
Blood
Blood
You might also like
- Examination Sheets For Internal MedicineDocument69 pagesExamination Sheets For Internal MedicineSaja SaqerNo ratings yet
- Path DumpsDocument44 pagesPath DumpsAndleeb ImranNo ratings yet
- Hypoglycemia Treatment ProtocolDocument1 pageHypoglycemia Treatment ProtocolCherryBeeNo ratings yet
- Chart of Commonly Transfused Blood ProductsDocument2 pagesChart of Commonly Transfused Blood Productsmara5140100% (8)
- Hem-Onc: AnswerDocument3 pagesHem-Onc: AnswerAman Raj KNo ratings yet
- Chapter 3 - WBC Abnormalities: 3.1 NeutrophiliaDocument25 pagesChapter 3 - WBC Abnormalities: 3.1 NeutrophiliaShishir AhmedNo ratings yet
- 13 Antihypertensive Drugs (Notes) AtfDocument24 pages13 Antihypertensive Drugs (Notes) AtfFeven AbrahamNo ratings yet
- Bleeding DisorderDocument90 pagesBleeding DisorderAnooda MazenNo ratings yet
- Platelet CasesDocument13 pagesPlatelet CasesRaheel IftikharNo ratings yet
- USMLE 1 Hematology BookDocument368 pagesUSMLE 1 Hematology BookPRINCENo ratings yet
- CARDIO - Valvular Heart Diseases Table DR BARTOLOMEDocument8 pagesCARDIO - Valvular Heart Diseases Table DR BARTOLOMEShams JailaniNo ratings yet
- TABLE of GENETIC DISORDERS PDFDocument13 pagesTABLE of GENETIC DISORDERS PDFQworld100% (1)
- High Yield OSCE - PediaDocument1 pageHigh Yield OSCE - Pediarere choiNo ratings yet
- USMLE Logistic Packet For IMGs-1Document7 pagesUSMLE Logistic Packet For IMGs-1Brian VianaNo ratings yet
- Normal Lab Values (USMLE Step 1)Document12 pagesNormal Lab Values (USMLE Step 1)nmp274No ratings yet
- Vasculitis: Disorder Vessels Pathology Presentation Test TX OtherDocument3 pagesVasculitis: Disorder Vessels Pathology Presentation Test TX OthermcwnotesNo ratings yet
- Haematology-Summary My NotesDocument24 pagesHaematology-Summary My NotesToria053No ratings yet
- MY Hematology MasterclassDocument32 pagesMY Hematology Masterclassabdul qayyumNo ratings yet
- Tumor Markers: Blood Group AntigenDocument5 pagesTumor Markers: Blood Group AntigenAngela ReyesNo ratings yet
- Heart SoundsDocument2 pagesHeart Soundsdanny_awwadNo ratings yet
- Hematology DR - Ahmed MowafyDocument111 pagesHematology DR - Ahmed MowafyMohamed AlsaabNo ratings yet
- Enzyme Deficiencies of Glycolysis and TCA: D N D S /SDocument8 pagesEnzyme Deficiencies of Glycolysis and TCA: D N D S /SJordan WhiteNo ratings yet
- Chemical Pathology Reference Range 2017Document19 pagesChemical Pathology Reference Range 2017Shobana RaveendranNo ratings yet
- Bipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomsDocument2 pagesBipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomshumdingerNo ratings yet
- Cardiovascular DiseasesDocument4 pagesCardiovascular DiseasesAshley Nicole LimNo ratings yet
- Internal Medicine Quick TablesDocument276 pagesInternal Medicine Quick Tablesjoey plouffeNo ratings yet
- Bootcamp's Step 1 Study ScheduleDocument8 pagesBootcamp's Step 1 Study ScheduleGlorivy E. Mora GonzalezNo ratings yet
- Mediastinum and Its ContentsDocument11 pagesMediastinum and Its ContentsPap YeeNo ratings yet
- PATH All TA Reviews Answers and Notes11Document718 pagesPATH All TA Reviews Answers and Notes11Andleeb Imran100% (1)
- Overview of AnaemiaDocument2 pagesOverview of AnaemiaGerardLumNo ratings yet
- Chart - WBC DisordersDocument1 pageChart - WBC DisordersSamuel RothschildNo ratings yet
- Review Slides OphthaDocument14 pagesReview Slides OphthaSUSHMITA MAE ROSE CONTRERASNo ratings yet
- Cardiovascular System PDFDocument182 pagesCardiovascular System PDFXochitl ZambranoNo ratings yet
- Infectious Disease (Part 1) : Viral DiseasesDocument11 pagesInfectious Disease (Part 1) : Viral Diseasesmiguel gaquitNo ratings yet
- OPTOMED-HW2-Diabetic Retinopathy PDFDocument3 pagesOPTOMED-HW2-Diabetic Retinopathy PDFDanalie SalvadorNo ratings yet
- MHD Exam 5 MaterialDocument122 pagesMHD Exam 5 Materialnaexuis5467100% (1)
- Adrenal Gland - Physiology, Pathology, and Pharmacology - Lecturio PDFDocument8 pagesAdrenal Gland - Physiology, Pathology, and Pharmacology - Lecturio PDFfaiz alamNo ratings yet
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocument3 pagesHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Ninja On Fleek - Fern Charts MT2 SLAY Most UpdatedDocument56 pagesNinja On Fleek - Fern Charts MT2 SLAY Most UpdatedyenniNo ratings yet
- MCQ 1. Heart Sound Heart Sound S1 S2Document7 pagesMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNo ratings yet
- (8!5!13) Cell Injury OutlineDocument9 pages(8!5!13) Cell Injury OutlineBhumiShahNo ratings yet
- Vasculitis MindnodeDocument1 pageVasculitis MindnodeToño VargasNo ratings yet
- VirologyLearnTable 2017-Sketchy PDFDocument4 pagesVirologyLearnTable 2017-Sketchy PDFdfgbdfgNo ratings yet
- Lec 2 - Blood VesselsDocument12 pagesLec 2 - Blood VesselsJeffrey LübbertNo ratings yet
- Microcytic AnemiaDocument2 pagesMicrocytic AnemiaLanaNo ratings yet
- Practical Aspects of Antibiotic Selection: Debbie Tristram, MD Professor of Pediatrics Albany Medical CollegeDocument52 pagesPractical Aspects of Antibiotic Selection: Debbie Tristram, MD Professor of Pediatrics Albany Medical Collegest_arjunaNo ratings yet
- GI Diarrheal Micro ChartDocument3 pagesGI Diarrheal Micro ChartEvan MillerNo ratings yet
- EndoDocument8 pagesEndoSheryl Layne Lao-SebrioNo ratings yet
- B - Embyrology HomologuesDocument1 pageB - Embyrology HomologuesS ParekhNo ratings yet
- Headache History: Introduction - WIPPPDocument4 pagesHeadache History: Introduction - WIPPPAmjad_2020No ratings yet
- Anatomy RR CerebellumDocument106 pagesAnatomy RR Cerebellumभईया भोसडिकाNo ratings yet
- Acute Myeloproliferative Acute Lymphoproliferative Chronic Myeloproliferative Chronic Lymphoproliferative Plasma Cell NeoplasmDocument1 pageAcute Myeloproliferative Acute Lymphoproliferative Chronic Myeloproliferative Chronic Lymphoproliferative Plasma Cell NeoplasmAudreySlitNo ratings yet
- Path Concept MapsDocument113 pagesPath Concept MapsAndleeb ImranNo ratings yet
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDocument25 pagesClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiNo ratings yet
- HEMATOLOGYDocument36 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINNo ratings yet
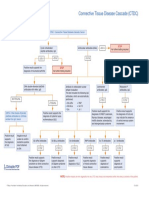
- Connective Tissue Disease CascadeDocument1 pageConnective Tissue Disease CascadeYustina BubnovaNo ratings yet
- Important GIT DrugsDocument3 pagesImportant GIT DrugsAndleeb ImranNo ratings yet
- Anemia SDocument42 pagesAnemia SCristinaGheorgheNo ratings yet
- UntitledDocument3 pagesUntitledSandeep m rNo ratings yet
- Aplastic and Hypoplastic Anemias Including Mylodysplastic SyndromeDocument47 pagesAplastic and Hypoplastic Anemias Including Mylodysplastic SyndromeRahul Kumar VermaNo ratings yet
- Ahuja, Motiani - 2004 - Current and Evolving Issues in Transfusion PracticeDocument8 pagesAhuja, Motiani - 2004 - Current and Evolving Issues in Transfusion Practicesushmakumari009No ratings yet
- Thrombocytopenia: Decreased Production Increased Destruction Sequestration PseudothrombocytopeniaDocument43 pagesThrombocytopenia: Decreased Production Increased Destruction Sequestration PseudothrombocytopeniaDea Tasha MeicitaNo ratings yet
- Therapeutic Plasma Exchange in Thrombotic Thrombocytopenic PurpuraDocument9 pagesTherapeutic Plasma Exchange in Thrombotic Thrombocytopenic Purpurasugi9namliNo ratings yet
- Pediatric HematologyDocument50 pagesPediatric HematologyYemaya84No ratings yet
- Koigi Benard Gathere H12/11303/15 Reproductive Health Assignment Coagulation Disorders in PregnancyDocument8 pagesKoigi Benard Gathere H12/11303/15 Reproductive Health Assignment Coagulation Disorders in PregnancyGATHERE KOIGINo ratings yet
- 4 Progress NotesDocument6 pages4 Progress NotesDinarkram Rabreca EculNo ratings yet
- Questions On Spleen and Splenectomy: Surgery Books For ResidentsDocument3 pagesQuestions On Spleen and Splenectomy: Surgery Books For ResidentsSajag GuptaNo ratings yet
- Preoperative HO RanyDocument35 pagesPreoperative HO RanyRMRNo ratings yet
- Signal Assessment Report Embolic Thrombotic Events SMQ Covid 19 Vaccine Chadox1 S Recombinant Covid - enDocument50 pagesSignal Assessment Report Embolic Thrombotic Events SMQ Covid 19 Vaccine Chadox1 S Recombinant Covid - enFlorinelNo ratings yet
- TrombositopeniaDocument12 pagesTrombositopeniaDias RahmawatiNo ratings yet
- Maternal Adaptations To Pregnancy - Hematologic Changes - UpToDate PDFDocument27 pagesMaternal Adaptations To Pregnancy - Hematologic Changes - UpToDate PDFDiego Andres VasquezNo ratings yet
- Bleeding Disorders 1Document152 pagesBleeding Disorders 1Shameena KnNo ratings yet
- Chapter 4 Drug StudyDocument9 pagesChapter 4 Drug StudyRegee Rose LacsonNo ratings yet
- ThrombocytopeniaDocument12 pagesThrombocytopeniatantyNo ratings yet
- Instruction: Select The Correct Answer For Each of The Following Questions. Mark Only One Answer byDocument7 pagesInstruction: Select The Correct Answer For Each of The Following Questions. Mark Only One Answer byEden Marie FranciscoNo ratings yet
- ThrombocytopeniaDocument19 pagesThrombocytopeniaChiyaanVikram100% (1)
- September 2018: Frcpath Questions Hemato-OncologyDocument24 pagesSeptember 2018: Frcpath Questions Hemato-OncologySyed Danish Ali100% (1)
- Kuliah Platelets DisordersDocument22 pagesKuliah Platelets DisordersDesi AdiyatiNo ratings yet
- Care of Clients With Physiologic and Psychosocial AlterationsDocument34 pagesCare of Clients With Physiologic and Psychosocial AlterationsChloie Marie RosalejosNo ratings yet
- Immune ThrombocytopeniaDocument11 pagesImmune ThrombocytopeniamiguelalmenarezNo ratings yet
- Circulating SerotoninDocument17 pagesCirculating Serotoninnihilx27374No ratings yet
- Drugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDocument4 pagesDrugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDejan OgnjanovicNo ratings yet
- Seminar 9-ITPDocument22 pagesSeminar 9-ITPanon_67984147No ratings yet
- HY USMLE Review Part IDocument18 pagesHY USMLE Review Part IDr.2020No ratings yet
- Terapi Rebozet Pada Pasien ITPDocument37 pagesTerapi Rebozet Pada Pasien ITPselusin internaNo ratings yet
- Evan Syndrome A Case ReportDocument3 pagesEvan Syndrome A Case ReportEditor IJTSRDNo ratings yet
- Hemostasis and Coagulation: Miklós MolnárDocument67 pagesHemostasis and Coagulation: Miklós MolnárHamzaNo ratings yet
- Schwartz 9th Ed: Chapter Outline: The SpleenDocument22 pagesSchwartz 9th Ed: Chapter Outline: The SpleenKathryn Reunilla100% (1)
- Inflammatory Disease of The HeartDocument20 pagesInflammatory Disease of The HeartmichaelurielNo ratings yet
- Clinpath-04.-Disorders of Hemostasis and Blood CoagulationDocument11 pagesClinpath-04.-Disorders of Hemostasis and Blood CoagulationCharisse Angelica MacedaNo ratings yet






















































































Download as docx, pdf, or txt
You might also like
- Examination Sheets For Internal MedicineDocument69 pagesExamination Sheets For Internal MedicineSaja SaqerNo ratings yet
- Path DumpsDocument44 pagesPath DumpsAndleeb ImranNo ratings yet
- Hypoglycemia Treatment ProtocolDocument1 pageHypoglycemia Treatment ProtocolCherryBeeNo ratings yet
- Chart of Commonly Transfused Blood ProductsDocument2 pagesChart of Commonly Transfused Blood Productsmara5140100% (8)
- Hem-Onc: AnswerDocument3 pagesHem-Onc: AnswerAman Raj KNo ratings yet
- Chapter 3 - WBC Abnormalities: 3.1 NeutrophiliaDocument25 pagesChapter 3 - WBC Abnormalities: 3.1 NeutrophiliaShishir AhmedNo ratings yet
- 13 Antihypertensive Drugs (Notes) AtfDocument24 pages13 Antihypertensive Drugs (Notes) AtfFeven AbrahamNo ratings yet
- Bleeding DisorderDocument90 pagesBleeding DisorderAnooda MazenNo ratings yet
- Platelet CasesDocument13 pagesPlatelet CasesRaheel IftikharNo ratings yet
- USMLE 1 Hematology BookDocument368 pagesUSMLE 1 Hematology BookPRINCENo ratings yet
- CARDIO - Valvular Heart Diseases Table DR BARTOLOMEDocument8 pagesCARDIO - Valvular Heart Diseases Table DR BARTOLOMEShams JailaniNo ratings yet
- TABLE of GENETIC DISORDERS PDFDocument13 pagesTABLE of GENETIC DISORDERS PDFQworld100% (1)
- High Yield OSCE - PediaDocument1 pageHigh Yield OSCE - Pediarere choiNo ratings yet
- USMLE Logistic Packet For IMGs-1Document7 pagesUSMLE Logistic Packet For IMGs-1Brian VianaNo ratings yet
- Normal Lab Values (USMLE Step 1)Document12 pagesNormal Lab Values (USMLE Step 1)nmp274No ratings yet
- Vasculitis: Disorder Vessels Pathology Presentation Test TX OtherDocument3 pagesVasculitis: Disorder Vessels Pathology Presentation Test TX OthermcwnotesNo ratings yet
- Haematology-Summary My NotesDocument24 pagesHaematology-Summary My NotesToria053No ratings yet
- MY Hematology MasterclassDocument32 pagesMY Hematology Masterclassabdul qayyumNo ratings yet
- Tumor Markers: Blood Group AntigenDocument5 pagesTumor Markers: Blood Group AntigenAngela ReyesNo ratings yet
- Heart SoundsDocument2 pagesHeart Soundsdanny_awwadNo ratings yet
- Hematology DR - Ahmed MowafyDocument111 pagesHematology DR - Ahmed MowafyMohamed AlsaabNo ratings yet
- Enzyme Deficiencies of Glycolysis and TCA: D N D S /SDocument8 pagesEnzyme Deficiencies of Glycolysis and TCA: D N D S /SJordan WhiteNo ratings yet
- Chemical Pathology Reference Range 2017Document19 pagesChemical Pathology Reference Range 2017Shobana RaveendranNo ratings yet
- Bipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomsDocument2 pagesBipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomshumdingerNo ratings yet
- Cardiovascular DiseasesDocument4 pagesCardiovascular DiseasesAshley Nicole LimNo ratings yet
- Internal Medicine Quick TablesDocument276 pagesInternal Medicine Quick Tablesjoey plouffeNo ratings yet
- Bootcamp's Step 1 Study ScheduleDocument8 pagesBootcamp's Step 1 Study ScheduleGlorivy E. Mora GonzalezNo ratings yet
- Mediastinum and Its ContentsDocument11 pagesMediastinum and Its ContentsPap YeeNo ratings yet
- PATH All TA Reviews Answers and Notes11Document718 pagesPATH All TA Reviews Answers and Notes11Andleeb Imran100% (1)
- Overview of AnaemiaDocument2 pagesOverview of AnaemiaGerardLumNo ratings yet
- Chart - WBC DisordersDocument1 pageChart - WBC DisordersSamuel RothschildNo ratings yet
- Review Slides OphthaDocument14 pagesReview Slides OphthaSUSHMITA MAE ROSE CONTRERASNo ratings yet
- Cardiovascular System PDFDocument182 pagesCardiovascular System PDFXochitl ZambranoNo ratings yet
- Infectious Disease (Part 1) : Viral DiseasesDocument11 pagesInfectious Disease (Part 1) : Viral Diseasesmiguel gaquitNo ratings yet
- OPTOMED-HW2-Diabetic Retinopathy PDFDocument3 pagesOPTOMED-HW2-Diabetic Retinopathy PDFDanalie SalvadorNo ratings yet
- MHD Exam 5 MaterialDocument122 pagesMHD Exam 5 Materialnaexuis5467100% (1)
- Adrenal Gland - Physiology, Pathology, and Pharmacology - Lecturio PDFDocument8 pagesAdrenal Gland - Physiology, Pathology, and Pharmacology - Lecturio PDFfaiz alamNo ratings yet
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocument3 pagesHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Ninja On Fleek - Fern Charts MT2 SLAY Most UpdatedDocument56 pagesNinja On Fleek - Fern Charts MT2 SLAY Most UpdatedyenniNo ratings yet
- MCQ 1. Heart Sound Heart Sound S1 S2Document7 pagesMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNo ratings yet
- (8!5!13) Cell Injury OutlineDocument9 pages(8!5!13) Cell Injury OutlineBhumiShahNo ratings yet
- Vasculitis MindnodeDocument1 pageVasculitis MindnodeToño VargasNo ratings yet
- VirologyLearnTable 2017-Sketchy PDFDocument4 pagesVirologyLearnTable 2017-Sketchy PDFdfgbdfgNo ratings yet
- Lec 2 - Blood VesselsDocument12 pagesLec 2 - Blood VesselsJeffrey LübbertNo ratings yet
- Microcytic AnemiaDocument2 pagesMicrocytic AnemiaLanaNo ratings yet
- Practical Aspects of Antibiotic Selection: Debbie Tristram, MD Professor of Pediatrics Albany Medical CollegeDocument52 pagesPractical Aspects of Antibiotic Selection: Debbie Tristram, MD Professor of Pediatrics Albany Medical Collegest_arjunaNo ratings yet
- GI Diarrheal Micro ChartDocument3 pagesGI Diarrheal Micro ChartEvan MillerNo ratings yet
- EndoDocument8 pagesEndoSheryl Layne Lao-SebrioNo ratings yet
- B - Embyrology HomologuesDocument1 pageB - Embyrology HomologuesS ParekhNo ratings yet
- Headache History: Introduction - WIPPPDocument4 pagesHeadache History: Introduction - WIPPPAmjad_2020No ratings yet
- Anatomy RR CerebellumDocument106 pagesAnatomy RR Cerebellumभईया भोसडिकाNo ratings yet
- Acute Myeloproliferative Acute Lymphoproliferative Chronic Myeloproliferative Chronic Lymphoproliferative Plasma Cell NeoplasmDocument1 pageAcute Myeloproliferative Acute Lymphoproliferative Chronic Myeloproliferative Chronic Lymphoproliferative Plasma Cell NeoplasmAudreySlitNo ratings yet
- Path Concept MapsDocument113 pagesPath Concept MapsAndleeb ImranNo ratings yet
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDocument25 pagesClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiNo ratings yet
- HEMATOLOGYDocument36 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINNo ratings yet
- Connective Tissue Disease CascadeDocument1 pageConnective Tissue Disease CascadeYustina BubnovaNo ratings yet
- Important GIT DrugsDocument3 pagesImportant GIT DrugsAndleeb ImranNo ratings yet
- Anemia SDocument42 pagesAnemia SCristinaGheorgheNo ratings yet
- UntitledDocument3 pagesUntitledSandeep m rNo ratings yet
- Aplastic and Hypoplastic Anemias Including Mylodysplastic SyndromeDocument47 pagesAplastic and Hypoplastic Anemias Including Mylodysplastic SyndromeRahul Kumar VermaNo ratings yet
- Ahuja, Motiani - 2004 - Current and Evolving Issues in Transfusion PracticeDocument8 pagesAhuja, Motiani - 2004 - Current and Evolving Issues in Transfusion Practicesushmakumari009No ratings yet
- Thrombocytopenia: Decreased Production Increased Destruction Sequestration PseudothrombocytopeniaDocument43 pagesThrombocytopenia: Decreased Production Increased Destruction Sequestration PseudothrombocytopeniaDea Tasha MeicitaNo ratings yet
- Therapeutic Plasma Exchange in Thrombotic Thrombocytopenic PurpuraDocument9 pagesTherapeutic Plasma Exchange in Thrombotic Thrombocytopenic Purpurasugi9namliNo ratings yet
- Pediatric HematologyDocument50 pagesPediatric HematologyYemaya84No ratings yet
- Koigi Benard Gathere H12/11303/15 Reproductive Health Assignment Coagulation Disorders in PregnancyDocument8 pagesKoigi Benard Gathere H12/11303/15 Reproductive Health Assignment Coagulation Disorders in PregnancyGATHERE KOIGINo ratings yet
- 4 Progress NotesDocument6 pages4 Progress NotesDinarkram Rabreca EculNo ratings yet
- Questions On Spleen and Splenectomy: Surgery Books For ResidentsDocument3 pagesQuestions On Spleen and Splenectomy: Surgery Books For ResidentsSajag GuptaNo ratings yet
- Preoperative HO RanyDocument35 pagesPreoperative HO RanyRMRNo ratings yet
- Signal Assessment Report Embolic Thrombotic Events SMQ Covid 19 Vaccine Chadox1 S Recombinant Covid - enDocument50 pagesSignal Assessment Report Embolic Thrombotic Events SMQ Covid 19 Vaccine Chadox1 S Recombinant Covid - enFlorinelNo ratings yet
- TrombositopeniaDocument12 pagesTrombositopeniaDias RahmawatiNo ratings yet
- Maternal Adaptations To Pregnancy - Hematologic Changes - UpToDate PDFDocument27 pagesMaternal Adaptations To Pregnancy - Hematologic Changes - UpToDate PDFDiego Andres VasquezNo ratings yet
- Bleeding Disorders 1Document152 pagesBleeding Disorders 1Shameena KnNo ratings yet
- Chapter 4 Drug StudyDocument9 pagesChapter 4 Drug StudyRegee Rose LacsonNo ratings yet
- ThrombocytopeniaDocument12 pagesThrombocytopeniatantyNo ratings yet
- Instruction: Select The Correct Answer For Each of The Following Questions. Mark Only One Answer byDocument7 pagesInstruction: Select The Correct Answer For Each of The Following Questions. Mark Only One Answer byEden Marie FranciscoNo ratings yet
- ThrombocytopeniaDocument19 pagesThrombocytopeniaChiyaanVikram100% (1)
- September 2018: Frcpath Questions Hemato-OncologyDocument24 pagesSeptember 2018: Frcpath Questions Hemato-OncologySyed Danish Ali100% (1)
- Kuliah Platelets DisordersDocument22 pagesKuliah Platelets DisordersDesi AdiyatiNo ratings yet
- Care of Clients With Physiologic and Psychosocial AlterationsDocument34 pagesCare of Clients With Physiologic and Psychosocial AlterationsChloie Marie RosalejosNo ratings yet
- Immune ThrombocytopeniaDocument11 pagesImmune ThrombocytopeniamiguelalmenarezNo ratings yet
- Circulating SerotoninDocument17 pagesCirculating Serotoninnihilx27374No ratings yet
- Drugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDocument4 pagesDrugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDejan OgnjanovicNo ratings yet
- Seminar 9-ITPDocument22 pagesSeminar 9-ITPanon_67984147No ratings yet
- HY USMLE Review Part IDocument18 pagesHY USMLE Review Part IDr.2020No ratings yet
- Terapi Rebozet Pada Pasien ITPDocument37 pagesTerapi Rebozet Pada Pasien ITPselusin internaNo ratings yet
- Evan Syndrome A Case ReportDocument3 pagesEvan Syndrome A Case ReportEditor IJTSRDNo ratings yet
- Hemostasis and Coagulation: Miklós MolnárDocument67 pagesHemostasis and Coagulation: Miklós MolnárHamzaNo ratings yet
- Schwartz 9th Ed: Chapter Outline: The SpleenDocument22 pagesSchwartz 9th Ed: Chapter Outline: The SpleenKathryn Reunilla100% (1)
- Inflammatory Disease of The HeartDocument20 pagesInflammatory Disease of The HeartmichaelurielNo ratings yet
- Clinpath-04.-Disorders of Hemostasis and Blood CoagulationDocument11 pagesClinpath-04.-Disorders of Hemostasis and Blood CoagulationCharisse Angelica MacedaNo ratings yet