Download as pdf or txt
You might also like
- Brooks 5K Beginner Training PlanDocument4 pagesBrooks 5K Beginner Training PlanBrooksRunning0% (2)
- MAPS Starter Blueprints 4Document5 pagesMAPS Starter Blueprints 4Ashutosh Singh100% (1)
- AJAC Bodyweight BodybuildingDocument17 pagesAJAC Bodyweight BodybuildingGermanicus Malmberg100% (2)
- Fifa11+ Poster Referee PDFDocument1 pageFifa11+ Poster Referee PDFAndre LuísNo ratings yet
- The Weight Influenced Self-Esteem Questionnaire (WISE-Q) Factor Structure and Psychometric PropertiesDocument9 pagesThe Weight Influenced Self-Esteem Questionnaire (WISE-Q) Factor Structure and Psychometric PropertiesMagda RossatoNo ratings yet
- .Document11 pages.hey hooNo ratings yet
- TCA - Compte y DuthuDocument4 pagesTCA - Compte y DuthuGaby BarrozoNo ratings yet
- Biceps and Body Image The Relationship Between MusDocument10 pagesBiceps and Body Image The Relationship Between Musmarcewwe10No ratings yet
- Characteristics of Muscle Dysmorphia in Male Football, Weight Training and Bodybuilder 2009Document7 pagesCharacteristics of Muscle Dysmorphia in Male Football, Weight Training and Bodybuilder 2009Magno FilhoNo ratings yet
- Compte & Duthu, 2015Document3 pagesCompte & Duthu, 2015Emilio J. CompteNo ratings yet
- Psychosocial Predictors of Drive For Muscularity in Male Colle - 2015 - Body ImaDocument5 pagesPsychosocial Predictors of Drive For Muscularity in Male Colle - 2015 - Body ImaCarolina CamoesasNo ratings yet
- Unconditional AcceptanceDocument10 pagesUnconditional AcceptanceIoanna NannaNo ratings yet
- Lantz 2002Document7 pagesLantz 2002Robert FluoroCarbonNo ratings yet
- The Body DissatisfactionDocument15 pagesThe Body DissatisfactionAsmah GhazaliNo ratings yet
- Critical Factors of Social Physique Anxiety: Exercising and Body Image SatisfactionDocument12 pagesCritical Factors of Social Physique Anxiety: Exercising and Body Image Satisfactionfotinimavr94No ratings yet
- BBRC Vol 14 No 04 2021-91Document5 pagesBBRC Vol 14 No 04 2021-91Dr Sharique AliNo ratings yet
- Louw 2012 - Sample Article On Correlates (Easy To Understand) 1Document11 pagesLouw 2012 - Sample Article On Correlates (Easy To Understand) 1Christopher LeNo ratings yet
- Escala de Dependencia Do Exercicio Fisico - ENDocument20 pagesEscala de Dependencia Do Exercicio Fisico - ENBruna MacedoNo ratings yet
- Healy 2018Document16 pagesHealy 2018Nahara LimaNo ratings yet
- Body ImageDocument18 pagesBody ImageDewa SatyaNo ratings yet
- LESSON 3 and 4 Module 2Document16 pagesLESSON 3 and 4 Module 2Jerry PalarionNo ratings yet
- Dismorfia Muscular, Imagen Corporal y Conductas Alimentarioas en Dos Poblaciones MasculinasDocument9 pagesDismorfia Muscular, Imagen Corporal y Conductas Alimentarioas en Dos Poblaciones Masculinasamandarhp12No ratings yet
- Body Concerns Ex Behaviour PaperDocument16 pagesBody Concerns Ex Behaviour PaperMohit KharbandaNo ratings yet
- Body Image Binge EatingDocument7 pagesBody Image Binge EatingangelaNo ratings yet
- Exercise Performance: LessonDocument5 pagesExercise Performance: LessonBOSSMEYJNo ratings yet
- Rosen Et Al, 1995Document8 pagesRosen Et Al, 1995DiegoNo ratings yet
- Assessment of Body Image Flexibility - BIAAQDocument11 pagesAssessment of Body Image Flexibility - BIAAQomsohamomNo ratings yet
- Applied Statistics Project Group No. 5 Section ADocument7 pagesApplied Statistics Project Group No. 5 Section AmadihaNo ratings yet
- Desouza2007 PDFDocument9 pagesDesouza2007 PDFAndra SpatarNo ratings yet
- 14 613 1 PBDocument7 pages14 613 1 PBVanessa Cruz RuizNo ratings yet
- Body Image Dissatisfaction: Gender Differences in Eating Attitudes, Self-Esteem, and Reasons For ExerciseDocument18 pagesBody Image Dissatisfaction: Gender Differences in Eating Attitudes, Self-Esteem, and Reasons For ExerciseNimic NimicNo ratings yet
- The Efficacy of A 9-Month Treadmill Walking Program On The Exercise Capacity and Weight Reduction For Adolescents With Severe AutismDocument10 pagesThe Efficacy of A 9-Month Treadmill Walking Program On The Exercise Capacity and Weight Reduction For Adolescents With Severe AutismmarikosvaNo ratings yet
- Muscle Dysmorphia: Could It Be Classified As An Addiction To Body Image?Document6 pagesMuscle Dysmorphia: Could It Be Classified As An Addiction To Body Image?Clau CobosNo ratings yet
- Drive For Muscularity Behaviors in Male BodybuildeDocument12 pagesDrive For Muscularity Behaviors in Male BodybuildeIndrashis MandalNo ratings yet
- Final Paper ProposalDocument13 pagesFinal Paper Proposalseanchiu0812No ratings yet
- Rosen 1996Document12 pagesRosen 1996pilaralonsorobledoNo ratings yet
- Nemer Off 1994Document10 pagesNemer Off 1994saadsffggeettrgbfbfbftggrg ergrtertererefrerrNo ratings yet
- Does Self Esteem Moderate The Relation Between Gender and WeightDocument11 pagesDoes Self Esteem Moderate The Relation Between Gender and Weightmurilo rodriguesNo ratings yet
- Body Image Dissatisfaction: Gender Differences Eating Attitudes, Self-Esteem, and Reasons For ExerciseDocument16 pagesBody Image Dissatisfaction: Gender Differences Eating Attitudes, Self-Esteem, and Reasons For Exerciseiusti iNo ratings yet
- Study of Physical Fitness Index Using Modified Harvard Step Test in Relation With Body Mass Index in Physiotherapy StudentsDocument4 pagesStudy of Physical Fitness Index Using Modified Harvard Step Test in Relation With Body Mass Index in Physiotherapy StudentsUswatun HasanahNo ratings yet
- Improving Health Related Fitness in Adolescents The CrossFit Teens Randomised Controlled TrialDocument16 pagesImproving Health Related Fitness in Adolescents The CrossFit Teens Randomised Controlled TrialChi Chung CHANNo ratings yet
- La Actividad Fisica y Los HuesosDocument10 pagesLa Actividad Fisica y Los HuesosyatibaduizaNo ratings yet
- The Effect of Different Response Formats On Ratings of Exerciser StereotypesDocument12 pagesThe Effect of Different Response Formats On Ratings of Exerciser StereotypesCarmarie Figueroa BenítezNo ratings yet
- Ivan 2Document5 pagesIvan 2Kamal Singh BhandariNo ratings yet
- Goal, Self EfficacyDocument17 pagesGoal, Self EfficacyAlexandra HNo ratings yet
- Amy FordDocument18 pagesAmy FordJaneNo ratings yet
- The Role of Stigmatizing Experiences MILKEWICZ ANNIS CASH HRABOSKYDocument13 pagesThe Role of Stigmatizing Experiences MILKEWICZ ANNIS CASH HRABOSKYGonzalo PaezNo ratings yet
- Building Strength: Strength Training Atti-Tudes and Behaviors of All-Women's and Coed Gym ExercisersDocument15 pagesBuilding Strength: Strength Training Atti-Tudes and Behaviors of All-Women's and Coed Gym ExercisersLaura Perez HoyosNo ratings yet
- Behavioral and Psychological Implications of Body Dissatisfaction: Do Men and Women Differ?Document14 pagesBehavioral and Psychological Implications of Body Dissatisfaction: Do Men and Women Differ?Jeral PerezNo ratings yet
- Effects of Physical Exercise in Older Adults With Reduced Physical Capacity Meta-Analysis of Resistance Exercise and MultimodalDocument12 pagesEffects of Physical Exercise in Older Adults With Reduced Physical Capacity Meta-Analysis of Resistance Exercise and MultimodalabcsouzaNo ratings yet
- Social Appearance Anxiety of Fitness ParticipantsDocument6 pagesSocial Appearance Anxiety of Fitness ParticipantsMumtaz MaulanaNo ratings yet
- Physical Self-Concept and Its Relationship To Exercise Dependence Symptoms in Young Regular Physical ExercisersDocument6 pagesPhysical Self-Concept and Its Relationship To Exercise Dependence Symptoms in Young Regular Physical ExercisersBarney MooreNo ratings yet
- Exploring The Gendered Nature of Weight Bias FIKKAN ROTHBLUMDocument18 pagesExploring The Gendered Nature of Weight Bias FIKKAN ROTHBLUMGonzalo PaezNo ratings yet
- UntitledDocument19 pagesUntitledAli NassarNo ratings yet
- Body Image: Emilio J. Compte, Ana R. Sepúlveda, Yolanda de Pellegrin, Miriam BlancoDocument7 pagesBody Image: Emilio J. Compte, Ana R. Sepúlveda, Yolanda de Pellegrin, Miriam BlancoameliaNo ratings yet
- Body Composition and Bone Mineral Density Of.1 PDFDocument6 pagesBody Composition and Bone Mineral Density Of.1 PDFJoao Evandro NetoNo ratings yet
- Factors Influencing Muscle Dysmorphia Among Individuals Within Gym CommunitiesDocument9 pagesFactors Influencing Muscle Dysmorphia Among Individuals Within Gym Communitiesangelpode93No ratings yet
- Wys Sen 2016Document7 pagesWys Sen 2016José RodríguezNo ratings yet
- College Men's Perceptions of Ideal Body Composition and ShapeDocument12 pagesCollege Men's Perceptions of Ideal Body Composition and ShapeJoyna HeinzNo ratings yet
- Associations Among Mens Sexist Attitudes Objectification of Women and Their Own Drive For MuscularityDocument11 pagesAssociations Among Mens Sexist Attitudes Objectification of Women and Their Own Drive For MuscularityFelipe Corrêa MessiasNo ratings yet
- The Body Image Psychological Inflexibility Scale DevelopmentDocument8 pagesThe Body Image Psychological Inflexibility Scale DevelopmentAna Gómez EstebanNo ratings yet
- Avila - 2010Document9 pagesAvila - 2010Matheus SilvaNo ratings yet
- Do You Even Lift BroDocument12 pagesDo You Even Lift BroCody MeyerNo ratings yet
- Weight Watchers She Loses, He Loses: The Truth about Men, Women, and Weight LossFrom EverandWeight Watchers She Loses, He Loses: The Truth about Men, Women, and Weight LossRating: 3 out of 5 stars3/5 (2)
- SR NFPA1583 v3Document8 pagesSR NFPA1583 v3nehemiasNo ratings yet
- Movement LibraryDocument72 pagesMovement LibraryKat ElvidgeNo ratings yet
- Bài tập bổ trợ anh 5 Smart Start Theme 1Document14 pagesBài tập bổ trợ anh 5 Smart Start Theme 1Phương ThảoNo ratings yet
- Screenshot 2024-01-13 at 14.51.57Document1 pageScreenshot 2024-01-13 at 14.51.57angelasaguirre573No ratings yet
- Estoy CansadoDocument100 pagesEstoy Cansadofujyreef100% (1)
- PE Narrative ReportDocument2 pagesPE Narrative ReportArjay L. PeñaNo ratings yet
- Cube PredatorDocument9 pagesCube PredatorDen KongNo ratings yet
- Muscular System NotesDocument6 pagesMuscular System NotesZussette Corbita VingcoNo ratings yet
- Adapted From The American Heart Association: Heart Rate Lab Lesson PlanDocument7 pagesAdapted From The American Heart Association: Heart Rate Lab Lesson PlansylNo ratings yet
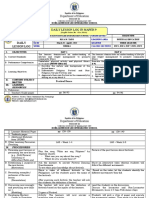
- DLL Q3 Week3 March28 Apr1Document5 pagesDLL Q3 Week3 March28 Apr1Rica TanoNo ratings yet
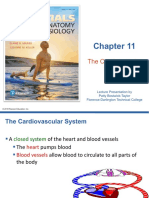
- Cu 10 Cardiovascular SystemDocument88 pagesCu 10 Cardiovascular SystemRose MendozaNo ratings yet
- Bio 20 Unit D Lesson 1 PresentationDocument16 pagesBio 20 Unit D Lesson 1 PresentationcoffinNo ratings yet
- W9-Module-Exercises To Boost Leg PowerDocument7 pagesW9-Module-Exercises To Boost Leg PowerBSBA MM-FMNo ratings yet
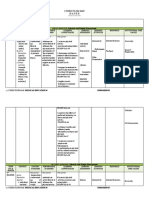
- Curriculum Map Mapeh: Lifestyle and Weight ManagementDocument7 pagesCurriculum Map Mapeh: Lifestyle and Weight ManagementJulie Ann Talento100% (1)
- Clauses of Purpose and ContrastDocument14 pagesClauses of Purpose and ContrastKlaudyna Strzępka-BrożekNo ratings yet
- Safe Lifting ManualDocument46 pagesSafe Lifting ManualvsfchanNo ratings yet
- Exercise Prescriptions For Health & FitnessDocument26 pagesExercise Prescriptions For Health & FitnessMuhammad wahabNo ratings yet
- Muscular SystemDocument22 pagesMuscular SystemFiraol DiribaNo ratings yet
- Artigo 01:09Document6 pagesArtigo 01:09Rodrigo AlvesNo ratings yet
- Tahun 6 Bahasa InggerisDocument14 pagesTahun 6 Bahasa InggerisRuss XanderNo ratings yet
- Assignment 9 RobertsDocument25 pagesAssignment 9 Robertsapi-550046687No ratings yet
- Team SportsDocument8 pagesTeam SportsNicoco LocoNo ratings yet
- Complete Sports Training - Speed, Strength & Conditioning For Today's Athlete PDFDocument221 pagesComplete Sports Training - Speed, Strength & Conditioning For Today's Athlete PDFognjenNo ratings yet
- Pe 103 Module First Semester 2020-2021Document49 pagesPe 103 Module First Semester 2020-2021John Gerard EstorbaNo ratings yet
- AB Flyer LRDocument2 pagesAB Flyer LRRidwan WanNo ratings yet
- Consider Four Basic Food GroupsDocument3 pagesConsider Four Basic Food GroupsPrecious ViterboNo ratings yet