Download as pdf or txt
You might also like
- Root Operations in The Medical and Surgical Section (ICD-10)Document2 pagesRoot Operations in The Medical and Surgical Section (ICD-10)Nicholas Henry100% (1)
- Drug ClearanceDocument65 pagesDrug ClearanceSyed Umair100% (1)
- ObturatorsDocument162 pagesObturatorsTaran67% (3)
- 8000 GK Questions UpdatedDocument260 pages8000 GK Questions UpdatedPrasanna100% (1)
- 1 - Renal Excretion of DrugsDocument18 pages1 - Renal Excretion of DrugsKashar SaeedNo ratings yet
- Excretion: Excretion. Elimination of Drugs and Its Metabolites FromDocument18 pagesExcretion: Excretion. Elimination of Drugs and Its Metabolites FromAlphahin 17100% (1)
- 4 General Pharmacology AliexcretionDocument31 pages4 General Pharmacology AliexcretionAurelia DS SequeiraNo ratings yet
- Renal Excretion of Drugs 3Document36 pagesRenal Excretion of Drugs 3Noorulhuda AbbasiNo ratings yet
- Excretion of DrugsDocument78 pagesExcretion of DrugsSohan PrasathNo ratings yet
- Lecture 1 Excrection of Drugs Pharm D 4th Year BPKDocument22 pagesLecture 1 Excrection of Drugs Pharm D 4th Year BPKDaisy Arora KhuranaNo ratings yet
- Drug ExcretionDocument20 pagesDrug ExcretionApurba Sarker Apu100% (3)
- Module 10 - Drugs Affecting The Urinary SystemDocument6 pagesModule 10 - Drugs Affecting The Urinary Systemsammcabico.studentNo ratings yet
- Renal and Non Renal Extretion of Drugs, Unit IIDocument12 pagesRenal and Non Renal Extretion of Drugs, Unit IIVarshaNo ratings yet
- Routes of Excretion Routes of Excretion Renal Excretion Non Renal Excretion Biliary ExcretionDocument5 pagesRoutes of Excretion Routes of Excretion Renal Excretion Non Renal Excretion Biliary Excretiontanuja reddyNo ratings yet
- Biopharmaceutics Lecture 7 UquDocument23 pagesBiopharmaceutics Lecture 7 Uquرنا الشريفNo ratings yet
- Unit-I Lecture-6Document3 pagesUnit-I Lecture-6Surjeet ChauhanNo ratings yet
- Excretion of Drugs: Dr. G.SAILAJA, M.Pharm - PH.D., Assoc. Professor, Dept. of PharmaceuticsDocument43 pagesExcretion of Drugs: Dr. G.SAILAJA, M.Pharm - PH.D., Assoc. Professor, Dept. of PharmaceuticsSailaja Reddy GunnamNo ratings yet
- 8 Drug ExcretionDocument61 pages8 Drug ExcretionAhmed YTNo ratings yet
- 2687pharmacy Lecture 2Document61 pages2687pharmacy Lecture 2Eman QawasmiNo ratings yet
- Drug Excretion-August 2020Document67 pagesDrug Excretion-August 2020Mussa Mwaitolage100% (1)
- EliminationDocument35 pagesEliminationPrathamesh PatilNo ratings yet
- 9 EliminationDocument5 pages9 EliminationkalloliNo ratings yet
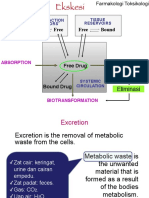
- Materi Fartok EkskresiDocument34 pagesMateri Fartok EkskresiOskarHowayNo ratings yet
- Human Physiology Urinary SystemDocument51 pagesHuman Physiology Urinary Systemmohamedsaithaf2000No ratings yet
- Excretion of DrugDocument36 pagesExcretion of DrugYeni SuwitaNo ratings yet
- Unit 2Document36 pagesUnit 2hasan.aliNo ratings yet
- ExcretionDocument35 pagesExcretionHely PatelNo ratings yet
- Renal PhysiologyDocument7 pagesRenal PhysiologySalah Mohamed FakhriNo ratings yet
- Chapter 18 Anaphy TransesDocument5 pagesChapter 18 Anaphy TransesHoly HaeinNo ratings yet
- CC2 PREMILS To FINALS MERGED PDFDocument65 pagesCC2 PREMILS To FINALS MERGED PDFAlecx LipatanNo ratings yet
- Revision FileDocument14 pagesRevision FileBasema HashhashNo ratings yet
- 3 Pharmacokinetics 2Document15 pages3 Pharmacokinetics 2aimi BatrisyiaNo ratings yet
- A. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)Document19 pagesA. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)IceNo ratings yet
- Chapter 1 Drug EliminationDocument116 pagesChapter 1 Drug Elimination221123No ratings yet
- K.23 Farmakologi (2) Pada Gagal GinjalDocument52 pagesK.23 Farmakologi (2) Pada Gagal GinjalHernita FerliyaniNo ratings yet
- Metabolic Pathway & Renal ExcretionDocument29 pagesMetabolic Pathway & Renal ExcretionRadha krishnaNo ratings yet
- Renal Pharma 3Document14 pagesRenal Pharma 3Pranjali WeladiNo ratings yet
- Pharma Nca1 Notes MidtermDocument8 pagesPharma Nca1 Notes MidtermAICEL A. ABILNo ratings yet
- GENERAL PHARMACOLOGY (Excretion)Document34 pagesGENERAL PHARMACOLOGY (Excretion)rexef82757No ratings yet
- CHAPTER 18 ANAPHY TransesDocument5 pagesCHAPTER 18 ANAPHY TransesHoly HaeinNo ratings yet
- Renal Drug ExcretionDocument15 pagesRenal Drug ExcretionSatwika EkanandaNo ratings yet
- Excretion of DrugsDocument43 pagesExcretion of DrugsBandameedi RamuNo ratings yet
- 1 General Introduction in Pharmacokinetics-Botswana 2019Document60 pages1 General Introduction in Pharmacokinetics-Botswana 2019Nelson MoreriNo ratings yet
- KidneyDocument6 pagesKidneyMohammad Jamal OwesatNo ratings yet
- 16.drug Excretion 1Document50 pages16.drug Excretion 1Ngetwa TzDe TheWirymanNo ratings yet
- 1 General PharmacologyDocument29 pages1 General PharmacologyAli EllaffiNo ratings yet
- PHPY 304 Study MidtermDocument31 pagesPHPY 304 Study Midtermbimal06khanalNo ratings yet
- Drug ExcretionDocument16 pagesDrug ExcretionSwapnilNo ratings yet
- Renal AllDocument38 pagesRenal AllAhmed MoneerNo ratings yet
- PHARMACOKINETICS & PharmacokineticsDocument60 pagesPHARMACOKINETICS & PharmacokineticsRaj PathakNo ratings yet
- Chapter 9 Excretory System PDFDocument17 pagesChapter 9 Excretory System PDFErica Ann Ical100% (1)
- 10.2.5 - Anti-Diarrhoea Agents Jan2014Document30 pages10.2.5 - Anti-Diarrhoea Agents Jan2014Gabrielle NnomoNo ratings yet
- Renal FunctionDocument11 pagesRenal FunctionJanely EstreraNo ratings yet
- Trans CC2 Lec Mod 1Document6 pagesTrans CC2 Lec Mod 1janekieannearlosNo ratings yet
- Chapter 26: Introduction To The Urinary SystemDocument37 pagesChapter 26: Introduction To The Urinary Systemmaatela7sasNo ratings yet
- 5 19 Excretory System PDFDocument12 pages5 19 Excretory System PDFHNo ratings yet
- Elimination: G. SrikarDocument23 pagesElimination: G. SrikarSowjanya NekuriNo ratings yet
- Excretion (Dr. Imran Ashraf)Document44 pagesExcretion (Dr. Imran Ashraf)Abdul WahabNo ratings yet
- To Convert BUN MG/DL To Urea In, BUN Multiplied With 2.14 - To Convert BUN MG/DL To Urea In, BUN Multiplied With 0.36Document6 pagesTo Convert BUN MG/DL To Urea In, BUN Multiplied With 2.14 - To Convert BUN MG/DL To Urea In, BUN Multiplied With 0.36RALPH JAN T. RIONo ratings yet
- PharmacokineticsDocument47 pagesPharmacokineticsْNo ratings yet
- ELIMINATIONDocument22 pagesELIMINATIONprashil charkariNo ratings yet
- Urinary System-2022-2023Document24 pagesUrinary System-2022-2023Fady FadyNo ratings yet
- CourseSpecification Form RehabDeptDocument3 pagesCourseSpecification Form RehabDeptAman GulNo ratings yet
- Instructor Course Assessment ReportDocument2 pagesInstructor Course Assessment ReportAman GulNo ratings yet
- Self Declaration FormDocument2 pagesSelf Declaration FormAman GulNo ratings yet
- Cho Nature ST Function ND AbsorptionDocument11 pagesCho Nature ST Function ND AbsorptionAman GulNo ratings yet
- Covent Garden Beauty Salon BrochureDocument2 pagesCovent Garden Beauty Salon Brochurethelondonseocompany_No ratings yet
- Powerpoint Protein LocalizationDocument54 pagesPowerpoint Protein LocalizationJoseph BenaiahNo ratings yet
- 01 - Decision Making in Emergency MedicineDocument4 pages01 - Decision Making in Emergency MedicineSlvdrPlgrnNo ratings yet
- Brace Your Core-WPS OfficeDocument3 pagesBrace Your Core-WPS Officecharles manuelNo ratings yet
- Muscular System March 2023 11Document95 pagesMuscular System March 2023 11ivy896613No ratings yet
- Surviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedDocument32 pagesSurviving Sepsis Campaign 2016 Guidelines Presentation Final RevisiedAdli Wafi Jabbar100% (1)
- Cardiopulmonary Bypass: DR R Sri Devi Assistant ProfessorDocument36 pagesCardiopulmonary Bypass: DR R Sri Devi Assistant ProfessorSanthi Swetha PudhotaNo ratings yet
- Lymphatic SystemDocument22 pagesLymphatic SystemdrynwhylNo ratings yet
- Best Practice Recommendations For Management of Swan Neck Deformity in Rheumatoid ArthritisDocument10 pagesBest Practice Recommendations For Management of Swan Neck Deformity in Rheumatoid ArthritisAirin QueNo ratings yet
- Cartuchos I-Stat 1Document2 pagesCartuchos I-Stat 1José CamposNo ratings yet
- DiverticulitisDocument2 pagesDiverticulitisyapyapvinx50% (2)
- Erasing Fear Memories Without Drugs: Jim SchnabelDocument2 pagesErasing Fear Memories Without Drugs: Jim SchnabelAlienistaPiNo ratings yet
- Digestive System ReviewDocument47 pagesDigestive System ReviewMartina RizkiNo ratings yet
- DrugDocument6 pagesDrugRose Ann MirafloresNo ratings yet
- Shaktanand: Shiv Swarodaya: Some Interesting AspectsDocument12 pagesShaktanand: Shiv Swarodaya: Some Interesting AspectsorekishNo ratings yet
- Chemotherapy and Renal Andhepatic Insufficiency 2008Document24 pagesChemotherapy and Renal Andhepatic Insufficiency 2008Vika RatuNo ratings yet
- Correlation Between The PH of Saliva, Plaque and Buffering Capacity of SalivaDocument3 pagesCorrelation Between The PH of Saliva, Plaque and Buffering Capacity of SalivasuhanaNo ratings yet
- Factors Affecting Body TemperatureDocument3 pagesFactors Affecting Body TemperaturenvhnygNo ratings yet
- Cell Structure Gizmo AnswersDocument5 pagesCell Structure Gizmo Answerspaula-navas 13451No ratings yet
- EnzymesDocument13 pagesEnzymesapi-290318217No ratings yet
- Pulseless Pumps & Artificial HeartsDocument23 pagesPulseless Pumps & Artificial HeartscafemedNo ratings yet
- CarbohydratesDocument17 pagesCarbohydratessafemindNo ratings yet
- S V ExercisesDocument2 pagesS V ExercisesAljake Llanes SalesNo ratings yet
- Elsa Manual SabreDocument50 pagesElsa Manual SabrerijalharunNo ratings yet
- Positioning Techniques in Long-Term Care: Self-Directed Learning Package For Health Care ProvidersDocument41 pagesPositioning Techniques in Long-Term Care: Self-Directed Learning Package For Health Care ProvidersHbk RajneeshNo ratings yet
- David Berceli Webinar Notes, Trauma Releasing Exercises NotesDocument23 pagesDavid Berceli Webinar Notes, Trauma Releasing Exercises NotesAnonymous F4KmWCH100% (11)
- Developing The WHOLE PersonDocument9 pagesDeveloping The WHOLE Persondianne genelzaNo ratings yet