Download as pdf or txt
You might also like
- Root Operations in The Medical and Surgical Section (ICD-10)Document2 pagesRoot Operations in The Medical and Surgical Section (ICD-10)Nicholas Henry100% (1)
- Anatomy and Physiology 1st Semester BSN General MCQS, Educational Platform-1Document9 pagesAnatomy and Physiology 1st Semester BSN General MCQS, Educational Platform-1Prince Masroor Ali Abro0% (1)
- Results With Continuous Cardiopulmonary Bypass For The Bidirectional Cavopulmonary Anastomosis - ProQuestDocument7 pagesResults With Continuous Cardiopulmonary Bypass For The Bidirectional Cavopulmonary Anastomosis - ProQuestWilliam WiryawanNo ratings yet
- 1 s2.0 S0929664608602041 MainDocument9 pages1 s2.0 S0929664608602041 MainEko SiswantoNo ratings yet
- Long-Term Outcomes of Patients With Tetralogy of Fallot Repaired in Young Infants and ToddlersDocument8 pagesLong-Term Outcomes of Patients With Tetralogy of Fallot Repaired in Young Infants and ToddlersResiden KardiologiNo ratings yet
- Asd FixDocument5 pagesAsd Fixratna putriNo ratings yet
- 1 s2.0 S187864802200444X MainDocument2 pages1 s2.0 S187864802200444X Mainade lydia br.siregarNo ratings yet
- PIIS091450871630020XDocument6 pagesPIIS091450871630020XGusti Ayu Radhitia OctaviaNo ratings yet
- Chandra 2013Document5 pagesChandra 2013Jose YoveraNo ratings yet
- Artificial Organs - 2009 - Popov - Mechanical Aortic Valve Replacement in Children and Adolescents After Previous Repair ofDocument7 pagesArtificial Organs - 2009 - Popov - Mechanical Aortic Valve Replacement in Children and Adolescents After Previous Repair ofWaleed Ismail KamelNo ratings yet
- Analysis of Post Operative Systemic To Pulmonary Artery Shunt FailureDocument5 pagesAnalysis of Post Operative Systemic To Pulmonary Artery Shunt FailurePaul HartingNo ratings yet
- 2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathyDocument9 pages2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathybanupluNo ratings yet
- Zheng 2016Document6 pagesZheng 2016Arindya RezekiNo ratings yet
- Study 3Document7 pagesStudy 3OstazNo ratings yet
- Article 7Document5 pagesArticle 7Kamal SaleemNo ratings yet
- Cardiac Interventions in Neonates WiDocument11 pagesCardiac Interventions in Neonates WiimNo ratings yet
- Aortic Valve Bypass: Experience From Denmark: Original Article - Adult CardiacDocument5 pagesAortic Valve Bypass: Experience From Denmark: Original Article - Adult CardiacmoplkiNo ratings yet
- Latus 2014Document5 pagesLatus 2014Effendi TanNo ratings yet
- 朱家权1Document9 pages朱家权1shentujin1997No ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open Reconstructiontmarrero00No ratings yet
- Follow-Up Transcatheter Closure of Atrial Septal Defect in Young Children: Results andDocument7 pagesFollow-Up Transcatheter Closure of Atrial Septal Defect in Young Children: Results andKholid KuNo ratings yet
- Korean QX Total Pulm Veins 2010Document5 pagesKorean QX Total Pulm Veins 2010Dr. LicónNo ratings yet
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDocument6 pagesPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNo ratings yet
- PIIS0003497519312469Document5 pagesPIIS0003497519312469Jacinto ThèauxNo ratings yet
- Progressive Right Ventricular Dysfunction in Patients With Pulmonary Arterial Hypertension Responding To TherapyDocument9 pagesProgressive Right Ventricular Dysfunction in Patients With Pulmonary Arterial Hypertension Responding To TherapyinaNo ratings yet
- 2011 Early Cannulation Grafts in Straight Axillo Axillary AngioaccessesDocument4 pages2011 Early Cannulation Grafts in Straight Axillo Axillary AngioaccessesKindylight KindylightNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofHesbon MomanyiNo ratings yet
- PIIS091450871930084XDocument7 pagesPIIS091450871930084XdrewantaNo ratings yet
- Aliment Pharmacol Ther - 2022 - Tergast - Home Based Tunnelled Peritoneal Drainage System As An Alternative TreatmentDocument11 pagesAliment Pharmacol Ther - 2022 - Tergast - Home Based Tunnelled Peritoneal Drainage System As An Alternative TreatmentTens AiepNo ratings yet
- The Impact of Dominant Ventricular Morphology On The Early Postoperative Course After The Glenn ProcedureDocument7 pagesThe Impact of Dominant Ventricular Morphology On The Early Postoperative Course After The Glenn ProcedureEitan KeizmanNo ratings yet
- Focus 1 Paper 4 Verheye Et Al 2015Document9 pagesFocus 1 Paper 4 Verheye Et Al 2015Jesson LuiNo ratings yet
- Abstracts / Pancreatology 19 (2019) S1 Es180 S30Document1 pageAbstracts / Pancreatology 19 (2019) S1 Es180 S30Hưng Nguyễn KiềuNo ratings yet
- AvenewDocument12 pagesAvenewNachchakorn DellNo ratings yet
- 1 PBDocument9 pages1 PBcorinaNo ratings yet
- Three-Dimensional Rotational Angiography As Guidance For Percutaneous Patent Ductus Arteriosus (PDA) Device Closure: A Case ReportDocument6 pagesThree-Dimensional Rotational Angiography As Guidance For Percutaneous Patent Ductus Arteriosus (PDA) Device Closure: A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Duplex Guided Balloon Angioplasty and Subintimal DDocument8 pagesDuplex Guided Balloon Angioplasty and Subintimal DJose PiulatsNo ratings yet
- Ekslusi The Importance of Preoperative Oxygen Saturation As A Predictor of Pulmonary Arterial Hypertension After Surgery of Atrial Septal DefectsDocument7 pagesEkslusi The Importance of Preoperative Oxygen Saturation As A Predictor of Pulmonary Arterial Hypertension After Surgery of Atrial Septal DefectsMaruliNo ratings yet
- Ejcm 11 0 enDocument388 pagesEjcm 11 0 enAlexander BerezinNo ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionRobert ChristevenNo ratings yet
- Kim2012Document5 pagesKim2012Stefanie MelisaNo ratings yet
- Concomitant Bentall Operation Plus Aortic Arch Replacement SurgeryDocument7 pagesConcomitant Bentall Operation Plus Aortic Arch Replacement Surgeryprofarmah6150No ratings yet
- Children: The Pulmonary Circulation in The Single Ventricle PatientDocument12 pagesChildren: The Pulmonary Circulation in The Single Ventricle PatientFernando PinedaNo ratings yet
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDocument9 pagesSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaNo ratings yet
- Intraaortic Balloon Pumping in ChildrenDocument6 pagesIntraaortic Balloon Pumping in ChildrenweikuohauNo ratings yet
- NEJM 2019 Early or Delayed Cardioversion in Recent-Onset Atrial FibrillationDocument10 pagesNEJM 2019 Early or Delayed Cardioversion in Recent-Onset Atrial Fibrillationsl duoNo ratings yet
- Nejmoa 2310392Document11 pagesNejmoa 2310392ENRIQUEFREDNo ratings yet
- Percutaneous Aortic Valve Implantation: The Anesthesiologist PerspectiveDocument11 pagesPercutaneous Aortic Valve Implantation: The Anesthesiologist Perspectiveserena7205No ratings yet
- NEJM 2 5 Mack Tavi1Document11 pagesNEJM 2 5 Mack Tavi1Mr. LNo ratings yet
- Laparoscopic Distal Splenoadrenal ShuntDocument5 pagesLaparoscopic Distal Splenoadrenal ShuntRichard QiuNo ratings yet
- Passive Leg Raising-Induced Changes in Pulse Pressure Variation To Assess Fluid Responsiveness in Mechanically Ventilated Patients - A Multicentre Prospective Observational StudyDocument9 pagesPassive Leg Raising-Induced Changes in Pulse Pressure Variation To Assess Fluid Responsiveness in Mechanically Ventilated Patients - A Multicentre Prospective Observational Studycardionerd101No ratings yet
- Acc 2021 00927Document9 pagesAcc 2021 00927DON TVNo ratings yet
- Influence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientsDocument6 pagesInfluence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientscamiladelgadomNo ratings yet
- Effect of The Preservation of Annulo-Papillary Continuity On Left Ventricular Ejection Fraction After Mitral Valve ReplacementDocument4 pagesEffect of The Preservation of Annulo-Papillary Continuity On Left Ventricular Ejection Fraction After Mitral Valve ReplacementThanh BinhNo ratings yet
- Khemani2009Document7 pagesKhemani2009Dwi Putri SekariniNo ratings yet
- Ecocardiografia Monitoreo Hemodinamico en Critico..Document12 pagesEcocardiografia Monitoreo Hemodinamico en Critico..cositaamorNo ratings yet
- Efficacy of Selective Arterial Embolisation For The Treatment of Life-Threatening Post-Partum Haemorrhage in A Large PopulationDocument6 pagesEfficacy of Selective Arterial Embolisation For The Treatment of Life-Threatening Post-Partum Haemorrhage in A Large PopulationAD MonikaNo ratings yet
- Case Report: Middle Aortic Syndrome Treated by Implantation of An Advanta V12 Large Diameter StentDocument3 pagesCase Report: Middle Aortic Syndrome Treated by Implantation of An Advanta V12 Large Diameter StentLenardR.ApazaNo ratings yet
- Baker 2013Document6 pagesBaker 2013Moni-k GuarnerosNo ratings yet
- 62 2020 Article 898Document7 pages62 2020 Article 898sinamirjaniNo ratings yet
- On-Treatment Function Testing of Platelets and Long-Term Outcome of Patients With Peripheral Arterial Disease Undergoing Transluminal AngioplastyDocument8 pagesOn-Treatment Function Testing of Platelets and Long-Term Outcome of Patients With Peripheral Arterial Disease Undergoing Transluminal AngioplastyGono GenieNo ratings yet
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- Best Practices of Apheresis in Hematopoietic Cell TransplantationFrom EverandBest Practices of Apheresis in Hematopoietic Cell TransplantationSyed A. AbutalibNo ratings yet
- Test Practice MBC DanishDocument3 pagesTest Practice MBC DanishdinaNo ratings yet
- MBC PracticeDocument2 pagesMBC PracticedinaNo ratings yet
- Approaches To Pulmonary Atresia With MAPCASDocument11 pagesApproaches To Pulmonary Atresia With MAPCASdinaNo ratings yet
- Persistent Pulmonary Hypertension of The NewbornDocument23 pagesPersistent Pulmonary Hypertension of The NewborndinaNo ratings yet
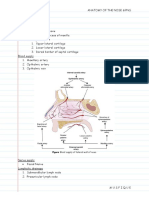
- Anatomy of The Nose & Paranasal Air SinusesDocument4 pagesAnatomy of The Nose & Paranasal Air SinusesMusfique RashidNo ratings yet
- Biomaterials Science, Ratner (2ed.) - 13-21Document9 pagesBiomaterials Science, Ratner (2ed.) - 13-21LUIS ANTHONY SALAS ARISTANo ratings yet
- Veterinary Internal Medicne - 2024 - Kendall - ACVIM Consensus Statement On Diagnosis and ManagementDocument26 pagesVeterinary Internal Medicne - 2024 - Kendall - ACVIM Consensus Statement On Diagnosis and Managementmarcia.lizolaNo ratings yet
- Pancreatic Cancer Handbook PDFDocument56 pagesPancreatic Cancer Handbook PDFsiti aisyahNo ratings yet
- ACDF WITHOUT IMPLANT (Orthopaedy)Document3 pagesACDF WITHOUT IMPLANT (Orthopaedy)mhjs ward6No ratings yet
- Da Vinci S System Docking Practicum PDFDocument6 pagesDa Vinci S System Docking Practicum PDFBio CientificNo ratings yet
- Spinal TuberculosisDocument54 pagesSpinal TuberculosisGagandeep YadavNo ratings yet
- Acute Respiratory FailureDocument5 pagesAcute Respiratory FailureHoney Bee S. PlatolonNo ratings yet
- RectumDocument129 pagesRectumRadhika SethuNo ratings yet
- Operating Room 2Document66 pagesOperating Room 2Ogy Ayop Mummy UddinNo ratings yet
- Northwest North Carolina Chapter: Register Online!! WWW - NWNCDocument8 pagesNorthwest North Carolina Chapter: Register Online!! WWW - NWNCJarrod WillardNo ratings yet
- Endoscopicretrograde Cholangiopancreatography (ERCP)Document21 pagesEndoscopicretrograde Cholangiopancreatography (ERCP)Suman PokhrelNo ratings yet
- Haad AnswersDocument106 pagesHaad AnswersMohammadKhanNo ratings yet
- Thorax and Lungs AnswersDocument3 pagesThorax and Lungs AnswersHazel Anne Dela CruzNo ratings yet
- Dextrocardia With Situs Inversus in An Adult Turkish 5797Document3 pagesDextrocardia With Situs Inversus in An Adult Turkish 5797Nazura Mohd NasirNo ratings yet
- Reviewer 418Document15 pagesReviewer 418Denese JocsonNo ratings yet
- Pathophysiology of Acute PainDocument12 pagesPathophysiology of Acute PainMuhammad Ghilman NurizzanNo ratings yet
- CholesistectomyDocument3 pagesCholesistectomyDenjo BonillaNo ratings yet
- Ico Guidelines For Diabetic Eye CareDocument19 pagesIco Guidelines For Diabetic Eye CareMuhammad Usman Salim100% (1)
- Thoracic Outlet SyndromeDocument16 pagesThoracic Outlet SyndromeDeepak RajNo ratings yet
- Spinal Cord TumoursDocument15 pagesSpinal Cord TumoursSakshi NegiNo ratings yet
- ACCP Lung Cancer 2013Document25 pagesACCP Lung Cancer 2013Hendarsyah SuryadinataNo ratings yet
- Blue Red LesionDocument14 pagesBlue Red LesionXara Barretto MagadiaNo ratings yet
- SBAR ToolDocument2 pagesSBAR Toolpragya_devkota0% (1)
- Definitive Orthodontic Treatmen1Document2 pagesDefinitive Orthodontic Treatmen1Dr.Fadi86% (7)
- Ebook Morreys The Elbow and Its Disorders PDF Full Chapter PDFDocument67 pagesEbook Morreys The Elbow and Its Disorders PDF Full Chapter PDFgeorge.messano625100% (34)
- ACL InjuryDocument42 pagesACL InjuryRishabh VermaNo ratings yet
- Thoracostomy Tubes and Catheters: Indications and Tube Selection in Adults and ChildrenDocument20 pagesThoracostomy Tubes and Catheters: Indications and Tube Selection in Adults and ChildrenaraNo ratings yet