily, with which he
Table 1. Clinical Characteristics of HCV Kidney Transplant Cases
achieved SVR12. Resistance testing and drug levels were
not completed for this patient.
ribavirin × 168 days
ribavirin × 168 days
Discussion
Retreatment
Transplantation of organs from donors with HCV
RAS not checked at baseline, checked after treatment failure.
infection has greatly increased organ availability. Though
achieving suppressed virus during treatment but expe-
days
days
days
riencing viral recurrence post-treatment (ie, a relapse) is
uncommon,1,2,4 not all patients achieve HCV cure with
DAA (IU/mL)
HCV Prior to
100,000,000
initial therapy. Although it is difficult to determine the
55,533,881
1,248,636
(>8.0 log)
exact cause of treatment failure, there are baseline
409,220
(6.1 log)
(5.6 log)
(7.7 log)
characteristics that have been identified as predictors of
poor response, even in the DAA era, including high
pretreatment HCV RNA, concomitant drug-drug in-
Genotype
teractions, bariatric surgery, HCV genotype, and pres-
ence of RAS. In the peritransplant setting there are likely
others, including timing of DAA initiation and induction
1a
immunosuppression. In the cases described here, the
Case
patients had various combinations of these negative
predictors.
1
b
a
AJKD Vol 82 | Iss 3 | September 2023 369
Steinbrink et al
Commenced
HCV RNA 7,536,540 IU/mL HCV RNA undetectable SOF/VEL/VOX
Genotype 1a 12 weeks
Commenced EOT HCV RNA 115,000 IU/mL EOT
Transplant SVR12
SOF/VEL 12 weeks HCV RNA undetectable Famotidine ceased HCV RNA undetectable
CASE 1
Day 0 Day 5 Day 28 Day 79 Day 112 Day 136 Day 154 Day 238 Day 322
HCV RNA 2,228 IU/mL HCV RNA <15 IU/mL Commenced HCV RNA 22,784
Genotype 3 HCV RNA undetectable detectable SOF/VEL/VOX IU/mL
12 weeks
HCV RNA Commenced
Commenced EOT EOT GLE/PIB/SOF/RBV EOT
581,840 SVR12
Transplant SOF/VEL 12 weeks HCV RNA undetectable HCV RNA undetectable 24 weeks HCV RNA undetectable
IU/mL
CASE 2
Day 0 Day 5 Day 28 Day 67 Day 112 Day 123 Day 138 Day 148 Day 232 Day 250 Day 272 Day 440 Day 524
HCV RNA 144,273 IU/mL HCV RNA
Genotype 3 41,600,000 IU/mL
HCV RNA Commenced
>100 million IU/mL HCV RNA GLE/PIB EOT
SOF/VEL/VOX 24 weeks
Transplant Commenced 13,100,867 IU/mL ceased HCV RNA undetectable SVR12
Omeprazole ceased HCV RNA undetectable
GLE/PIB 12 weeks
CASE 3
Day 0 Day 5 Day 22 Day 55 Day 62 Day 67 Day 108 Day 162 Day 276 Day 360
HCV RNA 52,438 IU/mL
HCV RNA 409,220 IU/mL HCV RNA undetectable Commenced SOF/VEL/VOX/RBV
Genotype 3 24 weeks SVR12
EOT HCV RNA HCV RNA HCV RNA EOT HCV RNA
Commenced undetectable
Transplant undetectable 233 IU/mL undetectable
GLE/PIB 12 weeks
CASE 4
Day 0 Day 5 Day 35 Day 59 Day 119 Day 133 Day 143 Day 163 Day 311 Day 395
DAYS FOLLOWING TRANSPLANTATION
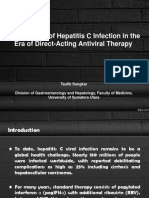
Figure 1. Clinical course timeline of all described kidney transplant cases, including time relative to transplant and initial and sub-
sequent antiviral regimen(s), through final sustained virologic response 12 weeks post treatment. Abbreviations: EOT, end of treat-
ment; GLE, glecaprevir; HCV RNA, hepatitis C viral load; PIB, pibrentasvir; RBV, ribavirin; SOF, sofosbuvir; SVR12, sustained
virologic response 12 weeks post treatment; VEL, velpatasvir; VOX, voxilaprevir.
Adequate drug absorption is imperative to treatment drug levels from their initial therapy. Unfortunately, there
success. All included patients reported 100% DAA adher- are no commercially available assays for DAA therapeutic
ence, confirmed biweekly with Transplant Pharmacy. Acid drug monitoring.
suppressants are commonly used post-transplant; however, Timing of DAAs may also impact virologic response in
PPIs have a severe interaction with velpatasvir, reducing this unique setting. All described patients started DAAs
area under the curve (AUC) concentrations by 26%-55% within 1 month post-transplant, while other centers
owing to decreased solubility at increased gastric pH.3 initiate DAAs pre-emptively within 1 week post-trans-
Histamine-blocking antacids (eg, famotidine) have a plant.1,2,4 The delayed DAA initiation may result in higher
moderate interaction with velpatasvir, decreasing AUC levels of pretreatment HCV RNA, which, although less
concentrations by approximately 15%.3 The interaction predictive of treatment outcomes with newer DAAs, has
with acid suppressants and glecaprevir/pibrentasvir is less been a predictor of treatment response with early DAA
clear. PPIs can decrease glecaprevir AUC by 29% and therapies. All the cases described in this report had high
maximum serum concentration by 22%, but evidence of initial HCV RNA levels (ranging from 409,000 to >100
treatment failure in clinical practice is lacking.5,6 million IU/mL). This is in contrast to other HCV transplant
There are little data on the effect of bariatric surgery on studies, such as the MYTHIC trial, where treatment was
DAA absorption. Available literature describes decreased started within the first week post-transplant, and median
systemic drug levels of some DAAs.7 This impact on drug peak HCV RNA was approximately only 2,000 IU/mL.4
levels may be attributable to distorted anatomy (such as Several barriers to a pre-emptive approach exist,
malabsorption owing to decreased gastric volume or sur- including administration/absorption for patients unable to
gical intestinal alteration impacting the digestive process) take medications by mouth (particularly with thoracic
leading to increased incidence of failure.7-11 The type of transplant), higher incidence of drug-drug interactions
surgery may impact the degree of absorption and should early in the postoperative period, and financial burden of
be considered before initiating treatment. In our study, 2 drug cost and securing medications while hospitalized.
patients had a history of bariatric surgery, with both Induction immunosuppression is an additional potential
restrictive and absorptive elements. Although both patients contributing factor to treatment failure. At our institution,
had drug levels in their final (curative) courses of therapy induction immunosuppression for kidney transplantation
consistent with adequate drug exposure, we do not have typically consists of solumedrol. Thymoglobulin is used
370 AJKD Vol 82 | Iss 3 | September 2023
Steinbrink et al
for higher-risk cases or delayed graft function. For context, Address for Correspondence: Julie Steinbrink, MD, #150 Hanes
of 106 recipients of kidneys from donors with HCV House, Duke University Medical Center, 315 Trent Dr, Durham,
NC 27710. Email: julie.steinbrink@duke.edu
infection at our institution, 40 received thymoglobulin
induction; those with steroid induction alone did not Support: Dr Steinbrink was funded by NIH/NIAID T32 grant
AI100851. The funders had no role in defining the content of the
develop treatment failure and were not described in this manuscript.
manuscript. However, the treatment failures in these 4
Financial Disclosure: The authors declare that they have no
cases required thymoglobulin along with routine relevant financial interests.
maintenance immunosuppression with tacrolimus, myco- Patient Protections: The authors declare that they have obtained
phenolate, and prednisone. This high degree of immu- written consent from each patient reported in this article for
nosuppression could theoretically impact viral clearance. publication of the information about him/her that appears within
However, in the HCV-transplantation literature, thymo- this case report.
globulin induction has been used without evidence of Peer Review: Received August 17, 2022. Evaluated by 2 external
higher treatment failure.1,2,12 peer reviewers, with direct editorial input from an Associate Editor
and a Deputy Editor. Accepted in revised form December 10, 2022.
Of the cases in this report, 1 was genotype 1a (histor-
ically most prevalent in the United States), while the rest
were genotype 3.13 Genotype 3 is increasingly seen in
acute HCV, particularly with injection drug use, and thus References
increasingly seen in organs from donors with HCV infec- 1. Reese PP, Abt PL, Blumberg EA, et al. Twelve-month outcomes
tion. Genotype 3 is associated with a higher incidence of after transplant of hepatitis C-infected kidneys into uninfected
virologic failure, particularly when grouped with other recipients: a single-group trial. Ann Intern Med. 2018;169(5):
negative baseline predictors. Additionally, pretreatment 273-281.
2. Durand CM, Bowring MG, Brown DM, et al. Direct-acting
HCV resistance testing is not standard practice for all
antiviral prophylaxis in kidney transplantation from hepatitis C
regimens or patients. Although many transplant recipients virus-infected donors to noninfected recipients: an open-label
are DAA naı̈ve, often the donor treatment status is nonrandomized trial. Ann Intern Med. 2018;168(8):533-540.
unknown—prior DAA failure results in treatment- 3. Epclusa (sofosbuvir and velpatasvir) [prescribing information].
emergent RASs the majority of the time.14 Two patients Foster City, CA: Gilead Sciences Inc; Revised: April 2022.
described here were found to have a post-treatment relapse Accessed December 2022.
Y93H mutation, which has been associated with decreased 4. Sise ME, Goldberg DS, Kort JJ, et al. Multicenter Study to
Transplant Hepatitis C-Infected Kidneys (MYTHIC): an open-
SVR rates to sofosbuvir/velpatasvir in patients with geno-
label study of combined glecaprevir and pibrentasvir to treat
type 3 infection (84% vs 97%).15 No patient had evidence recipients of transplanted kidneys from deceased donors with
of liver dysfunction during relapse. hepatitis C virus infection. J Am Soc Nephrol. 2020;31(11):
We acknowledge that this is a small number of cases, 2678-2687.
with only 4 patients described. Additionally, postrelapse 5. Mavyret (glecaprevir and pibrentasvir) [prescribing informa-
RAS testing and drug levels were not systematically tion]. North Chicago, IL: AbbVie Inc; December 2021.
checked and thus are not available for 2 of the 4 cases. 6. Flamm S, Reddy KR, Zadeikis N, et al. Efficacy and pharma-
cokinetics of glecaprevir and pibrentasvir with concurrent use
In summary, organs from donors with HCV infection
of acid-reducing agents in patients with chronic HCV infection.
are a safe and viable option for organ transplantation, but Clin Gastroenterol Hepatol. 2019;17(3):527-535.e526.
there are many factors to consider when a transplant 7. Smolders EJ, Willemse SB, El-Sherif O, Khoo S, Burger DM.
recipient experiences treatment failure. Transplant pro- The observed effect of gastric bypass surgery on direct-acting
viders must be aware of potential barriers to cure and antiviral treatment: a case report. Ann Hepatol. 2018;17(3):
attempt to optimize the initial treatment course, be vigilant 525-529.
about monitoring for failure, and be alert to antiviral 8. Tow CY, Reinus JF. Ineffective absorption? Failure of direct-
acting therapy for chronic hepatitis C in cirrhotic patients
salvage options.
with Roux-en-Y gastric bypass. J Investig Med High Impact
Case Rep. 2019;7:2324709619858127.
Article Information 9. Asselah T, Kowdley KV, Zadeikis N, et al. Efficacy of glecap-
Authors’ Full Names and Academic Degrees: Julie M. Steinbrink, revir/pibrentasvir for 8 or 12 weeks in patients with hepatitis C
MD, Shanti Narayanasamy, MBBS, Cameron R. Wolfe, MBBS, virus genotype 2, 4, 5, or 6 infection without cirrhosis. Clin
Eileen Maziarz, MD, Jennifer Byrns, PharmD, Jennifer J. Kiser, Gastroenterol Hepatol. 2018;16(3):417-426.
PharmD, PhD, and Susanna Naggie, MD. 10. Naganuma A, Sato K, Fukuchi T, et al. Successful prolonged
Authors’ Affiliations: Division of Infectious Diseases, Duke treatment of glecaprevir/pibrentasvir for chronic hepatitis C
University School of Medicine, Durham, North Carolina (JMS, SN, patient with treatment failure after 8-week therapy: a case
CRW, EM, SN); Department of Pharmacy, Duke University Medical report. Clin J Gastroenterol. 2019;12(6):592-597.
Center, Durham, North Carolina (JB); Department of 11. Hupa KL, Deterding K, Port K, et al. Stomach reduction or
Pharmaceutical Sciences, University of Colorado Anschutz gastric bypass as risk factor for treatment failure after DAA
Medical Campus, Aurora, Colorado (JJK); and Section of therapy for hepatitis C? J Hepatol. 2018;68(4):851-853.
Infectious Diseases, Durham Veterans Affairs Health Care System, 12. Molnar MZ, Nair S, Cseprekal O, et al. Transplantation of kid-
Durham, North Carolina (SN). neys from hepatitis C-infected donors to hepatitis C-negative
AJKD Vol 82 | Iss 3 | September 2023 371
Steinbrink et al
recipients: single center experience. Am J Transplant. 14. Wyles DL, Luetkemeyer AF. Understanding hepatitis C virus
2019;19(11):3046-3057. drug resistance: clinical implications for current and future
13. Reau N, Sulkowski MS, Thomas E, et al. Epidemiology and regimens. Top Antivir Med. 2017;25(3):103-109.
clinical characteristics of individuals with hepatitis C virus 15. Foster GR, Afdhal N, Roberts SK, et al. Sofosbuvir and vel-
infection in the United States, 2017-2019. Adv Ther. patasvir for HCV genotype 2 and 3 infection. N Engl J Med.
2021;38(12):5777-5790. 2015;373(27):2608-2617.
372 AJKD Vol 82 | Iss 3 | September 2023
You might also like
- Kikuchi 2018Document4 pagesKikuchi 2018aimanshahnaz285No ratings yet
- Sofosbuvir and Velpatasvir For HCV in Patients With Decompensated CirrhosisDocument12 pagesSofosbuvir and Velpatasvir For HCV in Patients With Decompensated CirrhosisanaNo ratings yet
- Success of (NS5BNS5A Inhibitors) SofosbuvirVelpatasvir in Management Hepatitis C Studied Tertiary Care Healthcare in Rawalpindi, PakistanDocument6 pagesSuccess of (NS5BNS5A Inhibitors) SofosbuvirVelpatasvir in Management Hepatitis C Studied Tertiary Care Healthcare in Rawalpindi, PakistanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pharmacological Management of Hepatitis CDocument62 pagesPharmacological Management of Hepatitis CWei HangNo ratings yet
- Bioscientific Review (BSR)Document9 pagesBioscientific Review (BSR)UMT JournalsNo ratings yet
- Prevalence of Hepatitis C Virus Infection And.10Document6 pagesPrevalence of Hepatitis C Virus Infection And.10aimanshahnaz285No ratings yet
- PIIS1542356520309253Document10 pagesPIIS1542356520309253pooja pandeyNo ratings yet
- Jurnal Ebm PDFDocument10 pagesJurnal Ebm PDFagustin488No ratings yet
- Servefile CFMDocument9 pagesServefile CFMLUIS ALFREDO SALGADO FLORESNo ratings yet
- Sofosbuvir For Previously Untreated Chronic Hepatitis C InfectionDocument10 pagesSofosbuvir For Previously Untreated Chronic Hepatitis C InfectionSitta Grewo LiandarNo ratings yet
- 2017 HepatologyDocument148 pages2017 HepatologyrdLuis1No ratings yet
- Remdesivir in Patients With Acute or Chronic Kidney Disease and COVID-19Document3 pagesRemdesivir in Patients With Acute or Chronic Kidney Disease and COVID-19lucianarottyNo ratings yet
- Bedaquiline Article Multidrug-Resistant TuberculosisDocument10 pagesBedaquiline Article Multidrug-Resistant TuberculosisAlvaro MuñozNo ratings yet
- Oral Presentations: Viral Hepatitis C: TherapyDocument2 pagesOral Presentations: Viral Hepatitis C: TherapyWilson WqaNo ratings yet
- Emerging Therapies in Hepatitis C. Dawn of The Era of The Direct Acting Antivirals (2011)Document14 pagesEmerging Therapies in Hepatitis C. Dawn of The Era of The Direct Acting Antivirals (2011)drheayNo ratings yet
- S1.2 PPT DR - Taufik SungkarDocument32 pagesS1.2 PPT DR - Taufik SungkarMuhammadIkhsanFadillahNo ratings yet
- Tropical Doctor YayınımızDocument6 pagesTropical Doctor Yayınımıztayibe balNo ratings yet
- Chronic Hepatitis BDocument5 pagesChronic Hepatitis BMurat HessesNo ratings yet
- Multidrug-Resistant Tuberculosis and Culture Conversion With BedaquilineDocument10 pagesMultidrug-Resistant Tuberculosis and Culture Conversion With BedaquilineSteven RichardNo ratings yet
- ) - Successful Treatment of Chronic Norovirus Gastroenteritis With Nitazoxanide in A Pediatric Kidney Transplant RecipientDocument4 pages) - Successful Treatment of Chronic Norovirus Gastroenteritis With Nitazoxanide in A Pediatric Kidney Transplant Recipientnutrimed82No ratings yet
- Computational Drug Repurposing Study Elucidating Simultaneous Inhibition of Entry and Replication of Novel Corona Virus by GrazoprevirDocument11 pagesComputational Drug Repurposing Study Elucidating Simultaneous Inhibition of Entry and Replication of Novel Corona Virus by GrazoprevirAlok JainNo ratings yet
- Final-HCV Guidelines Treatment 2018Document37 pagesFinal-HCV Guidelines Treatment 2018Joriza TamayoNo ratings yet
- 15 High Rate of Early Virological FailureDocument9 pages15 High Rate of Early Virological Failuredanayanto sumbungNo ratings yet
- AnticoagulantesDocument9 pagesAnticoagulantesjenifferferradaNo ratings yet
- Efficacy and Safety of Daclatasvir Plus Sofosbuvir For Treatment-Naïve and Treatment-Experienced Egyptian Patients With Hepatitis C Virus InfectionDocument13 pagesEfficacy and Safety of Daclatasvir Plus Sofosbuvir For Treatment-Naïve and Treatment-Experienced Egyptian Patients With Hepatitis C Virus InfectionIslam NasrNo ratings yet
- Sofosbuvir For Previously Untreated Chronic Hepatitis C InfectionDocument23 pagesSofosbuvir For Previously Untreated Chronic Hepatitis C InfectionalfianfirdausNo ratings yet
- THERAPY RIVER TrialDocument10 pagesTHERAPY RIVER Trialfretzie enguitoNo ratings yet
- Farmakokinetika RemdesivirDocument11 pagesFarmakokinetika RemdesivirAlfiana NovitaNo ratings yet
- Rivaroxaban in Patients With Atrial Fibrillation and A Bioprosthetic Mitral ValveDocument11 pagesRivaroxaban in Patients With Atrial Fibrillation and A Bioprosthetic Mitral ValveJuan JoseNo ratings yet
- Ferder 2010Document6 pagesFerder 2010Soshi DaysNo ratings yet
- Hep C TreatmentDocument40 pagesHep C Treatmentf9r8fzgdh6No ratings yet
- nejmoa1306218Document11 pagesnejmoa1306218reumatoccsNo ratings yet
- LENACAPAVIRDocument11 pagesLENACAPAVIRAhmed ElgenaidyNo ratings yet
- Hep B RekomendasiDocument5 pagesHep B RekomendasiKevin JawanNo ratings yet
- Direct anti-HCV Agents: Acta Pharmaceutica Sinica BDocument6 pagesDirect anti-HCV Agents: Acta Pharmaceutica Sinica BAnonymous qyRlxhNo ratings yet
- Caspofungin Population Pharmacokinetics in Critically Ill Patients Undergoing Continuous Veno-Venous Haemofiltration or HaemodiafiltrationDocument12 pagesCaspofungin Population Pharmacokinetics in Critically Ill Patients Undergoing Continuous Veno-Venous Haemofiltration or HaemodiafiltrationNguyễn LongNo ratings yet
- Divalproate AcidvalproateDocument10 pagesDivalproate AcidvalproateLuiz BelattoNo ratings yet
- TMP 8 FA6Document6 pagesTMP 8 FA6FrontiersNo ratings yet
- 52 2021-RAD-HCV RNA Sofosbuvir and InterferonDocument6 pages52 2021-RAD-HCV RNA Sofosbuvir and InterferonDr. Taha NazirNo ratings yet
- HCV Treatment RevolutionDocument3 pagesHCV Treatment RevolutionMai NabiehNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofWinnie WiyonoNo ratings yet
- 2 HCV Pangenotipe SOHO 2021 Dr. FardahDocument30 pages2 HCV Pangenotipe SOHO 2021 Dr. FardahAnnisa Oktoviani MursidaNo ratings yet
- 11168-Article Text-81547-2-10-20231227Document12 pages11168-Article Text-81547-2-10-20231227ppdsipd2019No ratings yet
- Resistance in HCV: Andrew J. Muir, MD MHSDocument33 pagesResistance in HCV: Andrew J. Muir, MD MHSEleni HagosNo ratings yet
- APJCP - Volume 23 - Issue 9 - Pages 2965-2971Document7 pagesAPJCP - Volume 23 - Issue 9 - Pages 2965-2971Ivania MarquezNo ratings yet
- Pretreatment To Avoid Positive RT-PCR Results With Inactivated VirusesDocument9 pagesPretreatment To Avoid Positive RT-PCR Results With Inactivated VirusesNori PurnamaNo ratings yet
- FTP PDFDocument5 pagesFTP PDFEltari SumbayakNo ratings yet
- Ganciclovir Dosing StrategiesDocument5 pagesGanciclovir Dosing StrategiesLUCY ROSALINOCYNo ratings yet
- Hepatitis C EditorialDocument3 pagesHepatitis C EditorialLuis Adolfo BermudezNo ratings yet
- Toksisitas Hati Terkait Dengan Sofosbuvir, Inhibitor NS5A: Laporan KasusDocument9 pagesToksisitas Hati Terkait Dengan Sofosbuvir, Inhibitor NS5A: Laporan KasusAldy WhisnuNo ratings yet
- Hep C en WercDocument7 pagesHep C en WerchidrogiriumNo ratings yet
- Effect of Rosuvastatin On Warfarin Pharmacodynamics and PharmacokineticsDocument9 pagesEffect of Rosuvastatin On Warfarin Pharmacodynamics and PharmacokineticsLuciana OliveiraNo ratings yet
- J Jacc 2023 04 019dDocument12 pagesJ Jacc 2023 04 019dCristi AlexandruNo ratings yet
- Disposition of Voriconazole During Continuous Veno-Venous Haemodiafiltration (CVVHDF) in A Single PatientDocument2 pagesDisposition of Voriconazole During Continuous Veno-Venous Haemodiafiltration (CVVHDF) in A Single PatientNguyễn LongNo ratings yet
- 11 COVID 19 Therapeutics For Nonhospitalized Patients Jan 2022Document2 pages11 COVID 19 Therapeutics For Nonhospitalized Patients Jan 2022rudy sanabriaNo ratings yet
- Remdesivir For 5 or 10 Days in Patients With Severe Covid-19Document11 pagesRemdesivir For 5 or 10 Days in Patients With Severe Covid-19TheRainMelodyNo ratings yet
- ContentServer - Asp 47Document8 pagesContentServer - Asp 47TataNo ratings yet
- 2 AnemiaDocument13 pages2 AnemiasalwaNo ratings yet
- REGEN-COV Antibody Combination and Outcomes in Outpatients With Covid-19Document12 pagesREGEN-COV Antibody Combination and Outcomes in Outpatients With Covid-19Trần Quang HuyNo ratings yet
- Hepatitis C Virus-Host Interactions and Therapeutics: Current Insights and Future PerspectivesFrom EverandHepatitis C Virus-Host Interactions and Therapeutics: Current Insights and Future PerspectivesNo ratings yet