
1 - Sample - Porth's Essentials of Pathophysiology 5e 5th Edition
1 - Sample - Porth's Essentials of Pathophysiology 5e 5th Edition
You might also like
- NURS 681 Advanced Health Physical Assessment and Lab APRN 202207SUIIOL OL B 202207SUIIOL 2022Document22 pagesNURS 681 Advanced Health Physical Assessment and Lab APRN 202207SUIIOL OL B 202207SUIIOL 2022mamba.dedanNo ratings yet
- Professional Nursing Concepts CompetenciesDocument572 pagesProfessional Nursing Concepts CompetenciesM Ifadh Arifqy JNo ratings yet
- Communication in Nursing 10th EditionDocument120 pagesCommunication in Nursing 10th Editionmilkah mwauraNo ratings yet
- Primary Care Art and Science of Advanced Practice Nursing 3rd Edition Dunphy Test BankDocument2 pagesPrimary Care Art and Science of Advanced Practice Nursing 3rd Edition Dunphy Test BankClaytonMendezNo ratings yet
- TestBank Norris Porths Essentials Pathophysiology 5e 2019Document505 pagesTestBank Norris Porths Essentials Pathophysiology 5e 2019Cindy Perez50% (2)
- Test Bank Advanced Practice Nursing in The Care of Older Adults 2nd Edition Kennedy-MaloneDocument2 pagesTest Bank Advanced Practice Nursing in The Care of Older Adults 2nd Edition Kennedy-Malonegoogg33% (3)
- Advanced Practice Nursing of Adults in Acute Care - Foster, Janet G., Prevost, Suzanne S.Document789 pagesAdvanced Practice Nursing of Adults in Acute Care - Foster, Janet G., Prevost, Suzanne S.Rex Lagunzad Flores100% (12)
- Pathophysiology, Physical Assessment 2022Document523 pagesPathophysiology, Physical Assessment 2022Keith Mimis100% (6)
- Chapter 01: The History and Interviewing Process Ball: Seidel's Guide To Physical Examination, 9th EditionDocument198 pagesChapter 01: The History and Interviewing Process Ball: Seidel's Guide To Physical Examination, 9th EditionAbdellah Saad100% (4)
- Test Bank Advanced Practice Nursing Essential Knowledge For The Profession 4th Edition DeNiscoDocument3 pagesTest Bank Advanced Practice Nursing Essential Knowledge For The Profession 4th Edition DeNiscoFit ragner0% (1)
- Adult-Gerontology and Family Nurse PractitiCertification Examination - Dunphy, Lynne M., Winland-Brown, Jill EDocument577 pagesAdult-Gerontology and Family Nurse PractitiCertification Examination - Dunphy, Lynne M., Winland-Brown, Jill EJhoana Rose Joaquin Santos100% (22)
- IV Study Guide 2013Document78 pagesIV Study Guide 2013Kaloy KamaoNo ratings yet
- World Coins 2018Document42 pagesWorld Coins 2018Louis Horu63% (8)
- Middle Range TheoriesDocument370 pagesMiddle Range Theoriesvickyhouseqq.comNo ratings yet
- N5315 Advanced Pathophysiology Syllabus Fall 2014Document15 pagesN5315 Advanced Pathophysiology Syllabus Fall 2014meeeh100% (1)
- Edmunds & Mayhew Advanced Pharmacology Chapter 1 Test BankDocument2 pagesEdmunds & Mayhew Advanced Pharmacology Chapter 1 Test BankHunter HuntingtongNo ratings yet
- Research For Nurses - Methods and InterpretationDocument767 pagesResearch For Nurses - Methods and Interpretationawinsy100% (1)
- Basic Medical Language 6th Brooks Test BankDocument12 pagesBasic Medical Language 6th Brooks Test BankRamiqqNo ratings yet
- Professional Role Development Paper - Final 1Document7 pagesProfessional Role Development Paper - Final 1api-532705739No ratings yet
- Fabrication of Pneumatic Punching and Riveting MachineDocument45 pagesFabrication of Pneumatic Punching and Riveting MachineElakkiya Karthic100% (7)
- This Study Resource Was: G R A D E S L A B - C O MDocument8 pagesThis Study Resource Was: G R A D E S L A B - C O MHugsNo ratings yet
- Illustrated Pharmacology For NursesDocument481 pagesIllustrated Pharmacology For NursesFinanceiro CeestecNo ratings yet
- Test Bank For Essentials of Nursing Research Appraising Evidence For Nursing Practice Eighth 8th Edition Denise F PolitDocument7 pagesTest Bank For Essentials of Nursing Research Appraising Evidence For Nursing Practice Eighth 8th Edition Denise F Politdominiclovell6veqec0% (1)
- Chapter 43: Antiulcer Drugs Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th EditionDocument95 pagesChapter 43: Antiulcer Drugs Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th Editionmichael patterson100% (1)
- This Study Resource Was: Dlugasch - Ch02-Applied Pathophysiology For The Advanced Practice Nurse, 1eDocument4 pagesThis Study Resource Was: Dlugasch - Ch02-Applied Pathophysiology For The Advanced Practice Nurse, 1eHugs0% (1)
- NURSING THE CHILDBEARING FAMILY: Passbooks Study GuideFrom EverandNURSING THE CHILDBEARING FAMILY: Passbooks Study GuideNo ratings yet
- APN Adult Gerontology PresentationDocument57 pagesAPN Adult Gerontology PresentationMelissa Makhoul100% (1)
- Adult Gero ACNP CompetenciesDocument28 pagesAdult Gero ACNP CompetenciesCatalina KNo ratings yet
- Clinical Judgement-An Essential Tool in The Nursing Profession PDFDocument10 pagesClinical Judgement-An Essential Tool in The Nursing Profession PDFNers SenNo ratings yet
- Chapter 26: Antibacterials Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th EditionDocument16 pagesChapter 26: Antibacterials Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th Editionmichael pattersonNo ratings yet
- Adult Gero Prim Care NP CompDocument29 pagesAdult Gero Prim Care NP Compkdavis618100% (1)
- Avoiding Common Errors in The Emergency Department-1002-1280Document280 pagesAvoiding Common Errors in The Emergency Department-1002-1280Hernando CastrillónNo ratings yet
- Irene Comisso Et Al. Nursing in Critical Care Setting An Overview From Basic To Sensitive Outcomes 2018 SpringerDocument531 pagesIrene Comisso Et Al. Nursing in Critical Care Setting An Overview From Basic To Sensitive Outcomes 2018 SpringerFatima Medriza DuranNo ratings yet
- 6521 Advanced Pharmacology Final ExamDocument19 pages6521 Advanced Pharmacology Final ExamSandra JeffersonNo ratings yet
- Seidels P.E Chapter 2 Test BankDocument5 pagesSeidels P.E Chapter 2 Test BankAthena SaturdayNo ratings yet
- 63d0f228e52b8 Basic Geriatric Nursing 7th Edition Williams Test BankDocument108 pages63d0f228e52b8 Basic Geriatric Nursing 7th Edition Williams Test Bankerickomusiq7No ratings yet
- Chapter 13: Alterations in Oxygen Transport Banasik: Pathophysiology, 6th EditionDocument10 pagesChapter 13: Alterations in Oxygen Transport Banasik: Pathophysiology, 6th Editionqwivy.com100% (1)
- Essentials of Critical Care Nursing (gnv64) PDFDocument537 pagesEssentials of Critical Care Nursing (gnv64) PDFMohammad Tayyab KhanNo ratings yet
- History & Physical 8.17.10Document12 pagesHistory & Physical 8.17.10kman0722100% (1)
- Seidels P.E Chapter 5 Test BankDocument5 pagesSeidels P.E Chapter 5 Test BankAthena Saturday100% (1)
- Pathophysiology Applications BookshelfDocument35 pagesPathophysiology Applications Bookshelfmorgan bigelow100% (2)
- Critical Care SedationFrom EverandCritical Care SedationAngelo Raffaele De GaudioNo ratings yet
- Patho Exam QuestionsDocument3 pagesPatho Exam QuestionsAndin GangNo ratings yet
- FNP ResumeDocument2 pagesFNP Resumeapi-501795561No ratings yet
- FNP Midterm Exam 2018Document6 pagesFNP Midterm Exam 2018Jefferyi Knigth AlVarezNo ratings yet
- Notes On NursingWhat It Is, and What It Is Not by Nightingale, Florence, 1820-1920Document79 pagesNotes On NursingWhat It Is, and What It Is Not by Nightingale, Florence, 1820-1920Gutenberg.org100% (2)
- Medication Management - PaperDocument12 pagesMedication Management - PaperGinaNo ratings yet
- Patient Information: Upper Endoscopy: Consult The Medical Resource Doctors TrustDocument38 pagesPatient Information: Upper Endoscopy: Consult The Medical Resource Doctors TrustAjnesh PrasadNo ratings yet
- Clinical ExemplarDocument4 pagesClinical Exemplarapi-272451466No ratings yet
- NP CompetenciesDocument84 pagesNP CompetenciesarbyjamesNo ratings yet
- CEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsDocument18 pagesCEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsLauren GarciaNo ratings yet
- Advanced Practice Nursing: Setting a New Paradigm for Care in the 21St CenturyFrom EverandAdvanced Practice Nursing: Setting a New Paradigm for Care in the 21St CenturyNo ratings yet
- Hepatic EncephalopathyDocument251 pagesHepatic EncephalopathyDanteNo ratings yet
- Answer-A Rationale: Pityriasis Rosea Presents With Papulo-Squamous Lesions of 2 To 20 CM Diameter, inDocument15 pagesAnswer-A Rationale: Pityriasis Rosea Presents With Papulo-Squamous Lesions of 2 To 20 CM Diameter, inarunatejaNo ratings yet
- BNF For Children (BNFC) 2018-2019 (Year 2018-2019) : Advance Book InformationDocument1 pageBNF For Children (BNFC) 2018-2019 (Year 2018-2019) : Advance Book InformationKhaing Moh Moh ZinNo ratings yet
- American Nurses Credentialing Center (ANCC) Adult Nurse Practitioner Exam Study GuideDocument20 pagesAmerican Nurses Credentialing Center (ANCC) Adult Nurse Practitioner Exam Study GuideMcRee Learning CenterNo ratings yet
- 0323796303Document883 pages0323796303elmin_pctNo ratings yet
- Pathopysiology QuestionsDocument159 pagesPathopysiology QuestionsMaria EcaterinaNo ratings yet
- RD Scope of Nursing PracticeDocument26 pagesRD Scope of Nursing PracticeJurinia VicenteNo ratings yet
- Hal 1-50Document109 pagesHal 1-50Anonymous xh699eTd8I100% (2)
- NURS 6521N Final Exam Question and Answers Feb 2020 (100/100)Document19 pagesNURS 6521N Final Exam Question and Answers Feb 2020 (100/100)Judy Durkin0% (1)
- Explain FOUR Measures Which Governments Can Use To Encourage Entrepreneurial Activities in The Caribbean Region.Document2 pagesExplain FOUR Measures Which Governments Can Use To Encourage Entrepreneurial Activities in The Caribbean Region.Bridget SequeaNo ratings yet
- Check Manual: ES SeriesDocument42 pagesCheck Manual: ES SeriesArturo CalderonNo ratings yet
- MotoGP (TM) 13 - Boxed Version Patch LogDocument2 pagesMotoGP (TM) 13 - Boxed Version Patch LogAbdul Haris NabuNo ratings yet
- Certificate in Sports Facilities ManagementDocument7 pagesCertificate in Sports Facilities ManagementAnkush SinghNo ratings yet
- 4500MB - CH 2 - Parr - Stirred Reactors and Pressure Vessels Catalog v15 Literature PDFDocument45 pages4500MB - CH 2 - Parr - Stirred Reactors and Pressure Vessels Catalog v15 Literature PDFglaubersgNo ratings yet
- Sophos UTM Software Appliance: Quick Start GuideDocument7 pagesSophos UTM Software Appliance: Quick Start GuidearistidesNo ratings yet
- Emerging Trends in Sales ManagementDocument14 pagesEmerging Trends in Sales ManagementAbdul Quadir100% (7)
- Kindergarten Teacher Cover Letter SampleDocument6 pagesKindergarten Teacher Cover Letter Samplektrplormd100% (1)
- Lenovo t430 NZM4H-7 r7.54Document97 pagesLenovo t430 NZM4H-7 r7.54norberto100% (1)
- Sheldon Krimsky - Kathleen Sloan - Race and The Genetic Revolution - Science, Myth, and Culture-Columbia University Press (2011)Document300 pagesSheldon Krimsky - Kathleen Sloan - Race and The Genetic Revolution - Science, Myth, and Culture-Columbia University Press (2011)Burnley JenifferNo ratings yet
- By Sin I Rise Part Two Sins - Cora ReillyDocument237 pagesBy Sin I Rise Part Two Sins - Cora ReillyNour Al-khatib50% (2)
- Logitech Hidpp 2.0 Specification Draft 2012-06-04Document16 pagesLogitech Hidpp 2.0 Specification Draft 2012-06-04cpttrNo ratings yet
- IHITES - Volume 3 - Issue 4 - Pages 27-31Document6 pagesIHITES - Volume 3 - Issue 4 - Pages 27-31jonaNo ratings yet
- Dicky Ramadhan Fresh Graduate Information System: ProfileDocument2 pagesDicky Ramadhan Fresh Graduate Information System: ProfileNovia SuhendraeniNo ratings yet
- 03 - Lecture Slide - Basic Models in TensorFlowDocument94 pages03 - Lecture Slide - Basic Models in TensorFlowRoberto PereiraNo ratings yet
- Ashura in Morocco PDFDocument2 pagesAshura in Morocco PDFOmar BelazriNo ratings yet
- 1 CertDocument1 page1 CertWan Hakim Wan YaacobNo ratings yet
- CM1312 2320 1210 1510 2025rollerDocument2 pagesCM1312 2320 1210 1510 2025rollerAnonymous O6vHkdNo ratings yet
- Digestion Fill-In NotesDocument1 pageDigestion Fill-In Notesapi-296488161No ratings yet
- Scott Meech Etec 500 Journal AssignmentDocument7 pagesScott Meech Etec 500 Journal Assignmentapi-373684092No ratings yet
- DSP Question Bank With SolutionsDocument52 pagesDSP Question Bank With SolutionsRakesh Kumar DNo ratings yet
- Boomerang e A4Document7 pagesBoomerang e A4Djura RehNo ratings yet
- Felcom 15 Servi̇s ManualDocument236 pagesFelcom 15 Servi̇s ManualAnıl Kahya75% (8)
- Pega74 Install Tomcat Db2Document43 pagesPega74 Install Tomcat Db2Amit GujralNo ratings yet
- Ohio Department of Transportation: Highway Plan Reading ManualDocument68 pagesOhio Department of Transportation: Highway Plan Reading ManualMwesigwa Dani100% (1)
- Karthik ResumeDocument3 pagesKarthik Resumeshagy05No ratings yet
- CO2 Content in Brine Under Pressure 084Document11 pagesCO2 Content in Brine Under Pressure 084Mari ParguilNo ratings yet
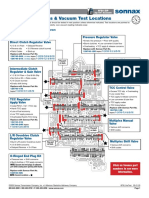
- Critical Wear Areas & Vacuum Test Locations: Upper Valve Body - 6F50 ShownDocument4 pagesCritical Wear Areas & Vacuum Test Locations: Upper Valve Body - 6F50 ShownautomaticosbrasilNo ratings yet























































































Download as pdf or txt
You might also like
- NURS 681 Advanced Health Physical Assessment and Lab APRN 202207SUIIOL OL B 202207SUIIOL 2022Document22 pagesNURS 681 Advanced Health Physical Assessment and Lab APRN 202207SUIIOL OL B 202207SUIIOL 2022mamba.dedanNo ratings yet
- Professional Nursing Concepts CompetenciesDocument572 pagesProfessional Nursing Concepts CompetenciesM Ifadh Arifqy JNo ratings yet
- Communication in Nursing 10th EditionDocument120 pagesCommunication in Nursing 10th Editionmilkah mwauraNo ratings yet
- Primary Care Art and Science of Advanced Practice Nursing 3rd Edition Dunphy Test BankDocument2 pagesPrimary Care Art and Science of Advanced Practice Nursing 3rd Edition Dunphy Test BankClaytonMendezNo ratings yet
- TestBank Norris Porths Essentials Pathophysiology 5e 2019Document505 pagesTestBank Norris Porths Essentials Pathophysiology 5e 2019Cindy Perez50% (2)
- Test Bank Advanced Practice Nursing in The Care of Older Adults 2nd Edition Kennedy-MaloneDocument2 pagesTest Bank Advanced Practice Nursing in The Care of Older Adults 2nd Edition Kennedy-Malonegoogg33% (3)
- Advanced Practice Nursing of Adults in Acute Care - Foster, Janet G., Prevost, Suzanne S.Document789 pagesAdvanced Practice Nursing of Adults in Acute Care - Foster, Janet G., Prevost, Suzanne S.Rex Lagunzad Flores100% (12)
- Pathophysiology, Physical Assessment 2022Document523 pagesPathophysiology, Physical Assessment 2022Keith Mimis100% (6)
- Chapter 01: The History and Interviewing Process Ball: Seidel's Guide To Physical Examination, 9th EditionDocument198 pagesChapter 01: The History and Interviewing Process Ball: Seidel's Guide To Physical Examination, 9th EditionAbdellah Saad100% (4)
- Test Bank Advanced Practice Nursing Essential Knowledge For The Profession 4th Edition DeNiscoDocument3 pagesTest Bank Advanced Practice Nursing Essential Knowledge For The Profession 4th Edition DeNiscoFit ragner0% (1)
- Adult-Gerontology and Family Nurse PractitiCertification Examination - Dunphy, Lynne M., Winland-Brown, Jill EDocument577 pagesAdult-Gerontology and Family Nurse PractitiCertification Examination - Dunphy, Lynne M., Winland-Brown, Jill EJhoana Rose Joaquin Santos100% (22)
- IV Study Guide 2013Document78 pagesIV Study Guide 2013Kaloy KamaoNo ratings yet
- World Coins 2018Document42 pagesWorld Coins 2018Louis Horu63% (8)
- Middle Range TheoriesDocument370 pagesMiddle Range Theoriesvickyhouseqq.comNo ratings yet
- N5315 Advanced Pathophysiology Syllabus Fall 2014Document15 pagesN5315 Advanced Pathophysiology Syllabus Fall 2014meeeh100% (1)
- Edmunds & Mayhew Advanced Pharmacology Chapter 1 Test BankDocument2 pagesEdmunds & Mayhew Advanced Pharmacology Chapter 1 Test BankHunter HuntingtongNo ratings yet
- Research For Nurses - Methods and InterpretationDocument767 pagesResearch For Nurses - Methods and Interpretationawinsy100% (1)
- Basic Medical Language 6th Brooks Test BankDocument12 pagesBasic Medical Language 6th Brooks Test BankRamiqqNo ratings yet
- Professional Role Development Paper - Final 1Document7 pagesProfessional Role Development Paper - Final 1api-532705739No ratings yet
- Fabrication of Pneumatic Punching and Riveting MachineDocument45 pagesFabrication of Pneumatic Punching and Riveting MachineElakkiya Karthic100% (7)
- This Study Resource Was: G R A D E S L A B - C O MDocument8 pagesThis Study Resource Was: G R A D E S L A B - C O MHugsNo ratings yet
- Illustrated Pharmacology For NursesDocument481 pagesIllustrated Pharmacology For NursesFinanceiro CeestecNo ratings yet
- Test Bank For Essentials of Nursing Research Appraising Evidence For Nursing Practice Eighth 8th Edition Denise F PolitDocument7 pagesTest Bank For Essentials of Nursing Research Appraising Evidence For Nursing Practice Eighth 8th Edition Denise F Politdominiclovell6veqec0% (1)
- Chapter 43: Antiulcer Drugs Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th EditionDocument95 pagesChapter 43: Antiulcer Drugs Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th Editionmichael patterson100% (1)
- This Study Resource Was: Dlugasch - Ch02-Applied Pathophysiology For The Advanced Practice Nurse, 1eDocument4 pagesThis Study Resource Was: Dlugasch - Ch02-Applied Pathophysiology For The Advanced Practice Nurse, 1eHugs0% (1)
- NURSING THE CHILDBEARING FAMILY: Passbooks Study GuideFrom EverandNURSING THE CHILDBEARING FAMILY: Passbooks Study GuideNo ratings yet
- APN Adult Gerontology PresentationDocument57 pagesAPN Adult Gerontology PresentationMelissa Makhoul100% (1)
- Adult Gero ACNP CompetenciesDocument28 pagesAdult Gero ACNP CompetenciesCatalina KNo ratings yet
- Clinical Judgement-An Essential Tool in The Nursing Profession PDFDocument10 pagesClinical Judgement-An Essential Tool in The Nursing Profession PDFNers SenNo ratings yet
- Chapter 26: Antibacterials Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th EditionDocument16 pagesChapter 26: Antibacterials Mccuistion: Pharmacology: A Patient-Centered Nursing Process Approach, 10Th Editionmichael pattersonNo ratings yet
- Adult Gero Prim Care NP CompDocument29 pagesAdult Gero Prim Care NP Compkdavis618100% (1)
- Avoiding Common Errors in The Emergency Department-1002-1280Document280 pagesAvoiding Common Errors in The Emergency Department-1002-1280Hernando CastrillónNo ratings yet
- Irene Comisso Et Al. Nursing in Critical Care Setting An Overview From Basic To Sensitive Outcomes 2018 SpringerDocument531 pagesIrene Comisso Et Al. Nursing in Critical Care Setting An Overview From Basic To Sensitive Outcomes 2018 SpringerFatima Medriza DuranNo ratings yet
- 6521 Advanced Pharmacology Final ExamDocument19 pages6521 Advanced Pharmacology Final ExamSandra JeffersonNo ratings yet
- Seidels P.E Chapter 2 Test BankDocument5 pagesSeidels P.E Chapter 2 Test BankAthena SaturdayNo ratings yet
- 63d0f228e52b8 Basic Geriatric Nursing 7th Edition Williams Test BankDocument108 pages63d0f228e52b8 Basic Geriatric Nursing 7th Edition Williams Test Bankerickomusiq7No ratings yet
- Chapter 13: Alterations in Oxygen Transport Banasik: Pathophysiology, 6th EditionDocument10 pagesChapter 13: Alterations in Oxygen Transport Banasik: Pathophysiology, 6th Editionqwivy.com100% (1)
- Essentials of Critical Care Nursing (gnv64) PDFDocument537 pagesEssentials of Critical Care Nursing (gnv64) PDFMohammad Tayyab KhanNo ratings yet
- History & Physical 8.17.10Document12 pagesHistory & Physical 8.17.10kman0722100% (1)
- Seidels P.E Chapter 5 Test BankDocument5 pagesSeidels P.E Chapter 5 Test BankAthena Saturday100% (1)
- Pathophysiology Applications BookshelfDocument35 pagesPathophysiology Applications Bookshelfmorgan bigelow100% (2)
- Critical Care SedationFrom EverandCritical Care SedationAngelo Raffaele De GaudioNo ratings yet
- Patho Exam QuestionsDocument3 pagesPatho Exam QuestionsAndin GangNo ratings yet
- FNP ResumeDocument2 pagesFNP Resumeapi-501795561No ratings yet
- FNP Midterm Exam 2018Document6 pagesFNP Midterm Exam 2018Jefferyi Knigth AlVarezNo ratings yet
- Notes On NursingWhat It Is, and What It Is Not by Nightingale, Florence, 1820-1920Document79 pagesNotes On NursingWhat It Is, and What It Is Not by Nightingale, Florence, 1820-1920Gutenberg.org100% (2)
- Medication Management - PaperDocument12 pagesMedication Management - PaperGinaNo ratings yet
- Patient Information: Upper Endoscopy: Consult The Medical Resource Doctors TrustDocument38 pagesPatient Information: Upper Endoscopy: Consult The Medical Resource Doctors TrustAjnesh PrasadNo ratings yet
- Clinical ExemplarDocument4 pagesClinical Exemplarapi-272451466No ratings yet
- NP CompetenciesDocument84 pagesNP CompetenciesarbyjamesNo ratings yet
- CEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsDocument18 pagesCEN Guide 4: Guide For The Inclusion of Environmental Aspects in Product StandardsLauren GarciaNo ratings yet
- Advanced Practice Nursing: Setting a New Paradigm for Care in the 21St CenturyFrom EverandAdvanced Practice Nursing: Setting a New Paradigm for Care in the 21St CenturyNo ratings yet
- Hepatic EncephalopathyDocument251 pagesHepatic EncephalopathyDanteNo ratings yet
- Answer-A Rationale: Pityriasis Rosea Presents With Papulo-Squamous Lesions of 2 To 20 CM Diameter, inDocument15 pagesAnswer-A Rationale: Pityriasis Rosea Presents With Papulo-Squamous Lesions of 2 To 20 CM Diameter, inarunatejaNo ratings yet
- BNF For Children (BNFC) 2018-2019 (Year 2018-2019) : Advance Book InformationDocument1 pageBNF For Children (BNFC) 2018-2019 (Year 2018-2019) : Advance Book InformationKhaing Moh Moh ZinNo ratings yet
- American Nurses Credentialing Center (ANCC) Adult Nurse Practitioner Exam Study GuideDocument20 pagesAmerican Nurses Credentialing Center (ANCC) Adult Nurse Practitioner Exam Study GuideMcRee Learning CenterNo ratings yet
- 0323796303Document883 pages0323796303elmin_pctNo ratings yet
- Pathopysiology QuestionsDocument159 pagesPathopysiology QuestionsMaria EcaterinaNo ratings yet
- RD Scope of Nursing PracticeDocument26 pagesRD Scope of Nursing PracticeJurinia VicenteNo ratings yet
- Hal 1-50Document109 pagesHal 1-50Anonymous xh699eTd8I100% (2)
- NURS 6521N Final Exam Question and Answers Feb 2020 (100/100)Document19 pagesNURS 6521N Final Exam Question and Answers Feb 2020 (100/100)Judy Durkin0% (1)
- Explain FOUR Measures Which Governments Can Use To Encourage Entrepreneurial Activities in The Caribbean Region.Document2 pagesExplain FOUR Measures Which Governments Can Use To Encourage Entrepreneurial Activities in The Caribbean Region.Bridget SequeaNo ratings yet
- Check Manual: ES SeriesDocument42 pagesCheck Manual: ES SeriesArturo CalderonNo ratings yet
- MotoGP (TM) 13 - Boxed Version Patch LogDocument2 pagesMotoGP (TM) 13 - Boxed Version Patch LogAbdul Haris NabuNo ratings yet
- Certificate in Sports Facilities ManagementDocument7 pagesCertificate in Sports Facilities ManagementAnkush SinghNo ratings yet
- 4500MB - CH 2 - Parr - Stirred Reactors and Pressure Vessels Catalog v15 Literature PDFDocument45 pages4500MB - CH 2 - Parr - Stirred Reactors and Pressure Vessels Catalog v15 Literature PDFglaubersgNo ratings yet
- Sophos UTM Software Appliance: Quick Start GuideDocument7 pagesSophos UTM Software Appliance: Quick Start GuidearistidesNo ratings yet
- Emerging Trends in Sales ManagementDocument14 pagesEmerging Trends in Sales ManagementAbdul Quadir100% (7)
- Kindergarten Teacher Cover Letter SampleDocument6 pagesKindergarten Teacher Cover Letter Samplektrplormd100% (1)
- Lenovo t430 NZM4H-7 r7.54Document97 pagesLenovo t430 NZM4H-7 r7.54norberto100% (1)
- Sheldon Krimsky - Kathleen Sloan - Race and The Genetic Revolution - Science, Myth, and Culture-Columbia University Press (2011)Document300 pagesSheldon Krimsky - Kathleen Sloan - Race and The Genetic Revolution - Science, Myth, and Culture-Columbia University Press (2011)Burnley JenifferNo ratings yet
- By Sin I Rise Part Two Sins - Cora ReillyDocument237 pagesBy Sin I Rise Part Two Sins - Cora ReillyNour Al-khatib50% (2)
- Logitech Hidpp 2.0 Specification Draft 2012-06-04Document16 pagesLogitech Hidpp 2.0 Specification Draft 2012-06-04cpttrNo ratings yet
- IHITES - Volume 3 - Issue 4 - Pages 27-31Document6 pagesIHITES - Volume 3 - Issue 4 - Pages 27-31jonaNo ratings yet
- Dicky Ramadhan Fresh Graduate Information System: ProfileDocument2 pagesDicky Ramadhan Fresh Graduate Information System: ProfileNovia SuhendraeniNo ratings yet
- 03 - Lecture Slide - Basic Models in TensorFlowDocument94 pages03 - Lecture Slide - Basic Models in TensorFlowRoberto PereiraNo ratings yet
- Ashura in Morocco PDFDocument2 pagesAshura in Morocco PDFOmar BelazriNo ratings yet
- 1 CertDocument1 page1 CertWan Hakim Wan YaacobNo ratings yet
- CM1312 2320 1210 1510 2025rollerDocument2 pagesCM1312 2320 1210 1510 2025rollerAnonymous O6vHkdNo ratings yet
- Digestion Fill-In NotesDocument1 pageDigestion Fill-In Notesapi-296488161No ratings yet
- Scott Meech Etec 500 Journal AssignmentDocument7 pagesScott Meech Etec 500 Journal Assignmentapi-373684092No ratings yet
- DSP Question Bank With SolutionsDocument52 pagesDSP Question Bank With SolutionsRakesh Kumar DNo ratings yet
- Boomerang e A4Document7 pagesBoomerang e A4Djura RehNo ratings yet
- Felcom 15 Servi̇s ManualDocument236 pagesFelcom 15 Servi̇s ManualAnıl Kahya75% (8)
- Pega74 Install Tomcat Db2Document43 pagesPega74 Install Tomcat Db2Amit GujralNo ratings yet
- Ohio Department of Transportation: Highway Plan Reading ManualDocument68 pagesOhio Department of Transportation: Highway Plan Reading ManualMwesigwa Dani100% (1)
- Karthik ResumeDocument3 pagesKarthik Resumeshagy05No ratings yet
- CO2 Content in Brine Under Pressure 084Document11 pagesCO2 Content in Brine Under Pressure 084Mari ParguilNo ratings yet
- Critical Wear Areas & Vacuum Test Locations: Upper Valve Body - 6F50 ShownDocument4 pagesCritical Wear Areas & Vacuum Test Locations: Upper Valve Body - 6F50 ShownautomaticosbrasilNo ratings yet