
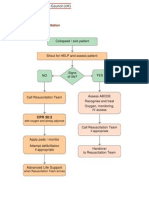
(Pre-Hospital) Adult Basic Life Support: Unresponsive
(Pre-Hospital) Adult Basic Life Support: Unresponsive
You might also like
- BLS PDFDocument6 pagesBLS PDFAyesha Jadoon80% (5)
- Scenarios For RevisionDocument16 pagesScenarios For RevisionJadon PunshonNo ratings yet
- Presentation TOT KDM Pend. Khas - 22 April 2015Document4 pagesPresentation TOT KDM Pend. Khas - 22 April 2015Jocelyn WongNo ratings yet
- Paediatric ALS A3Document1 pagePaediatric ALS A3Ali HusseinNo ratings yet
- Cardiac Arrest Advanced Life Support PDFDocument1 pageCardiac Arrest Advanced Life Support PDFCristina TrofimovNo ratings yet
- Cardiac Arrest Advanced Life SupportDocument1 pageCardiac Arrest Advanced Life SupportCristina TrofimovNo ratings yet
- 1 AlgorithmsDocument19 pages1 AlgorithmsRiya Sood100% (1)
- Cardiopulmonary Resuscitation: Dr. Abdul Rashad Senior Lecturer United College of Physical TherapyDocument27 pagesCardiopulmonary Resuscitation: Dr. Abdul Rashad Senior Lecturer United College of Physical TherapypashaNo ratings yet
- BLS Healthcare Provider AlgorithmDocument7 pagesBLS Healthcare Provider AlgorithmyuniNo ratings yet
- Healthcare CPR Cheat Sheet: Check The SceneDocument2 pagesHealthcare CPR Cheat Sheet: Check The SceneRocel Marie SullestaNo ratings yet
- PBLSposterDocument1 pagePBLSposterJose SesmeroNo ratings yet
- Resuscitation Guidelines: To Download A Copy of This Handout, or For Further Information Please VisitDocument4 pagesResuscitation Guidelines: To Download A Copy of This Handout, or For Further Information Please Visitcxz4321No ratings yet
- First Aid: Onboard VesselsDocument14 pagesFirst Aid: Onboard VesselsMico YogoreNo ratings yet
- In Hospital AlgoDocument1 pageIn Hospital Algozacklim_2000No ratings yet
- Basic Life Support PUSKESDocument16 pagesBasic Life Support PUSKESHend SuryaNo ratings yet
- AlgorithmBLS Ped CA Single RescuerCOVID 200406Document1 pageAlgorithmBLS Ped CA Single RescuerCOVID 200406Karla HernandezNo ratings yet
- PalsDocument1 pagePalslordroentgenNo ratings yet
- First Aid: TrainingDocument62 pagesFirst Aid: TrainingAyLin Yong100% (1)
- 2005 Aha Bls and Acls SummaryDocument3 pages2005 Aha Bls and Acls SummarypauerishNo ratings yet
- G2015 in Hospital ResuscitationDocument1 pageG2015 in Hospital ResuscitationLily hestiNo ratings yet
- Adult - BLS - PPT 2Document49 pagesAdult - BLS - PPT 2urjaNo ratings yet
- Healthcare Provider CAB of CPR Helpful HintsDocument2 pagesHealthcare Provider CAB of CPR Helpful HintsDarrell BrightNo ratings yet
- First AidDocument35 pagesFirst AidKrishna Patel100% (1)
- Fbao Protocols Conscious To Unconscious - Infant Care (2010 Ecc Guidelines Applied)Document1 pageFbao Protocols Conscious To Unconscious - Infant Care (2010 Ecc Guidelines Applied)Aleksandar PetrovicNo ratings yet
- Pediatric CPRDocument6 pagesPediatric CPRAnserinNo ratings yet
- CPR For ChildDocument19 pagesCPR For Childicuanak anakicuNo ratings yet
- Final-OPIDO (SN) - BSN 407 - CPRDocument1 pageFinal-OPIDO (SN) - BSN 407 - CPRrodolfo opidoNo ratings yet
- Algorithm-BLS Ped 2 Rescuers 200624Document1 pageAlgorithm-BLS Ped 2 Rescuers 200624Omar BalfaqeehNo ratings yet
- Basic Life SupportDocument2 pagesBasic Life SupportAhmad Khair Ahmad BazliNo ratings yet
- Adult Basic Life Support 2015Document44 pagesAdult Basic Life Support 2015A A Putri Sukma WardiniNo ratings yet
- BLS + CPRDocument3 pagesBLS + CPRM7md Al-HuwaitiNo ratings yet
- Basic Life SuppDocument46 pagesBasic Life SuppDiana Garcia SaclutiNo ratings yet
- Aneasth.2 - PHCP2Document11 pagesAneasth.2 - PHCP2أحمد أسامهNo ratings yet
- Abdulfattah Alhazmi Ayhazmi@uqu - Edu.saDocument18 pagesAbdulfattah Alhazmi Ayhazmi@uqu - Edu.saعبدالرحمن الحربيNo ratings yet
- Dr. Kunal Jhaveri (MD)Document42 pagesDr. Kunal Jhaveri (MD)Bhaskar Äðítýæ Phatak100% (1)
- BLS Manual 2013Document13 pagesBLS Manual 2013Algean AloNo ratings yet
- Raka Jati P: Dept. Anestesiologi Dan Terapi Intensif Fakultas Kedokteran USU/RSUP. H. Adam Malik MedanDocument56 pagesRaka Jati P: Dept. Anestesiologi Dan Terapi Intensif Fakultas Kedokteran USU/RSUP. H. Adam Malik MedanDaniel Aprianto SihotangNo ratings yet
- CWTS ReviewerDocument5 pagesCWTS ReviewerJedine SachiNo ratings yet
- Basic Life SupportDocument22 pagesBasic Life SupportDhiren PranamiNo ratings yet
- Bantuan Hidup Dasar Guideline 2010: Revision of Guidelines 2000 Guidelines 2005Document48 pagesBantuan Hidup Dasar Guideline 2010: Revision of Guidelines 2000 Guidelines 2005Yuly Fajar SariNo ratings yet
- Basic Life SupportDocument11 pagesBasic Life SupportUtkrisht Shah100% (1)
- Basic Life Support CPRDocument44 pagesBasic Life Support CPRJasmin KulanićNo ratings yet
- CPR Basic Life SupportDocument25 pagesCPR Basic Life SupportShikya AbnasNo ratings yet
- Basic Life Support (Cardiopulmonary Resuscitation) : Respiratory Cardiac ArrestDocument3 pagesBasic Life Support (Cardiopulmonary Resuscitation) : Respiratory Cardiac Arreststeve jaymeNo ratings yet
- Pocket Book of Hospital Care For Children - Guidleines For The Management of Common Illnesses With Limited Resources. (2012, World Health Organization)Document442 pagesPocket Book of Hospital Care For Children - Guidleines For The Management of Common Illnesses With Limited Resources. (2012, World Health Organization)Sadia YousafNo ratings yet
- BLS Code Card - Basic Life Support Adults and AdolescentsDocument2 pagesBLS Code Card - Basic Life Support Adults and AdolescentsphuongNo ratings yet
- CPR Guideline 2022Document12 pagesCPR Guideline 2022Wyndham WooNo ratings yet
- Raka Jati P: Dept. Anestesiologi Dan Terapi Intensif Fakultas Kedokteran USU/RSUP. H. Adam Malik MedanDocument56 pagesRaka Jati P: Dept. Anestesiologi Dan Terapi Intensif Fakultas Kedokteran USU/RSUP. H. Adam Malik MedanRony ArzalNo ratings yet
- Cardiopulmonary Resuscitation: Yohanes Rudijanto, DR., SpanDocument63 pagesCardiopulmonary Resuscitation: Yohanes Rudijanto, DR., SpanPadrepio R RahadiNo ratings yet
- BLS Study Guide and PretestDocument47 pagesBLS Study Guide and PretestRicha AbcedeNo ratings yet
- Emergency Aid Presentation - V4Document43 pagesEmergency Aid Presentation - V4Smpp MondhaNo ratings yet
- Algoritmos en PandemiaDocument5 pagesAlgoritmos en PandemiaRafael MejiaNo ratings yet
- Masuri Prim AjutorDocument143 pagesMasuri Prim AjutorReka Drincal100% (1)
- Bantuan Hidup DasarDocument33 pagesBantuan Hidup DasarFrederica MutiaraNo ratings yet
- Dart BLS CPR With AEDDocument27 pagesDart BLS CPR With AEDLucas WangNo ratings yet
- Adult BLSDocument69 pagesAdult BLSShajahan SideequeNo ratings yet
- Bls Amsep Ina For ThaiDocument46 pagesBls Amsep Ina For ThaiRaissa Alfaathir HeriNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- First Aid & Emergency Companions: First Aid & Emergencies at SeaFrom EverandFirst Aid & Emergency Companions: First Aid & Emergencies at SeaNo ratings yet
- Exercise Tolerance TestingDocument15 pagesExercise Tolerance TestingPratyaksha TiwariNo ratings yet
- Biology - MYP 3 - 31st AugustDocument6 pagesBiology - MYP 3 - 31st Augustarchit.kulkarni7756No ratings yet
- Informe DEMO Del Holter de Arritmia Contec TLC9803Document14 pagesInforme DEMO Del Holter de Arritmia Contec TLC9803Edward MoralesNo ratings yet
- Diara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineDocument19 pagesDiara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineJara RogacionNo ratings yet
- Modified Duke's Criteria For Infective Endocarditis - Mnemonic - EpomedicineDocument5 pagesModified Duke's Criteria For Infective Endocarditis - Mnemonic - EpomedicineAsmaNo ratings yet
- Materi Dasar EkgDocument52 pagesMateri Dasar EkgFirsandiPrasastyaFikryGozali100% (2)
- ECG in Emergency MedicineDocument228 pagesECG in Emergency MedicineM.FADLINo ratings yet
- Dr. Atif Sher ASCVD CardioConDocument21 pagesDr. Atif Sher ASCVD CardioConwali ahmedNo ratings yet
- Acls Pretest Answer Key: Rhythm Identification (Part I)Document3 pagesAcls Pretest Answer Key: Rhythm Identification (Part I)aditNo ratings yet
- Qrs Complexes: Fast & Easy Ecgs - A Self-Paced Learning ProgramDocument49 pagesQrs Complexes: Fast & Easy Ecgs - A Self-Paced Learning ProgramMuhammad Hatta HamzahNo ratings yet
- دليل الأمراض الشائعة للأطباء-1Document148 pagesدليل الأمراض الشائعة للأطباء-1Ibrahim RamizNo ratings yet
- ArrhythmiasDocument23 pagesArrhythmiasKelvin Mandela100% (1)
- Congenital Heart DiseaseDocument82 pagesCongenital Heart DiseaseDimpal ChoudharyNo ratings yet
- TroponinDocument78 pagesTroponinLidya MustikasariNo ratings yet
- Blockage of The HeartDocument21 pagesBlockage of The HeartLilian EdeniNo ratings yet
- Path of HypertensionDocument52 pagesPath of HypertensionTom TsouNo ratings yet
- PMR Poster TBI Takotsubo AAP 2010 PosterDocument1 pagePMR Poster TBI Takotsubo AAP 2010 PosterjuanvelasquezNo ratings yet
- ACLS ECG Rhythm Strips Pretest Question Answers (Quiz) PDFDocument11 pagesACLS ECG Rhythm Strips Pretest Question Answers (Quiz) PDF김민길100% (1)
- Diet For Cardiovaskular Disease - ErinetaDocument8 pagesDiet For Cardiovaskular Disease - ErinetaErin NettaNo ratings yet
- The Medical Book of Lists A Primer of Differential Diagnosis in PDFDocument260 pagesThe Medical Book of Lists A Primer of Differential Diagnosis in PDFshoko100% (1)
- Basic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalDocument79 pagesBasic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalVeerapong Vattanavanit0% (1)
- Philips DXL 16-Lead ECG Algorithm 0B Criteria Quick GuildDocument15 pagesPhilips DXL 16-Lead ECG Algorithm 0B Criteria Quick GuildHoàng Anh NguyễnNo ratings yet
- Slide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSDocument20 pagesSlide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSsyahrial fazaNo ratings yet
- Bio Investigatory ProjectDocument20 pagesBio Investigatory ProjectMariaNo ratings yet
- Heart BlockDocument26 pagesHeart BlockTrending raze100% (1)
- ECG Study GuideDocument7 pagesECG Study GuideannaNo ratings yet
- High-Sensitivity Cardiac Troponin at Presentation To Rule Out Myocardial Infarction (Historic)Document20 pagesHigh-Sensitivity Cardiac Troponin at Presentation To Rule Out Myocardial Infarction (Historic)DenisseRangelNo ratings yet
- Viskin Et Al 2021 Polymorphic Ventricular Tachycardia Terminology Mechanism Diagnosis and Emergency TherapyDocument17 pagesViskin Et Al 2021 Polymorphic Ventricular Tachycardia Terminology Mechanism Diagnosis and Emergency TherapyMey TalabessyNo ratings yet
- Atrioventricular Spetal Defect Avsd Partial EditDocument2 pagesAtrioventricular Spetal Defect Avsd Partial EditFelicia Shan SugataNo ratings yet
- CardiologyDocument70 pagesCardiologyDharshini MohanNo ratings yet























































































Download as pdf or txt
You might also like
- BLS PDFDocument6 pagesBLS PDFAyesha Jadoon80% (5)
- Scenarios For RevisionDocument16 pagesScenarios For RevisionJadon PunshonNo ratings yet
- Presentation TOT KDM Pend. Khas - 22 April 2015Document4 pagesPresentation TOT KDM Pend. Khas - 22 April 2015Jocelyn WongNo ratings yet
- Paediatric ALS A3Document1 pagePaediatric ALS A3Ali HusseinNo ratings yet
- Cardiac Arrest Advanced Life Support PDFDocument1 pageCardiac Arrest Advanced Life Support PDFCristina TrofimovNo ratings yet
- Cardiac Arrest Advanced Life SupportDocument1 pageCardiac Arrest Advanced Life SupportCristina TrofimovNo ratings yet
- 1 AlgorithmsDocument19 pages1 AlgorithmsRiya Sood100% (1)
- Cardiopulmonary Resuscitation: Dr. Abdul Rashad Senior Lecturer United College of Physical TherapyDocument27 pagesCardiopulmonary Resuscitation: Dr. Abdul Rashad Senior Lecturer United College of Physical TherapypashaNo ratings yet
- BLS Healthcare Provider AlgorithmDocument7 pagesBLS Healthcare Provider AlgorithmyuniNo ratings yet
- Healthcare CPR Cheat Sheet: Check The SceneDocument2 pagesHealthcare CPR Cheat Sheet: Check The SceneRocel Marie SullestaNo ratings yet
- PBLSposterDocument1 pagePBLSposterJose SesmeroNo ratings yet
- Resuscitation Guidelines: To Download A Copy of This Handout, or For Further Information Please VisitDocument4 pagesResuscitation Guidelines: To Download A Copy of This Handout, or For Further Information Please Visitcxz4321No ratings yet
- First Aid: Onboard VesselsDocument14 pagesFirst Aid: Onboard VesselsMico YogoreNo ratings yet
- In Hospital AlgoDocument1 pageIn Hospital Algozacklim_2000No ratings yet
- Basic Life Support PUSKESDocument16 pagesBasic Life Support PUSKESHend SuryaNo ratings yet
- AlgorithmBLS Ped CA Single RescuerCOVID 200406Document1 pageAlgorithmBLS Ped CA Single RescuerCOVID 200406Karla HernandezNo ratings yet
- PalsDocument1 pagePalslordroentgenNo ratings yet
- First Aid: TrainingDocument62 pagesFirst Aid: TrainingAyLin Yong100% (1)
- 2005 Aha Bls and Acls SummaryDocument3 pages2005 Aha Bls and Acls SummarypauerishNo ratings yet
- G2015 in Hospital ResuscitationDocument1 pageG2015 in Hospital ResuscitationLily hestiNo ratings yet
- Adult - BLS - PPT 2Document49 pagesAdult - BLS - PPT 2urjaNo ratings yet
- Healthcare Provider CAB of CPR Helpful HintsDocument2 pagesHealthcare Provider CAB of CPR Helpful HintsDarrell BrightNo ratings yet
- First AidDocument35 pagesFirst AidKrishna Patel100% (1)
- Fbao Protocols Conscious To Unconscious - Infant Care (2010 Ecc Guidelines Applied)Document1 pageFbao Protocols Conscious To Unconscious - Infant Care (2010 Ecc Guidelines Applied)Aleksandar PetrovicNo ratings yet
- Pediatric CPRDocument6 pagesPediatric CPRAnserinNo ratings yet
- CPR For ChildDocument19 pagesCPR For Childicuanak anakicuNo ratings yet
- Final-OPIDO (SN) - BSN 407 - CPRDocument1 pageFinal-OPIDO (SN) - BSN 407 - CPRrodolfo opidoNo ratings yet
- Algorithm-BLS Ped 2 Rescuers 200624Document1 pageAlgorithm-BLS Ped 2 Rescuers 200624Omar BalfaqeehNo ratings yet
- Basic Life SupportDocument2 pagesBasic Life SupportAhmad Khair Ahmad BazliNo ratings yet
- Adult Basic Life Support 2015Document44 pagesAdult Basic Life Support 2015A A Putri Sukma WardiniNo ratings yet
- BLS + CPRDocument3 pagesBLS + CPRM7md Al-HuwaitiNo ratings yet
- Basic Life SuppDocument46 pagesBasic Life SuppDiana Garcia SaclutiNo ratings yet
- Aneasth.2 - PHCP2Document11 pagesAneasth.2 - PHCP2أحمد أسامهNo ratings yet
- Abdulfattah Alhazmi Ayhazmi@uqu - Edu.saDocument18 pagesAbdulfattah Alhazmi Ayhazmi@uqu - Edu.saعبدالرحمن الحربيNo ratings yet
- Dr. Kunal Jhaveri (MD)Document42 pagesDr. Kunal Jhaveri (MD)Bhaskar Äðítýæ Phatak100% (1)
- BLS Manual 2013Document13 pagesBLS Manual 2013Algean AloNo ratings yet
- Raka Jati P: Dept. Anestesiologi Dan Terapi Intensif Fakultas Kedokteran USU/RSUP. H. Adam Malik MedanDocument56 pagesRaka Jati P: Dept. Anestesiologi Dan Terapi Intensif Fakultas Kedokteran USU/RSUP. H. Adam Malik MedanDaniel Aprianto SihotangNo ratings yet
- CWTS ReviewerDocument5 pagesCWTS ReviewerJedine SachiNo ratings yet
- Basic Life SupportDocument22 pagesBasic Life SupportDhiren PranamiNo ratings yet
- Bantuan Hidup Dasar Guideline 2010: Revision of Guidelines 2000 Guidelines 2005Document48 pagesBantuan Hidup Dasar Guideline 2010: Revision of Guidelines 2000 Guidelines 2005Yuly Fajar SariNo ratings yet
- Basic Life SupportDocument11 pagesBasic Life SupportUtkrisht Shah100% (1)
- Basic Life Support CPRDocument44 pagesBasic Life Support CPRJasmin KulanićNo ratings yet
- CPR Basic Life SupportDocument25 pagesCPR Basic Life SupportShikya AbnasNo ratings yet
- Basic Life Support (Cardiopulmonary Resuscitation) : Respiratory Cardiac ArrestDocument3 pagesBasic Life Support (Cardiopulmonary Resuscitation) : Respiratory Cardiac Arreststeve jaymeNo ratings yet
- Pocket Book of Hospital Care For Children - Guidleines For The Management of Common Illnesses With Limited Resources. (2012, World Health Organization)Document442 pagesPocket Book of Hospital Care For Children - Guidleines For The Management of Common Illnesses With Limited Resources. (2012, World Health Organization)Sadia YousafNo ratings yet
- BLS Code Card - Basic Life Support Adults and AdolescentsDocument2 pagesBLS Code Card - Basic Life Support Adults and AdolescentsphuongNo ratings yet
- CPR Guideline 2022Document12 pagesCPR Guideline 2022Wyndham WooNo ratings yet
- Raka Jati P: Dept. Anestesiologi Dan Terapi Intensif Fakultas Kedokteran USU/RSUP. H. Adam Malik MedanDocument56 pagesRaka Jati P: Dept. Anestesiologi Dan Terapi Intensif Fakultas Kedokteran USU/RSUP. H. Adam Malik MedanRony ArzalNo ratings yet
- Cardiopulmonary Resuscitation: Yohanes Rudijanto, DR., SpanDocument63 pagesCardiopulmonary Resuscitation: Yohanes Rudijanto, DR., SpanPadrepio R RahadiNo ratings yet
- BLS Study Guide and PretestDocument47 pagesBLS Study Guide and PretestRicha AbcedeNo ratings yet
- Emergency Aid Presentation - V4Document43 pagesEmergency Aid Presentation - V4Smpp MondhaNo ratings yet
- Algoritmos en PandemiaDocument5 pagesAlgoritmos en PandemiaRafael MejiaNo ratings yet
- Masuri Prim AjutorDocument143 pagesMasuri Prim AjutorReka Drincal100% (1)
- Bantuan Hidup DasarDocument33 pagesBantuan Hidup DasarFrederica MutiaraNo ratings yet
- Dart BLS CPR With AEDDocument27 pagesDart BLS CPR With AEDLucas WangNo ratings yet
- Adult BLSDocument69 pagesAdult BLSShajahan SideequeNo ratings yet
- Bls Amsep Ina For ThaiDocument46 pagesBls Amsep Ina For ThaiRaissa Alfaathir HeriNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- First Aid & Emergency Companions: First Aid & Emergencies at SeaFrom EverandFirst Aid & Emergency Companions: First Aid & Emergencies at SeaNo ratings yet
- Exercise Tolerance TestingDocument15 pagesExercise Tolerance TestingPratyaksha TiwariNo ratings yet
- Biology - MYP 3 - 31st AugustDocument6 pagesBiology - MYP 3 - 31st Augustarchit.kulkarni7756No ratings yet
- Informe DEMO Del Holter de Arritmia Contec TLC9803Document14 pagesInforme DEMO Del Holter de Arritmia Contec TLC9803Edward MoralesNo ratings yet
- Diara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineDocument19 pagesDiara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineJara RogacionNo ratings yet
- Modified Duke's Criteria For Infective Endocarditis - Mnemonic - EpomedicineDocument5 pagesModified Duke's Criteria For Infective Endocarditis - Mnemonic - EpomedicineAsmaNo ratings yet
- Materi Dasar EkgDocument52 pagesMateri Dasar EkgFirsandiPrasastyaFikryGozali100% (2)
- ECG in Emergency MedicineDocument228 pagesECG in Emergency MedicineM.FADLINo ratings yet
- Dr. Atif Sher ASCVD CardioConDocument21 pagesDr. Atif Sher ASCVD CardioConwali ahmedNo ratings yet
- Acls Pretest Answer Key: Rhythm Identification (Part I)Document3 pagesAcls Pretest Answer Key: Rhythm Identification (Part I)aditNo ratings yet
- Qrs Complexes: Fast & Easy Ecgs - A Self-Paced Learning ProgramDocument49 pagesQrs Complexes: Fast & Easy Ecgs - A Self-Paced Learning ProgramMuhammad Hatta HamzahNo ratings yet
- دليل الأمراض الشائعة للأطباء-1Document148 pagesدليل الأمراض الشائعة للأطباء-1Ibrahim RamizNo ratings yet
- ArrhythmiasDocument23 pagesArrhythmiasKelvin Mandela100% (1)
- Congenital Heart DiseaseDocument82 pagesCongenital Heart DiseaseDimpal ChoudharyNo ratings yet
- TroponinDocument78 pagesTroponinLidya MustikasariNo ratings yet
- Blockage of The HeartDocument21 pagesBlockage of The HeartLilian EdeniNo ratings yet
- Path of HypertensionDocument52 pagesPath of HypertensionTom TsouNo ratings yet
- PMR Poster TBI Takotsubo AAP 2010 PosterDocument1 pagePMR Poster TBI Takotsubo AAP 2010 PosterjuanvelasquezNo ratings yet
- ACLS ECG Rhythm Strips Pretest Question Answers (Quiz) PDFDocument11 pagesACLS ECG Rhythm Strips Pretest Question Answers (Quiz) PDF김민길100% (1)
- Diet For Cardiovaskular Disease - ErinetaDocument8 pagesDiet For Cardiovaskular Disease - ErinetaErin NettaNo ratings yet
- The Medical Book of Lists A Primer of Differential Diagnosis in PDFDocument260 pagesThe Medical Book of Lists A Primer of Differential Diagnosis in PDFshoko100% (1)
- Basic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalDocument79 pagesBasic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalVeerapong Vattanavanit0% (1)
- Philips DXL 16-Lead ECG Algorithm 0B Criteria Quick GuildDocument15 pagesPhilips DXL 16-Lead ECG Algorithm 0B Criteria Quick GuildHoàng Anh NguyễnNo ratings yet
- Slide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSDocument20 pagesSlide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSsyahrial fazaNo ratings yet
- Bio Investigatory ProjectDocument20 pagesBio Investigatory ProjectMariaNo ratings yet
- Heart BlockDocument26 pagesHeart BlockTrending raze100% (1)
- ECG Study GuideDocument7 pagesECG Study GuideannaNo ratings yet
- High-Sensitivity Cardiac Troponin at Presentation To Rule Out Myocardial Infarction (Historic)Document20 pagesHigh-Sensitivity Cardiac Troponin at Presentation To Rule Out Myocardial Infarction (Historic)DenisseRangelNo ratings yet
- Viskin Et Al 2021 Polymorphic Ventricular Tachycardia Terminology Mechanism Diagnosis and Emergency TherapyDocument17 pagesViskin Et Al 2021 Polymorphic Ventricular Tachycardia Terminology Mechanism Diagnosis and Emergency TherapyMey TalabessyNo ratings yet
- Atrioventricular Spetal Defect Avsd Partial EditDocument2 pagesAtrioventricular Spetal Defect Avsd Partial EditFelicia Shan SugataNo ratings yet
- CardiologyDocument70 pagesCardiologyDharshini MohanNo ratings yet