Download as pdf or txt
You might also like
- Stahl's Essential Psychopharmacology - 5th EdDocument826 pagesStahl's Essential Psychopharmacology - 5th Edjulian.motjeeNo ratings yet
- UNHCR - Strengthening Mental Health and Psychosocial Support in 2021Document22 pagesUNHCR - Strengthening Mental Health and Psychosocial Support in 2021Beatriz SouzaNo ratings yet
- Sir Von Post ExamDocument21 pagesSir Von Post ExamxxxVINCHxxx0% (1)
- SA Mind Sep Oct 2015 PDFDocument70 pagesSA Mind Sep Oct 2015 PDFMichael CervantesNo ratings yet
- Seminar On Current Issues and Trends in Psychiatry. Mental Health Services in Kerala India and GlobalDocument34 pagesSeminar On Current Issues and Trends in Psychiatry. Mental Health Services in Kerala India and GlobalGopika SNo ratings yet
- 03 - 01 - 22 - WHO - Syria - Advocacy - Package - Fact Sheets - Mental Health - D3a2 - NoelDocument2 pages03 - 01 - 22 - WHO - Syria - Advocacy - Package - Fact Sheets - Mental Health - D3a2 - NoelLoloNo ratings yet
- 4.psyche Last TopicDocument84 pages4.psyche Last TopicJoseph Christian EstrellaNo ratings yet
- Mental Health First Aid Training: (MHFA)Document5 pagesMental Health First Aid Training: (MHFA)Biro Psikologi SakinahNo ratings yet
- Mental Health and OT Reference GuideDocument5 pagesMental Health and OT Reference GuideMaya JohnsonNo ratings yet
- Who Qualityrights: Act, Unite and EmpowerDocument4 pagesWho Qualityrights: Act, Unite and EmpowerRizki AmaliaNo ratings yet
- Mental Health ProgramsDocument25 pagesMental Health ProgramsJustine RaniliNo ratings yet
- Introduction To Mental Health Care in Indonesia: Herni SusantiDocument20 pagesIntroduction To Mental Health Care in Indonesia: Herni Susantiderry11082000No ratings yet
- Munity Psychiatry - COPDocument16 pagesMunity Psychiatry - COPCarlos Luque GNo ratings yet
- Adopting Mindfulness and Technology For Personalised Mental Health InterventionDocument2 pagesAdopting Mindfulness and Technology For Personalised Mental Health InterventionSeethe58No ratings yet
- Compiled PPT - CompressedDocument56 pagesCompiled PPT - CompressedAnchal SinghNo ratings yet
- Diploma in NursingDocument10 pagesDiploma in NursinglilianNo ratings yet
- Unit 1 CHN ConceptsDocument10 pagesUnit 1 CHN ConceptsJacqueline S. PunoNo ratings yet
- Psyche BoostDocument1 pagePsyche Boostmahrrby5No ratings yet
- College of Nursing: Cavite State UniversityDocument5 pagesCollege of Nursing: Cavite State UniversityIvy CalladaNo ratings yet
- Unit 2 - Psychology's Role in Primary CareDocument30 pagesUnit 2 - Psychology's Role in Primary CareGabrielaMichelle7No ratings yet
- Linking Mental Health NCDs HLM3 Priorities 2018Document10 pagesLinking Mental Health NCDs HLM3 Priorities 2018dkumar_100No ratings yet
- Consolidated 4Document12 pagesConsolidated 4marketing.nexonenterprisesNo ratings yet
- 4.psyche Last TopicDocument84 pages4.psyche Last TopicJoseph Christian EstrellaNo ratings yet
- Mental Health Awareness: The Indian Scenario: Industrial Psychiatry Journal July 2016Document5 pagesMental Health Awareness: The Indian Scenario: Industrial Psychiatry Journal July 2016Mirgank TirkhaNo ratings yet
- SARKHEL S, SINGH O P, ARORA M. Clinical Practice Guidelines For Psychoeducation in Psychiatric Disorders General Principles of PsychoeducationDocument5 pagesSARKHEL S, SINGH O P, ARORA M. Clinical Practice Guidelines For Psychoeducation in Psychiatric Disorders General Principles of PsychoeducationIsmael dos SantosNo ratings yet
- Cohesive, Collaborative, Collective: Advancing Mental Health Promotion in CanadaDocument60 pagesCohesive, Collaborative, Collective: Advancing Mental Health Promotion in CanadaPeterborough Examiner100% (2)
- Mental Health ProgramDocument4 pagesMental Health ProgramMADULI, Marlone G.100% (1)
- 53 Ijar2014julyDocument3 pages53 Ijar2014julySofia nazeerNo ratings yet
- Agency Overview PresentationDocument10 pagesAgency Overview Presentationapi-693321754No ratings yet
- 810 Presentation Poster - 2Document1 page810 Presentation Poster - 2Tayla Owen-JonesNo ratings yet
- Epidemiology and Psychiatric SciencesDocument5 pagesEpidemiology and Psychiatric SciencesExalted WahyoedieNo ratings yet
- Mental Health and Counselling PsychologyDocument8 pagesMental Health and Counselling PsychologyYahaya Ado WasaiNo ratings yet
- Mental Health Promotion in The Community: Nursing Perspectives' Mithun Kumar KurmiDocument7 pagesMental Health Promotion in The Community: Nursing Perspectives' Mithun Kumar KurmieditorbijnrNo ratings yet
- An Exploratory Study On The Feasibility and Appropriateness of Family Psychoeducation For Postpartum Women With Psychosis in UgandaDocument13 pagesAn Exploratory Study On The Feasibility and Appropriateness of Family Psychoeducation For Postpartum Women With Psychosis in UgandaEduardo Aguirre DávilaNo ratings yet
- MHN 10Document16 pagesMHN 10Vaishali SinghNo ratings yet
- HFN Annual Progress Report - Fy 2019Document26 pagesHFN Annual Progress Report - Fy 2019Shubha KandelNo ratings yet
- CHN 1Document10 pagesCHN 1keiemorayaNo ratings yet
- Community Mental HealthDocument17 pagesCommunity Mental HealthNicholeNo ratings yet
- A Psychotherapy Day Service For People With A Primary Diagnosis of Personality DisorderDocument1 pageA Psychotherapy Day Service For People With A Primary Diagnosis of Personality Disorderapi-75039177No ratings yet
- CMHA MHW Community Mental HealthDocument1 pageCMHA MHW Community Mental Healtharava.swapnaNo ratings yet
- Functions & Role of Community Mental Health Nursing: Srinivasan ADocument29 pagesFunctions & Role of Community Mental Health Nursing: Srinivasan AsrinivasanaNo ratings yet
- Challenges To Mental Health in The PhilsDocument40 pagesChallenges To Mental Health in The PhilsFrances Vale BasanNo ratings yet
- Nami ResourceDocument1 pageNami Resourceapi-578365819No ratings yet
- WAPHA AAD Handbook FAweb-pagesDocument6 pagesWAPHA AAD Handbook FAweb-pagesWilliam Lucero SalcedoNo ratings yet
- Mental Health - NIST Presentation - 2 Sept 2021.pptx - FINALDocument20 pagesMental Health - NIST Presentation - 2 Sept 2021.pptx - FINALnyagahvw86No ratings yet
- Using Digital Tech To Support Employees Mental Health and Resilience FDocument8 pagesUsing Digital Tech To Support Employees Mental Health and Resilience FElmer Orlando TampaNo ratings yet
- Program Officer - Mental HealthDocument3 pagesProgram Officer - Mental Healthhst7ngqth9No ratings yet
- Article 3Document12 pagesArticle 3Samuel Owusu DonkoNo ratings yet
- Your Journey Begins Here Your Journey Begins Here: March 20, 2010Document2 pagesYour Journey Begins Here Your Journey Begins Here: March 20, 2010api-26002115No ratings yet
- Portfolio Sijiya MamDocument1 pagePortfolio Sijiya Mammathewx01No ratings yet
- Mental Health AwarenessDocument1 pageMental Health AwarenessAtif SyedNo ratings yet
- Community Health Nursing 2 (Population Groups AND Community As ClientsDocument15 pagesCommunity Health Nursing 2 (Population Groups AND Community As ClientsJoann PunzalanNo ratings yet
- Mental Health and Counselling PsychologyDocument8 pagesMental Health and Counselling PsychologyYahaya Ado WasaiNo ratings yet
- BSN 3e Concept PaperDocument29 pagesBSN 3e Concept PaperCherish Marie HurbodaNo ratings yet
- Promotion and Prevention in Child Mental Health: Appropriate????Document8 pagesPromotion and Prevention in Child Mental Health: Appropriate????deepti sharmaNo ratings yet
- Psychiatric NursingDocument20 pagesPsychiatric Nursingjohn denver floresNo ratings yet
- AIOT occupational-therpy-intervention-in-COVID19 - FinalDocument19 pagesAIOT occupational-therpy-intervention-in-COVID19 - FinalAna Claudia GomesNo ratings yet
- Mindbloom 1Document10 pagesMindbloom 1Aryan BuchakeNo ratings yet
- The First Consumer Action Forum - Mental Health in Sri LankaDocument11 pagesThe First Consumer Action Forum - Mental Health in Sri LankaChintha Janaki MunasingheNo ratings yet
- A. Who: 1. Millennium Development Goals (MDGS)Document8 pagesA. Who: 1. Millennium Development Goals (MDGS)AmethystNo ratings yet
- The Positive Mental Health Instrument: Development and Validation of A Culturally Relevant Scale in A Multi-Ethnic Asian PopulationDocument19 pagesThe Positive Mental Health Instrument: Development and Validation of A Culturally Relevant Scale in A Multi-Ethnic Asian PopulationFebrio IglesiasNo ratings yet
- PICS-6pp-DL PRINTDocument2 pagesPICS-6pp-DL PRINTThuy LeNo ratings yet
- Psychiatric Mental Health Nursing Made Easy: Beginner's Guide to Mental Health NursingFrom EverandPsychiatric Mental Health Nursing Made Easy: Beginner's Guide to Mental Health NursingNo ratings yet
- Grnma NMCG Webinar Zoom 28th July 2023-1Document1 pageGrnma NMCG Webinar Zoom 28th July 2023-1Theophilus BaidooNo ratings yet
- Health Law and Ethics Lecture 01Document49 pagesHealth Law and Ethics Lecture 01Theophilus BaidooNo ratings yet
- Therapeutic Nurse-Client RelationshipDocument31 pagesTherapeutic Nurse-Client RelationshipTheophilus BaidooNo ratings yet
- The Hogbetsotso FestivalDocument3 pagesThe Hogbetsotso FestivalTheophilus BaidooNo ratings yet
- Practising As A Midwife in The UkDocument27 pagesPractising As A Midwife in The UkTheophilus BaidooNo ratings yet
- Press Release - Dubai AmbulanceDocument1 pagePress Release - Dubai AmbulanceTheophilus BaidooNo ratings yet
- Presentation On Mentoring For 37 Military Nurses Slide Share To GoDocument56 pagesPresentation On Mentoring For 37 Military Nurses Slide Share To GoTheophilus BaidooNo ratings yet
- Laryea's Care StudyDocument101 pagesLaryea's Care StudyTheophilus BaidooNo ratings yet
- Traffitech Brochure Update - 230818 - 123024Document1 pageTraffitech Brochure Update - 230818 - 123024Theophilus BaidooNo ratings yet
- Epidemiology 1Document60 pagesEpidemiology 1Theophilus BaidooNo ratings yet
- BIO130 Chapter 15&16 SlidesDocument26 pagesBIO130 Chapter 15&16 SlidesTheophilus BaidooNo ratings yet
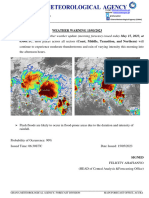
- Weather Warning 15052023Document1 pageWeather Warning 15052023Theophilus BaidooNo ratings yet
- Courses For Second Semester 2023 - 1Document6 pagesCourses For Second Semester 2023 - 1Theophilus BaidooNo ratings yet
- African Family and Health DeliveryDocument25 pagesAfrican Family and Health DeliveryTheophilus BaidooNo ratings yet
- Slave Trade and ColonialismDocument21 pagesSlave Trade and ColonialismTheophilus BaidooNo ratings yet
- BIO130 Chapter 17 SlidesDocument42 pagesBIO130 Chapter 17 SlidesTheophilus BaidooNo ratings yet
- Specialised Traditions of Knowledge and Health Delivery-1Document40 pagesSpecialised Traditions of Knowledge and Health Delivery-1Theophilus BaidooNo ratings yet
- Electron Transport System: ATP Adp + ATP Synthase P Nadh + H EnergyDocument12 pagesElectron Transport System: ATP Adp + ATP Synthase P Nadh + H EnergyTheophilus BaidooNo ratings yet
- African St. Political Systems LectureDocument23 pagesAfrican St. Political Systems LectureTheophilus BaidooNo ratings yet
- University of Health and Allied Sciences (UHAS) Ho Department of General and Liberal Studies UHAS 114: Introduction To Ghanaian and African StudiesDocument18 pagesUniversity of Health and Allied Sciences (UHAS) Ho Department of General and Liberal Studies UHAS 114: Introduction To Ghanaian and African StudiesTheophilus BaidooNo ratings yet
- African Belief Systems, Religion in Trad. Soc.Document42 pagesAfrican Belief Systems, Religion in Trad. Soc.Theophilus BaidooNo ratings yet
- Animation: Diffusion Through Cell MembranesDocument6 pagesAnimation: Diffusion Through Cell MembranesTheophilus BaidooNo ratings yet
- African Marriage Forms and Health Implica-TionsDocument43 pagesAfrican Marriage Forms and Health Implica-TionsTheophilus BaidooNo ratings yet
- Animation: Mitosis and CytokinesisDocument10 pagesAnimation: Mitosis and CytokinesisTheophilus BaidooNo ratings yet
- Chapt01 Holes Lecture Animation JWTDocument34 pagesChapt01 Holes Lecture Animation JWTCut TirayaNo ratings yet
- Regulation of Metabolic Pathways: Limited Number of Regulatory Enzymes Negative FeedbackDocument12 pagesRegulation of Metabolic Pathways: Limited Number of Regulatory Enzymes Negative FeedbackTheophilus BaidooNo ratings yet
- Animation: Primary Active TransportDocument12 pagesAnimation: Primary Active TransportTheophilus BaidooNo ratings yet
- Skeletal System: BY Victor BawiahDocument171 pagesSkeletal System: BY Victor BawiahTheophilus BaidooNo ratings yet
- Lymphatic System: By-Victor BawiahDocument42 pagesLymphatic System: By-Victor BawiahTheophilus BaidooNo ratings yet
- The Circulatory System CuDocument23 pagesThe Circulatory System CuTheophilus BaidooNo ratings yet
- Postreading Self Assessment and CME Test Preferred.28Document22 pagesPostreading Self Assessment and CME Test Preferred.28مجاهد إسماعيل حسن حسينNo ratings yet
- Bystritsky Anxiety Treatment Overview Pharm Therap 2013Document14 pagesBystritsky Anxiety Treatment Overview Pharm Therap 2013Amanuel MaruNo ratings yet
- Diagnosing in The Mood SpectrumDocument1 pageDiagnosing in The Mood Spectrumdo leeNo ratings yet
- Clinical Psychopharmacology of Eating Disorders: A Research UpdateDocument11 pagesClinical Psychopharmacology of Eating Disorders: A Research UpdategloriaNo ratings yet
- Kleinman - 1982 - Neurasthenia and Depression A Study of Somatization and Culture in ChinaDocument74 pagesKleinman - 1982 - Neurasthenia and Depression A Study of Somatization and Culture in ChinalessentomeNo ratings yet
- How To Conquer Social Anxiety For Document Sharing PDFDocument15 pagesHow To Conquer Social Anxiety For Document Sharing PDFAvery HaydenNo ratings yet
- Psych Drugs - From MedbulletsDocument2 pagesPsych Drugs - From MedbulletsFazeyfazeNo ratings yet
- Effectiveness of Vortioxetine in Patients With Major Depressive Disorder and Early-Stage Dementia - The MEMORY StudyDocument32 pagesEffectiveness of Vortioxetine in Patients With Major Depressive Disorder and Early-Stage Dementia - The MEMORY Studymalebranche18No ratings yet
- Low Back PainDocument17 pagesLow Back PainRamon Salinas AguileraNo ratings yet
- Evans Argumentative EssayDocument11 pagesEvans Argumentative Essayapi-451598862No ratings yet
- Kristin Layous, Et Al. Delivering Happiness. Translating Positive Psychology Intervention Research For Treating Major and Minor Depressive DisordersDocument11 pagesKristin Layous, Et Al. Delivering Happiness. Translating Positive Psychology Intervention Research For Treating Major and Minor Depressive DisordersCésar Daniel GonzálezNo ratings yet
- Psychiatric Nursing - Psycho PharmacologyDocument50 pagesPsychiatric Nursing - Psycho PharmacologyKaren MichelleNo ratings yet
- Antidepressant Discontinuation SyndromeDocument26 pagesAntidepressant Discontinuation SyndromeDevi DamayantiNo ratings yet
- Mood Disorders:: Identification and ManagementDocument45 pagesMood Disorders:: Identification and ManagementFikatu HugoronNo ratings yet
- Psychiatric MedicationsDocument1 pagePsychiatric MedicationspavanNo ratings yet
- Psychotropic Drugs: Western Mindanao State UniversityDocument41 pagesPsychotropic Drugs: Western Mindanao State UniversityAmie CuevasNo ratings yet
- Antidepressant AgentsDocument38 pagesAntidepressant AgentsdidiNo ratings yet
- Acupuncture Therapy: Mechanism of Action, Efficacy, and Safety: A Potential Intervention For Psychogenic Disorders?Document7 pagesAcupuncture Therapy: Mechanism of Action, Efficacy, and Safety: A Potential Intervention For Psychogenic Disorders?Nemanja ArsenovicNo ratings yet
- Nikolas Rose - Neurochemical Selves - Society, Nov/Dec 2003Document14 pagesNikolas Rose - Neurochemical Selves - Society, Nov/Dec 2003kod65redNo ratings yet
- PDF Libido CompressDocument16 pagesPDF Libido Compresskirollos adelNo ratings yet
- CG250 2012-05 Common Ground MagazineDocument40 pagesCG250 2012-05 Common Ground MagazineCommonGroundBCNo ratings yet
- Psy0418 EzineDocument33 pagesPsy0418 Ezinebulli babuNo ratings yet
- Neebs Fundamentals of Mental Health Nursing 4Th Edition Gorman Test Bank Full Chapter PDFDocument36 pagesNeebs Fundamentals of Mental Health Nursing 4Th Edition Gorman Test Bank Full Chapter PDFkatherinegarnerjwcrantdby100% (8)
- AdhdDocument92 pagesAdhdNeric Ico MagleoNo ratings yet
- Depression in Children and Adolescents: Evaluation and TreatmentDocument9 pagesDepression in Children and Adolescents: Evaluation and Treatmentmike jognNo ratings yet
- Frequently Asked Questions About PharmacogenomicsDocument7 pagesFrequently Asked Questions About PharmacogenomicsMaria Alvarez DejudNo ratings yet
- Depression Discussion PaperDocument14 pagesDepression Discussion Paperpinky giradoNo ratings yet