Download as pdf or txt
You might also like
- IMFPADocument12 pagesIMFPAakadzituNo ratings yet
- UWIOC - Scholarship - Application - GeneralDocument6 pagesUWIOC - Scholarship - Application - GeneralAaliyah CharlesNo ratings yet
- Committee On Student Scholarship / Study GrantDocument3 pagesCommittee On Student Scholarship / Study GrantsattNo ratings yet
- MA Bursary Application FormDocument7 pagesMA Bursary Application FormhalalisaninhlosenhleNo ratings yet
- Ojt FormDocument18 pagesOjt FormKyle TyNo ratings yet
- Youth Ambassadors - Inbound Student Application - 2020 PDFDocument15 pagesYouth Ambassadors - Inbound Student Application - 2020 PDFDalilah CarpenterNo ratings yet
- FAMS Financial Aid FormDocument5 pagesFAMS Financial Aid FormHammad EjazNo ratings yet
- PSRC APPLICATION FORM With DPA Consent 2021 - Copy (Replica) (Replica)Document2 pagesPSRC APPLICATION FORM With DPA Consent 2021 - Copy (Replica) (Replica)Edcel SilvaNo ratings yet
- 2011 2012 Financial Aid ApplicationDocument4 pages2011 2012 Financial Aid ApplicationSescily FeistyNo ratings yet
- QR 2.1-1-3-c Job Application FormDocument3 pagesQR 2.1-1-3-c Job Application FormMochammad Aji HutamaNo ratings yet
- SUSI-2020 Application FormDocument5 pagesSUSI-2020 Application Formwafaa elottriNo ratings yet
- Dube Trade Port Application FormDocument7 pagesDube Trade Port Application FormNcediswaNo ratings yet
- 2023 Work and Travel ApplicationDocument6 pages2023 Work and Travel ApplicationMarly VeraNo ratings yet
- Job Application FormDocument6 pagesJob Application Formpermaikenyalang3024No ratings yet
- Application Form English 入學申請表 英文版 -1Document8 pagesApplication Form English 入學申請表 英文版 -1bagus ibnu utamaNo ratings yet
- Dav Centenary Public School: (Part - A)Document5 pagesDav Centenary Public School: (Part - A)Nitin SharmaNo ratings yet
- Sample HR FormDocument4 pagesSample HR FormJesstoni CaniedoNo ratings yet
- Application Form ASTON BintaroDocument3 pagesApplication Form ASTON BintaroROOMS ARTOTEL CASA CIKARANGNo ratings yet
- FAMS Application For Financial Aid For Education: Subject To Availability of FundsDocument4 pagesFAMS Application For Financial Aid For Education: Subject To Availability of FundsMohammad ShafiqNo ratings yet
- Ihsan Trsut Qarz Hasna Application FormDocument14 pagesIhsan Trsut Qarz Hasna Application FormJehanzaib javedNo ratings yet
- Candidate Application Form V2 23 June 2015 Neo EltariDocument4 pagesCandidate Application Form V2 23 June 2015 Neo Eltarianita nahakNo ratings yet
- 2018 SUSI Appllication Form EngDocument8 pages2018 SUSI Appllication Form Engmeziane brahimNo ratings yet
- FLP Esmel Fellowship Program 2022 2023 Application FormDocument2 pagesFLP Esmel Fellowship Program 2022 2023 Application FormHexeneNo ratings yet
- Mentor App - ReviewedDocument3 pagesMentor App - Reviewedapi-351705157No ratings yet
- 2023 UCF Legislative Scholars Internship Application HandshakeDocument4 pages2023 UCF Legislative Scholars Internship Application HandshakeZaki NaNo ratings yet
- Application FormDocument4 pagesApplication Formscribd22322No ratings yet
- HRD Form 001 Employee Application Gen - Admin v.001Document3 pagesHRD Form 001 Employee Application Gen - Admin v.001DadangNo ratings yet
- Invigilator Application Form 0 2Document2 pagesInvigilator Application Form 0 2Shail MakhijaniNo ratings yet
- ASEAN Leadership Training in JapanDocument5 pagesASEAN Leadership Training in JapanNaif OmarNo ratings yet
- Application Form V3 Jan 2022Document4 pagesApplication Form V3 Jan 2022IT Gunungmas GroupNo ratings yet
- Asmph Financial Aid Application - Non Ofw Income - Sy2013-14 PDFDocument19 pagesAsmph Financial Aid Application - Non Ofw Income - Sy2013-14 PDFCardioTCSNo ratings yet
- Selg Election Forms Grades 4 5Document4 pagesSelg Election Forms Grades 4 5vjornadalNo ratings yet
- Ahf Personal Grants 1Document7 pagesAhf Personal Grants 1Mary Joyce AquinoNo ratings yet
- UNL Financial ResourceDocument2 pagesUNL Financial ResourceKofi AmoakoNo ratings yet
- Application Form: Legal Scholarship Program ACADEMIC YEAR 2020-2021Document2 pagesApplication Form: Legal Scholarship Program ACADEMIC YEAR 2020-2021Michelle RamaNo ratings yet
- Icog Membership FormDocument2 pagesIcog Membership FormDrDevdatt Laxman PitaleNo ratings yet
- Applicant No. - : (Name in Birth Certificate) Last NameDocument5 pagesApplicant No. - : (Name in Birth Certificate) Last NameElisabeth HenangerNo ratings yet
- BG Check FormDocument1 pageBG Check Formmasterbats040217No ratings yet
- Application For EmploymentDocument4 pagesApplication For EmploymentDileep GoyalNo ratings yet
- Application For Housing Loan Under Griha ShobhaDocument7 pagesApplication For Housing Loan Under Griha ShobhaDr BusinessNo ratings yet
- Kas Secondary Bursary FormDocument4 pagesKas Secondary Bursary FormSam RuhiNo ratings yet
- SCG Sharing The Dream Scholarship Program - College LevelDocument5 pagesSCG Sharing The Dream Scholarship Program - College LevelJ DNo ratings yet
- Indian Association of Structural Engineers: Application Form - Fellow/Member/Associate MemberDocument3 pagesIndian Association of Structural Engineers: Application Form - Fellow/Member/Associate MemberS Muneer HussainNo ratings yet
- Al-Hind - Ap - Registration - FormDocument1 pageAl-Hind - Ap - Registration - FormJoy MunshiNo ratings yet
- Ihsan TrsutDocument14 pagesIhsan TrsutAakash Kumar MissraniNo ratings yet
- AFPMBAI Grade ApplicationDocument2 pagesAFPMBAI Grade ApplicationLem OrNo ratings yet
- PDS - 2022-2023 PDFDocument2 pagesPDS - 2022-2023 PDFMarcelino CalataNo ratings yet
- DDA Application FormatDocument2 pagesDDA Application FormatPooja TharejaNo ratings yet
- Government College University Hyderabad (Gcuh) : Application FormDocument2 pagesGovernment College University Hyderabad (Gcuh) : Application FormNauman IrfanNo ratings yet
- FLP Sy2019 2020 Scholarship Program Form and Guidelines 1Document6 pagesFLP Sy2019 2020 Scholarship Program Form and Guidelines 1Josef GutierrezNo ratings yet
- Application Form Youth For Development and Global XchangeDocument4 pagesApplication Form Youth For Development and Global Xchangeapi-26153714No ratings yet
- Parent/Guardian Information: Continued On ReverseDocument2 pagesParent/Guardian Information: Continued On Reverseadhi eng lrtNo ratings yet
- Pappas EmpApplication EnglishDocument2 pagesPappas EmpApplication EnglishGordon FreemanNo ratings yet
- Migration and Declaration FormsDocument5 pagesMigration and Declaration Formsdeepheat_008No ratings yet
- Please Complete All Sections in Block Letters in Your Own HandwritingDocument4 pagesPlease Complete All Sections in Block Letters in Your Own HandwritingSaarthak SangamnerkarNo ratings yet
- Application For Admission: Please Note: This Entire Form Is To Be Completed by The Applicant. Please Print ClearlyDocument3 pagesApplication For Admission: Please Note: This Entire Form Is To Be Completed by The Applicant. Please Print ClearlyJanuhu ZakaryNo ratings yet
- Indian Association of Structural Engineers: Application Form - Fellow/Member/Associate MemberDocument3 pagesIndian Association of Structural Engineers: Application Form - Fellow/Member/Associate Memberkhajarasool786No ratings yet
- App Form Apna Office IndividualDocument6 pagesApp Form Apna Office IndividualKadhar AnwarNo ratings yet
- Application For Admission - Middle and High School: ApplicantDocument2 pagesApplication For Admission - Middle and High School: ApplicantRafaelNo ratings yet
- FT SDW 096 00 Individual Inventory FormDocument2 pagesFT SDW 096 00 Individual Inventory FormNasi RiceNo ratings yet
- Information Processing in MeteorologyDocument8 pagesInformation Processing in MeteorologyDavid ThompsonNo ratings yet
- Nathan pdf3Document1 pageNathan pdf3David ThompsonNo ratings yet
- Britney Gordon's Resume PDFDocument3 pagesBritney Gordon's Resume PDFDavid ThompsonNo ratings yet
- NathanDocument1 pageNathanDavid ThompsonNo ratings yet
- Chadane Edwards - Graded Group AssignmentDocument8 pagesChadane Edwards - Graded Group AssignmentDavid ThompsonNo ratings yet
- Development of Shapes 2Document1 pageDevelopment of Shapes 2David ThompsonNo ratings yet
- Development of Shapes 1Document1 pageDevelopment of Shapes 1David ThompsonNo ratings yet
- 2018 - Sample 2Document23 pages2018 - Sample 2David ThompsonNo ratings yet
- Rate of ReactionDocument6 pagesRate of ReactionDavid ThompsonNo ratings yet
- Thompson TD (1) - Layout5-IsO A1 (594 X 841)Document1 pageThompson TD (1) - Layout5-IsO A1 (594 X 841)David ThompsonNo ratings yet
- Development of Shapes 3Document1 pageDevelopment of Shapes 3David ThompsonNo ratings yet
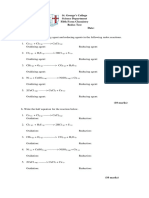
- Redox Worksheet - 5th FormDocument2 pagesRedox Worksheet - 5th FormDavid ThompsonNo ratings yet
- Javier Hague 44 Detail SheetDocument1 pageJavier Hague 44 Detail SheetDavid ThompsonNo ratings yet
- Nathan pdf2Document1 pageNathan pdf2David ThompsonNo ratings yet
- David Thompson - SBA - Section CDocument36 pagesDavid Thompson - SBA - Section CDavid ThompsonNo ratings yet
- Javier Hague 44 Roof PlanDocument1 pageJavier Hague 44 Roof PlanDavid ThompsonNo ratings yet
- Britney Gordon's Resume and Cover Letter PDFDocument4 pagesBritney Gordon's Resume and Cover Letter PDFDavid ThompsonNo ratings yet
- Javier Hague PDFDocument1 pageJavier Hague PDFDavid ThompsonNo ratings yet
- Floor Plan ClassworkDocument1 pageFloor Plan ClassworkDavid ThompsonNo ratings yet
- Javier Hague Floor PlanDocument1 pageJavier Hague Floor PlanDavid ThompsonNo ratings yet
- Development of Shapes 1 PDFDocument1 pageDevelopment of Shapes 1 PDFDavid ThompsonNo ratings yet
- Javier Hague Foundation PlanDocument1 pageJavier Hague Foundation PlanDavid ThompsonNo ratings yet
- Internal TangentDocument1 pageInternal TangentDavid ThompsonNo ratings yet
- Development of Shapes 4 PDFDocument1 pageDevelopment of Shapes 4 PDFDavid ThompsonNo ratings yet
- Drawing word-ISO A1Document1 pageDrawing word-ISO A1David ThompsonNo ratings yet
- Development of Shapes 2 PDFDocument1 pageDevelopment of Shapes 2 PDFDavid ThompsonNo ratings yet
- Development of Shapes 3Document1 pageDevelopment of Shapes 3David ThompsonNo ratings yet
- Unit-1 Administrative Law E-Notes - LLB 208Document20 pagesUnit-1 Administrative Law E-Notes - LLB 208Dinesh GadkariNo ratings yet
- Victorian AgeDocument2 pagesVictorian AgeMaria vittoria SodaNo ratings yet
- The Corporation: I. Chapter OutlineDocument3 pagesThe Corporation: I. Chapter Outlinehung TranNo ratings yet
- Test Bank For Essentials of Business Law and The Legal Environment 11th Edition Richard A MannDocument11 pagesTest Bank For Essentials of Business Law and The Legal Environment 11th Edition Richard A MannRicky Mchendry100% (40)
- TC66-Series Cone Crushers IOM Manual - Rev.4 - Conos Trio LinderosDocument74 pagesTC66-Series Cone Crushers IOM Manual - Rev.4 - Conos Trio LinderosFrancisco Vera100% (3)
- CBRE Hotel Insights The Vietnam MarketDocument5 pagesCBRE Hotel Insights The Vietnam MarketVu Le MinhNo ratings yet
- ENA Nurses CODE OF ETHICSDocument16 pagesENA Nurses CODE OF ETHICSAMANUEL NUREDIN80% (10)
- Introduction: Linguistic Processes and The Reproduction of Gender BiasDocument22 pagesIntroduction: Linguistic Processes and The Reproduction of Gender BiasNgoc Anh Thi LoNo ratings yet
- StoreProcedure 2004 LDCE Question - Paper PDFDocument5 pagesStoreProcedure 2004 LDCE Question - Paper PDFmurthy g100% (2)
- Understanding Rape: Described by Professionals Within The Justice SystemDocument23 pagesUnderstanding Rape: Described by Professionals Within The Justice SystemHera FakherNo ratings yet
- The Arrow's Impossibility Theorem: The Paradox of DemocracyDocument35 pagesThe Arrow's Impossibility Theorem: The Paradox of DemocracyHafsa JahanNo ratings yet
- Fundamental RulesDocument18 pagesFundamental RulesrakeshNo ratings yet
- Write A Reflection Paper On How The Concept of OFW Supports The Disparity Between 1, 2 and 3 World CountriesDocument2 pagesWrite A Reflection Paper On How The Concept of OFW Supports The Disparity Between 1, 2 and 3 World CountriesJoyce PeñaescociaNo ratings yet
- The Attractor Factor PDFDocument10 pagesThe Attractor Factor PDFbulbtommy50% (2)
- Office/School/Clc Workweek PlanDocument3 pagesOffice/School/Clc Workweek PlanAlbinMae Caroline Intong-Torres Bracero-CuyosNo ratings yet
- Deepanshu Bhardwaj - Offer LetterDocument4 pagesDeepanshu Bhardwaj - Offer Letter4424qpzkzmNo ratings yet
- Insolvency & Bankruptcy Code, 2016Document23 pagesInsolvency & Bankruptcy Code, 2016Jeswin JohnNo ratings yet
- Articles 689, EtcDocument28 pagesArticles 689, EtcSla DettabaliNo ratings yet
- Cambridge IGCSE: HISTORY 0470/11Document12 pagesCambridge IGCSE: HISTORY 0470/11Muras BaiyshevNo ratings yet
- AXA Loan Application Form v2019 (All Entities)Document2 pagesAXA Loan Application Form v2019 (All Entities)Jon EsberNo ratings yet
- The Mindset and Practices of Excellent CEO S - 1572287515Document11 pagesThe Mindset and Practices of Excellent CEO S - 1572287515Adrián ReinalttNo ratings yet
- Reflection SablasDocument2 pagesReflection SablasAlyza SablasNo ratings yet
- Business Ethics and Social ResponsibilityDocument35 pagesBusiness Ethics and Social ResponsibilityMelody FabreagNo ratings yet
- Org Chart & Seating PlanDocument2 pagesOrg Chart & Seating PlanNur Marini Nabilah MazlanNo ratings yet
- Your Offer Letter,,,,.Document2 pagesYour Offer Letter,,,,.Süñîl Åñîl PäťïlNo ratings yet
- 2018 OSC Memo: Non-Disclosure UpdateDocument4 pages2018 OSC Memo: Non-Disclosure UpdateFedSmith Inc.No ratings yet
- Erlanger & Galinger vs. Swedish East Asiatic Co., LTD., 34 Phil. 178, No. 10051 March 9, 1916Document38 pagesErlanger & Galinger vs. Swedish East Asiatic Co., LTD., 34 Phil. 178, No. 10051 March 9, 1916Marl Dela ROsaNo ratings yet
- Palacio vs. Fely Transportation Co., 5 SCRA 1011 (1962)Document3 pagesPalacio vs. Fely Transportation Co., 5 SCRA 1011 (1962)VINCENTREY BERNARDONo ratings yet