Download as pdf or txt
You might also like
- 6int 2005 Jun QDocument9 pages6int 2005 Jun Qapi-19836745No ratings yet
- Everythings An Argument NotesDocument4 pagesEverythings An Argument Notesjumurph100% (1)
- Final Version of HIV ResearchDocument29 pagesFinal Version of HIV ResearchJordan Abosama MamalumpongNo ratings yet
- State of Hivaids Epidemic in Urban Areas in Kwazulu-Natal, South AfricaDocument21 pagesState of Hivaids Epidemic in Urban Areas in Kwazulu-Natal, South AfricaNoor Ul HassanNo ratings yet
- Keaslian 3 Di PakaiDocument10 pagesKeaslian 3 Di PakaiAfraNo ratings yet
- Aids 33 s283Document12 pagesAids 33 s283ilhamfajriNo ratings yet
- HIV and AIDs Status in NigeriaDocument15 pagesHIV and AIDs Status in NigeriaRufai HarunaNo ratings yet
- Journal 2Document6 pagesJournal 2Anastasia ApriliaNo ratings yet
- 6030 14907 1 PBDocument7 pages6030 14907 1 PBnovaariani903No ratings yet
- Epidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014Document6 pagesEpidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014jessicaNo ratings yet
- Rifal MijuDocument10 pagesRifal MijuSAFIRA FAUZIANA THAHARNo ratings yet
- Situasi DBD Di Indonesia. Pusat Data Dan Informasi Kementrian Kesehatan RI.2016Document6 pagesSituasi DBD Di Indonesia. Pusat Data Dan Informasi Kementrian Kesehatan RI.2016El Alsha AndiniNo ratings yet
- Reference ThesisDocument13 pagesReference ThesisGhina SalsabilaNo ratings yet
- The Rise of Imported Dengue Infections in Victoria, Australia, 2010-2016Document11 pagesThe Rise of Imported Dengue Infections in Victoria, Australia, 2010-2016Satriya WibawaNo ratings yet
- Covid NigeriaDocument5 pagesCovid NigeriaPriscy CandoNo ratings yet
- Spatial and Temporal Pattern of Drug Resistant TB in South South NigeriaDocument12 pagesSpatial and Temporal Pattern of Drug Resistant TB in South South Nigeriaijmb333No ratings yet
- Cohorte 10 PDFDocument7 pagesCohorte 10 PDFLaura MottaNo ratings yet
- Increase in Tuberculosis Cases Among Prisoners, Brazil, 2009-2014Document4 pagesIncrease in Tuberculosis Cases Among Prisoners, Brazil, 2009-2014Camila da Silva SouzaNo ratings yet
- Incidence Predictors Poor Outcome Childhood TB North Cameroun ADB 1Document15 pagesIncidence Predictors Poor Outcome Childhood TB North Cameroun ADB 1Elie Junior Olomo NdjambouNo ratings yet
- Tuberculosis ArticleDocument7 pagesTuberculosis ArticleMaria BacasnoNo ratings yet
- Determinant Factors of Drop Out (Do) Among Multi Drugs Resistance Tuberculosis (MDR TB) Patients at Jakarta Province in 2011 To 2015Document6 pagesDeterminant Factors of Drop Out (Do) Among Multi Drugs Resistance Tuberculosis (MDR TB) Patients at Jakarta Province in 2011 To 2015eis kusmitaNo ratings yet
- Challenges of Measuring The Healthcare Access andDocument1 pageChallenges of Measuring The Healthcare Access andJIO MALENKONo ratings yet
- Ministry of Education and Scientific Research) ) Al-Muthanna University College of Medicine) )Document13 pagesMinistry of Education and Scientific Research) ) Al-Muthanna University College of Medicine) )Hussein H. MahmoodNo ratings yet
- 086-092 49958+nursalamDocument7 pages086-092 49958+nursalamSALSABILA RAHMA REFFANANANo ratings yet
- Sociodemographic Characteristics of Patients With Advanced HIV Disease in Enugu, South-East Nigeria: A Retrospective Analysis of Program DataDocument6 pagesSociodemographic Characteristics of Patients With Advanced HIV Disease in Enugu, South-East Nigeria: A Retrospective Analysis of Program DataInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- HIV-TB Co-Infection With Clinical PresentationDocument6 pagesHIV-TB Co-Infection With Clinical PresentationMarcellia AngelinaNo ratings yet
- 75-Article Text-329-1-10-20220929Document16 pages75-Article Text-329-1-10-20220929BrianNo ratings yet
- Piaa 030Document10 pagesPiaa 030Suryadi LimardiNo ratings yet
- Increased Age-Adjusted Cancer Mortality After The 3rd mRNA-Lipid Nanoparticle Vaccine Dose During The COVID-19 Pandemic in JapanDocument14 pagesIncreased Age-Adjusted Cancer Mortality After The 3rd mRNA-Lipid Nanoparticle Vaccine Dose During The COVID-19 Pandemic in JapandanielnagaseNo ratings yet
- Dynamic Modeling of Hepatitis C Transmission Among People Who InjectDocument16 pagesDynamic Modeling of Hepatitis C Transmission Among People Who InjectFAIZALNo ratings yet
- SARS-CoV-2 Infections and COVID-19 Fatality EstimaDocument12 pagesSARS-CoV-2 Infections and COVID-19 Fatality EstimaAmanda WrightNo ratings yet
- Fakultas Kesehatan Masyarakat, Universitas Halu Oleo, Kendari Fakultas Ilmu Kesehatan, Universitas Tribhuwana Tunggadewi, MalangDocument13 pagesFakultas Kesehatan Masyarakat, Universitas Halu Oleo, Kendari Fakultas Ilmu Kesehatan, Universitas Tribhuwana Tunggadewi, MalangDoni FitraNo ratings yet
- Tuberculosis Among Migrant WorDocument8 pagesTuberculosis Among Migrant WorBimaSuryaNo ratings yet
- Uses of Statistical Methodology in HIV/AIDS Projections: Ramesh S. Patil, Sajjan C.G. and Nagaraja Rao CDocument14 pagesUses of Statistical Methodology in HIV/AIDS Projections: Ramesh S. Patil, Sajjan C.G. and Nagaraja Rao CSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- 5 Revista Internacional de ESalud y Comunicaciones MdicasDocument21 pages5 Revista Internacional de ESalud y Comunicaciones MdicaslauraNo ratings yet
- Surveilans HIV Di Kabupaten JemberDocument10 pagesSurveilans HIV Di Kabupaten Jemberafifah.nurfaidahNo ratings yet
- Sexually Transmitted Infections and Associated Risk Factors Among Male Clients of Sex Workers-, A Cross-Sectional Pilot Project in Antwerp, BelgiumDocument7 pagesSexually Transmitted Infections and Associated Risk Factors Among Male Clients of Sex Workers-, A Cross-Sectional Pilot Project in Antwerp, BelgiumFrans LandiNo ratings yet
- The Tuberculosis Profi Le of The Philippines, 2003-2011: Advancing DOTS and BeyondDocument6 pagesThe Tuberculosis Profi Le of The Philippines, 2003-2011: Advancing DOTS and BeyondAprez SyahvaliaNo ratings yet
- Seroprevalence of COVID-19 Infection in A Rural District of South India: A Population-Based Seroepidemiological StudyDocument11 pagesSeroprevalence of COVID-19 Infection in A Rural District of South India: A Population-Based Seroepidemiological StudySANAULLAH SULTANPURNo ratings yet
- Medi 102 E32811Document9 pagesMedi 102 E32811dani catriaNo ratings yet
- Simpore2006-Toxoplasma Gondii, HCV, and HBV SeroprevalenceDocument4 pagesSimpore2006-Toxoplasma Gondii, HCV, and HBV Seroprevalenceizvery.badNo ratings yet
- Assessing The Burden of Dengue Among Household Members in Alaminos Laguna The Philippines A Prospective Cohort StudyDocument10 pagesAssessing The Burden of Dengue Among Household Members in Alaminos Laguna The Philippines A Prospective Cohort Studyfigin86893No ratings yet
- 4 IndonesiaDocument12 pages4 IndonesiaGyanNurmaindahHendiantiNo ratings yet
- Joenputri N2020Document5 pagesJoenputri N2020ichaNo ratings yet
- TB 2Document5 pagesTB 2Shyenette SarmientoNo ratings yet
- Spatial Epidemiology and Climatic Predictors of Paediatric Dengue Infections Captured Via Sentinel Site Surveillance, Phnom Penh Cambodia 2011 - 2012Document8 pagesSpatial Epidemiology and Climatic Predictors of Paediatric Dengue Infections Captured Via Sentinel Site Surveillance, Phnom Penh Cambodia 2011 - 2012Andrew HukomNo ratings yet
- Burden and Consequences of Tuberculosis Among HIV-Infected Individuals Insights From The Itojo Hospital HIV Clinic in Ntungamo DistrictDocument8 pagesBurden and Consequences of Tuberculosis Among HIV-Infected Individuals Insights From The Itojo Hospital HIV Clinic in Ntungamo DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Revealed That: Among New and Among Re-Treatment TB Cases Had MDR-TBDocument32 pagesRevealed That: Among New and Among Re-Treatment TB Cases Had MDR-TBComingSoonNo ratings yet
- Jalalpur Jattan Case StudyDocument8 pagesJalalpur Jattan Case Studyduracell19No ratings yet
- Effects of COVID-19 On Parkinson Disease Clinical Features - A CMDocument12 pagesEffects of COVID-19 On Parkinson Disease Clinical Features - A CMAntonyNo ratings yet
- World TB Day - March 24, 2020 Global Epidemiology of Tuberculosis and Progress Toward Meeting Global Targets - Worldwide, 2018Document5 pagesWorld TB Day - March 24, 2020 Global Epidemiology of Tuberculosis and Progress Toward Meeting Global Targets - Worldwide, 2018elburouj.pokemonNo ratings yet
- Telaah Jurnal Aditya Adella PratamaDocument35 pagesTelaah Jurnal Aditya Adella PratamaGemantri veyonda ZikryNo ratings yet
- JUrnalnya PBL 1Document7 pagesJUrnalnya PBL 1Siti Zahra MaharaniNo ratings yet
- Report 34: COVID-19 Infection Fatality Ratio: Estimates From SeroprevalenceDocument18 pagesReport 34: COVID-19 Infection Fatality Ratio: Estimates From SeroprevalenceIonuț AlexandrescuNo ratings yet
- Research Paper On Dengue Fever in PakistanDocument6 pagesResearch Paper On Dengue Fever in Pakistangvzz4v44100% (1)
- Maternal Mortality Ratio - Trends in The Vital Registration DataDocument4 pagesMaternal Mortality Ratio - Trends in The Vital Registration DataadskvcdsNo ratings yet
- DEATH STATISTICS - IFR 0.23% - Infection Fatality Rate of COVID-19 - John P A IoannidisDocument37 pagesDEATH STATISTICS - IFR 0.23% - Infection Fatality Rate of COVID-19 - John P A IoannidisPeter100% (1)
- 1 Line Treatment Outcomes of The New Pulmonary Bacteriologically Confirmed TB Cases (2012 Cohort, %)Document34 pages1 Line Treatment Outcomes of The New Pulmonary Bacteriologically Confirmed TB Cases (2012 Cohort, %)ComingSoonNo ratings yet
- Journal Reading HIVDocument20 pagesJournal Reading HIVayuni fatriciaNo ratings yet
- Prevalence of Malaria Among Patients at The Sino-Gabonese Friendship Hospital in Franceville A Two-Year Retrospective StudyDocument8 pagesPrevalence of Malaria Among Patients at The Sino-Gabonese Friendship Hospital in Franceville A Two-Year Retrospective StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 s2.0 S1746809421000914 MainDocument8 pages1 s2.0 S1746809421000914 MainFernando DaudNo ratings yet
- Telemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.From EverandTelemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.No ratings yet
- St. Martin vs. LWVDocument2 pagesSt. Martin vs. LWVBaby T. Agcopra100% (5)
- Commets Muhammed ProposalDocument38 pagesCommets Muhammed ProposalMohammed HussenNo ratings yet
- CIR Vs RhombusDocument2 pagesCIR Vs RhombusKateBarrionEspinosaNo ratings yet
- India - Sri Lanka HVDC InterconnectionDocument2 pagesIndia - Sri Lanka HVDC InterconnectionsukhadiadarshanNo ratings yet
- Attendance DenmarkDocument3 pagesAttendance Denmarkdennis berja laguraNo ratings yet
- Constitution Template For Mobile Legends Esports ClubDocument5 pagesConstitution Template For Mobile Legends Esports Clubpcipm pcipmsebrangulu2plgNo ratings yet
- Social Science PortfolioDocument2 pagesSocial Science Portfoliorajesh duaNo ratings yet
- 3 MicroDocument4 pages3 MicroDumitraNo ratings yet
- Tata Acquired Luxury Auto Brands Jaguar and Land Rover - From Ford MotorsDocument15 pagesTata Acquired Luxury Auto Brands Jaguar and Land Rover - From Ford MotorsJoel SaldanhaNo ratings yet
- Bimco - FPD Booklet 2012Document32 pagesBimco - FPD Booklet 2012Reda HmrNo ratings yet
- Module 24Document140 pagesModule 24api-278516771No ratings yet
- Report of Monument and PatternsDocument23 pagesReport of Monument and PatternsMAHEEN FATIMANo ratings yet
- Imogene M. King - Theory of Goal AttainmentDocument18 pagesImogene M. King - Theory of Goal AttainmentLouis Gabriel AdayaNo ratings yet
- UNIT 8 Types of Punishment For Crimes RedactataDocument17 pagesUNIT 8 Types of Punishment For Crimes Redactataanna825020No ratings yet
- View Full-Featured Version: Send To PrinterDocument5 pagesView Full-Featured Version: Send To PrinteremmanjabasaNo ratings yet
- Assignment 01 MemberManagementDocument9 pagesAssignment 01 MemberManagementDinh Huu Khang (K16HCM)No ratings yet
- Satire Powerpoint Without PicsDocument19 pagesSatire Powerpoint Without Picsapi-300762638No ratings yet
- Quiz - BRITISH AMERICAN CULTUREDocument16 pagesQuiz - BRITISH AMERICAN CULTUREK28 Chuyên Tin CHLNo ratings yet
- Ramon DistrictDocument1 pageRamon DistrictPad-ay Jasmin IrisNo ratings yet
- Latihan Soal Chapter 7 Kelas ViiiDocument3 pagesLatihan Soal Chapter 7 Kelas ViiiChalwa AnjumitaNo ratings yet
- Custody ServiceDocument4 pagesCustody ServicemuffadNo ratings yet
- LLM Advice - All You Need To Know About Statement of Purpose (SOP)Document20 pagesLLM Advice - All You Need To Know About Statement of Purpose (SOP)Seema ChauhanNo ratings yet
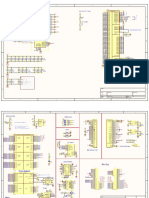
- Maix BitDocument2 pagesMaix BitloborisNo ratings yet
- Grammar g3Document3 pagesGrammar g3Future Stars SchoolNo ratings yet
- Rizal Life Works BL Guide Quiz 12 and PrelimDocument15 pagesRizal Life Works BL Guide Quiz 12 and PrelimCarla Mae Alcantara100% (1)
- DF MCQ 1Document7 pagesDF MCQ 1SAI RAMAN67% (6)
- Manual For Conflict AnalysisDocument38 pagesManual For Conflict AnalysisNadine KadriNo ratings yet
- Mindmap For Hands Held HighDocument1 pageMindmap For Hands Held Highapi-523333030No ratings yet