Download as docx, pdf, or txt
You might also like
- Instant Download Connect Core Concepts in Health Brief 16th Edition Ebook PDF PDF ScribdDocument41 pagesInstant Download Connect Core Concepts in Health Brief 16th Edition Ebook PDF PDF Scribdcarmine.adams474100% (47)
- Phenylketonuria (PKU) : PH Arn, Nemours Children's Clinic, Jacksonville, FL, USADocument3 pagesPhenylketonuria (PKU) : PH Arn, Nemours Children's Clinic, Jacksonville, FL, USAHappy612No ratings yet
- FWD Producst: Products For AllDocument44 pagesFWD Producst: Products For AllCharish DanaoNo ratings yet
- Subclinical Hypothyroidism TDocument6 pagesSubclinical Hypothyroidism TAnisa Iswari Pombaile-NgurawanNo ratings yet
- Approach To Differential Diagnosis PDFDocument62 pagesApproach To Differential Diagnosis PDFanasNo ratings yet
- PkuDocument6 pagesPkuAlbertEscanoNo ratings yet
- PhenylketonuriaDocument8 pagesPhenylketonuriaAmberlee PetiNo ratings yet
- Phenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeDocument24 pagesPhenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeAsfoor gake1No ratings yet
- Inborn Errors of MetabolismDocument60 pagesInborn Errors of MetabolismPyneandy KimberlyNo ratings yet
- PhenylketonuriaDocument17 pagesPhenylketonuriamovies villa hit hai broNo ratings yet
- Biochemistry - METABOLISM OF PROTEINDocument44 pagesBiochemistry - METABOLISM OF PROTEINrebeccaNo ratings yet
- PHENYLKETONURIADocument22 pagesPHENYLKETONURIAIvy Ann AguirreNo ratings yet
- Inborn Errors of MetabolismDocument40 pagesInborn Errors of MetabolismajjaNo ratings yet
- Endocrine DisordersDocument33 pagesEndocrine DisordersTinaNo ratings yet
- Inborn Errors of Metabolism Student LectureDocument81 pagesInborn Errors of Metabolism Student LectureFavourNo ratings yet
- Endocrine DisordersDocument33 pagesEndocrine DisordersBuvana VigneshNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaAnny AlvrzNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaReham QueNo ratings yet
- Clinical FirstDocument342 pagesClinical FirstYasmeen AtiehNo ratings yet
- Aminoacid MetabolismDocument25 pagesAminoacid MetabolismMischief ManagerNo ratings yet
- 23 Pku AkuDocument1 page23 Pku AkuJose DolletonNo ratings yet
- Fenilketonuria: Devi WuysangDocument23 pagesFenilketonuria: Devi WuysangChristantina Pradescha AssaNo ratings yet
- Phenylketonur IA: Done byDocument27 pagesPhenylketonur IA: Done byAsfoor gake1100% (1)
- DR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHDocument2 pagesDR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHPonnusamy KumarNo ratings yet
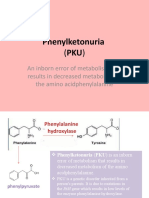
- Phenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino AcidphenylalanineDocument8 pagesPhenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino Acidphenylalanineელენე ბუჩუკურიNo ratings yet
- Munyame 2018Document6 pagesMunyame 2018kemoNo ratings yet
- PHENYLKETONURIADocument3 pagesPHENYLKETONURIAMiwa IshiiNo ratings yet
- DR Kumar Ponnusamy Biochemistry-Genetics USMLE Preparatory Course BIOGEN Reusable On-Line Resources For Large Group Teaching-Learning in Relatively Short TimeDocument1 pageDR Kumar Ponnusamy Biochemistry-Genetics USMLE Preparatory Course BIOGEN Reusable On-Line Resources For Large Group Teaching-Learning in Relatively Short TimeDr Kumar Ponnusamy100% (1)
- Articulo Final Verdadero!!!!Document6 pagesArticulo Final Verdadero!!!!lapzsssNo ratings yet
- Inborn Errors of Amino Acid Metabolism: (Advanced Nutrition)Document8 pagesInborn Errors of Amino Acid Metabolism: (Advanced Nutrition)Deepshikha PatelNo ratings yet
- Inborn Error of MetabolismDocument38 pagesInborn Error of MetabolismRubinaNo ratings yet
- Inherited Metabolic DisorderDocument12 pagesInherited Metabolic DisorderTrisha Dianne RaquenioNo ratings yet
- PhenylketonuriaDocument1 pagePhenylketonuriaHolly SevillanoNo ratings yet
- Phenyl Keto NuriaDocument3 pagesPhenyl Keto NuriawawawawaNo ratings yet
- MCH Group 8Document12 pagesMCH Group 8nafisatmuhammed452No ratings yet
- Phenylketonuria (PKU) : Diagnosis and ManagementDocument2 pagesPhenylketonuria (PKU) : Diagnosis and ManagementFerdianaNo ratings yet
- PhenylketonuriaDocument14 pagesPhenylketonuriaMonica MoralesNo ratings yet
- Inborn Error of Metabolism and Introduction To Cancer GeneticsDocument9 pagesInborn Error of Metabolism and Introduction To Cancer GeneticsviancaNo ratings yet
- Case3 PhenylketunuriaDocument2 pagesCase3 PhenylketunuriaKath BoniolNo ratings yet
- Urinalysis 2Document9 pagesUrinalysis 2Dawn GonzagaNo ratings yet
- Phenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)Document1 pagePhenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)reriti2008No ratings yet
- Phenylketonuria: Symposium: Inborn Errors of MetabolismDocument5 pagesPhenylketonuria: Symposium: Inborn Errors of MetabolismIntan RizanaNo ratings yet
- Unit 6 TransDocument8 pagesUnit 6 TransGrace FernandoNo ratings yet
- Pediatrics ReviewDocument275 pagesPediatrics ReviewHaslinNo ratings yet
- Amino Acid DisordersDocument7 pagesAmino Acid DisordersarshehadaNo ratings yet
- Group 4 - Pku (BSN 1-A)Document11 pagesGroup 4 - Pku (BSN 1-A)oluanah13No ratings yet
- Common IEM Solaf M Elsayed 2021Document13 pagesCommon IEM Solaf M Elsayed 2021anas barakahNo ratings yet
- Bio Chem Case ThreeDocument2 pagesBio Chem Case ThreeLeonard Rey Suratos ManabatNo ratings yet
- Inborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaDocument19 pagesInborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaSubhi MishraNo ratings yet
- Recurrent Kidney Stones in A Child With Lesch-Nyhan Syndrome: AnswersDocument3 pagesRecurrent Kidney Stones in A Child With Lesch-Nyhan Syndrome: AnswersAriani SetianingsihNo ratings yet
- Metabolic Disorders 01Document41 pagesMetabolic Disorders 01Brent LagartoNo ratings yet
- PHENYLKETONURIADocument4 pagesPHENYLKETONURIAmarsiel03No ratings yet
- AUBF Metabolic Disorders and Inborn Error of MetabolismDocument3 pagesAUBF Metabolic Disorders and Inborn Error of MetabolismAngela LaglivaNo ratings yet
- USMD, CSF, SEMEN - Professor'sDocument10 pagesUSMD, CSF, SEMEN - Professor'sMartin ClydeNo ratings yet
- PhenylketonuriaDocument10 pagesPhenylketonuriaMalathy Ravendran100% (1)
- Inborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Document4 pagesInborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Wen Jie LauNo ratings yet
- Aub F Urine Screening For Metabolic DisordersDocument4 pagesAub F Urine Screening For Metabolic DisordersRomie SolacitoNo ratings yet
- Vii. Urine Screening For Metabolic DisordersDocument4 pagesVii. Urine Screening For Metabolic DisordersDee GeeNo ratings yet
- Biochemistry & Genetics Important Concepts Q&as DR Kumar Ponnusamy & Jegathambigai RN, Biochemistry & Genetics, International Medical University (IMU) / AIMST University School of Medicine, MalaysiaDocument60 pagesBiochemistry & Genetics Important Concepts Q&as DR Kumar Ponnusamy & Jegathambigai RN, Biochemistry & Genetics, International Medical University (IMU) / AIMST University School of Medicine, MalaysiaDr Kumar Ponnusamy100% (3)
- Phenyl Keto NuriaDocument1 pagePhenyl Keto NuriamucwcburdwanNo ratings yet
- Metabolic DisordersDocument80 pagesMetabolic DisordersXeniyaFedoryakNo ratings yet
- Hypophosphatemia, (Low Phosphate) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypophosphatemia, (Low Phosphate) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Blondin-Brosseau Et Al 2021Document28 pagesBlondin-Brosseau Et Al 2021JefersonMatosdeColaresNo ratings yet
- Physiotherapy Management: Otago Home Exercise ProgrammeDocument9 pagesPhysiotherapy Management: Otago Home Exercise ProgrammeanjelikaNo ratings yet
- Name of The Drug Mechanism of Action Dosage Indications Contraindications Adverse Reaction Nursing InterventionDocument4 pagesName of The Drug Mechanism of Action Dosage Indications Contraindications Adverse Reaction Nursing InterventionMary joy PaaNo ratings yet
- Disorders of The Endocrine SystemDocument12 pagesDisorders of The Endocrine SystemAlfred Jayson RuizNo ratings yet
- Paediatrics Workbook - Nuc304: SUMMER 2021Document10 pagesPaediatrics Workbook - Nuc304: SUMMER 2021Rawan KhateebNo ratings yet
- DecombDocument3 pagesDecombDr.2020No ratings yet
- Research Paper 4Document15 pagesResearch Paper 4api-548795523No ratings yet
- Acutescrotalemergencies: Molly M. Bourke,, Joshua Z. SilverbergDocument18 pagesAcutescrotalemergencies: Molly M. Bourke,, Joshua Z. SilverbergSebastian ChavesNo ratings yet
- Research Proposal FinalDocument35 pagesResearch Proposal FinalBienne Zyrus Earl CarpioNo ratings yet
- Principles of Inheritance and Variation - Revision WorksheetDocument5 pagesPrinciples of Inheritance and Variation - Revision Worksheetafsheenfatima2006No ratings yet
- Hyper Hyponatremia LERMADocument8 pagesHyper Hyponatremia LERMAJINYVEV APARICINo ratings yet
- Final SK Golden 7+8 ErrataDocument19 pagesFinal SK Golden 7+8 ErrataHassam ZulfiqarNo ratings yet
- Troponin Elevation in Coronary Vs Non Coronary DiseaseDocument10 pagesTroponin Elevation in Coronary Vs Non Coronary Diseasealejandro montesNo ratings yet
- HYPERMETROPIA and Myopia PDFDocument55 pagesHYPERMETROPIA and Myopia PDFDrashti ChudasamaNo ratings yet
- Week 13 CD COURSE TASK 7. Dengue Fever, Filariasis, Malaria and EncephalitisDocument5 pagesWeek 13 CD COURSE TASK 7. Dengue Fever, Filariasis, Malaria and EncephalitisRogelyn PatriarcaNo ratings yet
- History of Disease & Levels of Prevention 2Document39 pagesHistory of Disease & Levels of Prevention 2Nadine VillaretNo ratings yet
- Blueprints PsychiatryDocument432 pagesBlueprints PsychiatryFiona Fleming87% (15)
- Focal Segmental Glomerulosclerosis: State-of-the-Art and Clinical PerspectiveDocument15 pagesFocal Segmental Glomerulosclerosis: State-of-the-Art and Clinical PerspectiveGabriela CruzNo ratings yet
- AAMA - Anatomy and Physiology QuestionsDocument11 pagesAAMA - Anatomy and Physiology QuestionsHUAWEI HUAWEINo ratings yet
- Forensic PsychiatryDocument52 pagesForensic PsychiatrySiow Siow0% (1)
- Measuring The Occurrence of Disease: Dr. Elijah Kakande MBCHB, MPH Department of Public HealthDocument25 pagesMeasuring The Occurrence of Disease: Dr. Elijah Kakande MBCHB, MPH Department of Public HealthNawita JordanNo ratings yet
- Lumbar RadiculopathyDocument16 pagesLumbar Radiculopathyprince singhNo ratings yet
- GI BleedingDocument17 pagesGI BleedingBảo LongNo ratings yet
- Practical Paper 2Document32 pagesPractical Paper 2Ashika AshuNo ratings yet
- Trigemina Nerve Sem 2 WordDocument18 pagesTrigemina Nerve Sem 2 WordBharathi GudapatiNo ratings yet
- Dipiro PneumoniaDocument8 pagesDipiro Pneumoniameri dayaniNo ratings yet