Download as xlsx, pdf, or txt
You might also like
- Expectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameDocument3 pagesExpectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameLeslie D. Aton87% (15)
- Expectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameDocument3 pagesExpectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameLeslie D. Aton60% (5)
- Expectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameDocument3 pagesExpectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameLeslie D. Aton80% (10)
- Record of Barangay Inhabitants by Household: Date AccomplishedDocument3 pagesRecord of Barangay Inhabitants by Household: Date Accomplishedrandy hernandez100% (3)
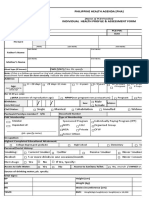
- PHA Individual Health Profile & Assessment Form As of Oct.09, 2017Document8 pagesPHA Individual Health Profile & Assessment Form As of Oct.09, 2017Eden VblagasyNo ratings yet
- Feeding ProgramDocument1 pageFeeding ProgramPau ZaballeroNo ratings yet
- PersonalityDocument2 pagesPersonalityMohamed AmzatNo ratings yet
- Postnatal Care: General InformationDocument7 pagesPostnatal Care: General InformationSri Abinash MishraNo ratings yet
- 1 Health History Woman PDFDocument3 pages1 Health History Woman PDFAhlem LahidhebNo ratings yet
- OPT Plus Form 1 List of Preschoolers With Height Measurement and Identified Nutritional StatusDocument10 pagesOPT Plus Form 1 List of Preschoolers With Height Measurement and Identified Nutritional StatusNorhanifa HADJI AMERNo ratings yet
- PSM Case ProformaDocument28 pagesPSM Case ProformaSathish100% (1)
- Medical FormDocument2 pagesMedical FormAnnnisa100% (1)
- Nfhs Student Health RecordDocument2 pagesNfhs Student Health Recordestudillojesusimo64No ratings yet
- Form KonselingDocument2 pagesForm KonselingUmi LatifahNo ratings yet
- Practical Record Book of MHN For B SC Nursing 03-06-2024Document152 pagesPractical Record Book of MHN For B SC Nursing 03-06-2024rakeshghonasagiNo ratings yet
- Pangasinan NNC File TemplateDocument1 pagePangasinan NNC File TemplateMark Raven PoyaoanNo ratings yet
- Bloodtypes, Bodytypes, and You: Why Your Unique Genetic Code is the Key to Losing Weight for LifeFrom EverandBloodtypes, Bodytypes, and You: Why Your Unique Genetic Code is the Key to Losing Weight for LifeRating: 5 out of 5 stars5/5 (1)
- Nursing Department: Bicol University Tabaco Campus Tabaco CityDocument3 pagesNursing Department: Bicol University Tabaco Campus Tabaco CityCelline Isabelle ReyesNo ratings yet
- Normal Pedia Assessment Guide Sep2023Document4 pagesNormal Pedia Assessment Guide Sep2023krishamarie.roldanNo ratings yet
- Gran Logia Nacional de Filipinas: Member Information SheetDocument1 pageGran Logia Nacional de Filipinas: Member Information SheetDen-Mark MedelNo ratings yet
- FBHP Congregational Care Survey Draft Updated 2 - 2 - 2021Document4 pagesFBHP Congregational Care Survey Draft Updated 2 - 2 - 2021Isaiah Knight Student - HeritageHSNo ratings yet
- Askeb Persalinan 2Document16 pagesAskeb Persalinan 2Anggreni APNo ratings yet
- Childs Growth DevelopmentDocument51 pagesChilds Growth Developmentmd191031No ratings yet
- College Application Form: ID PictureDocument3 pagesCollege Application Form: ID PictureDionne Sebastian DoromalNo ratings yet
- Job Application Form Oct 2018Document3 pagesJob Application Form Oct 2018ahmerNo ratings yet
- Postnatalassessment 190419153322Document3 pagesPostnatalassessment 190419153322megha30kashyap09No ratings yet
- Background Information A. Child C. HealthDocument1 pageBackground Information A. Child C. HealthMay annNo ratings yet
- Family Surveyed 2017 - TimberDocument26 pagesFamily Surveyed 2017 - TimberAlibasher Macalnas0% (1)
- Health Booklet 2014Document68 pagesHealth Booklet 2014Tan KMNo ratings yet
- Discipleship Profile: Personal DataDocument2 pagesDiscipleship Profile: Personal DataAlona Villamor ChancoNo ratings yet
- Central Philippine University College of Medicine: "Daw Naggulpi Kupos Lawas Niya"Document2 pagesCentral Philippine University College of Medicine: "Daw Naggulpi Kupos Lawas Niya"anon_858662383No ratings yet
- Postpartum AssessmentDocument2 pagesPostpartum AssessmentmichinagatomoNo ratings yet
- Askeb Persalinan 1Document14 pagesAskeb Persalinan 1Anggreni APNo ratings yet
- Health Booklet 2014Document68 pagesHealth Booklet 2014QwesxzNo ratings yet
- Mother-Child BookDocument40 pagesMother-Child BookTherese Mae MadroneroNo ratings yet
- Student Permanent Health Record-40Document1 pageStudent Permanent Health Record-40eroshNo ratings yet
- Completed Exemplar 9Document20 pagesCompleted Exemplar 9api-374818694No ratings yet
- Lecture 7-Adolescence 10.28 Full SlidesDocument110 pagesLecture 7-Adolescence 10.28 Full SlidesShannonNo ratings yet
- Cursillo Candidate Application FormDocument1 pageCursillo Candidate Application FormThe Filipino Cursillo Community Diocese of OaklandNo ratings yet
- Nifas 4Document9 pagesNifas 4gek ayuNo ratings yet
- Antenatal CareDocument7 pagesAntenatal Careunnatiswaraj7No ratings yet
- Youth Camp Registration Form and Waiver - 2023Document1 pageYouth Camp Registration Form and Waiver - 2023Ernesto GrijaldoNo ratings yet
- Service Volunteer Application Kimberton HillsDocument6 pagesService Volunteer Application Kimberton HillsNelsonNo ratings yet
- Michigan: 2018 County Health Rankings ReportDocument16 pagesMichigan: 2018 County Health Rankings ReportClickon DetroitNo ratings yet
- Weekly JournalDocument4 pagesWeekly Journalmaritesjasmin68No ratings yet
- Nutritional Assessments For Pediatric PDFDocument90 pagesNutritional Assessments For Pediatric PDFPatyNo ratings yet
- Pragyan College of Nursing, Bhopal: Community Care Plan/ Case Study / Care Presentation Format/ PerformaDocument6 pagesPragyan College of Nursing, Bhopal: Community Care Plan/ Case Study / Care Presentation Format/ PerformaNeelofur Ibran AliNo ratings yet
- Nurse HistoryDocument3 pagesNurse HistoryHAROLD ANGELESNo ratings yet
- Formulario EncryptedDocument2 pagesFormulario EncryptedRuben GonzalezNo ratings yet
- South Carolina: 2018 County Health Rankings ReportDocument16 pagesSouth Carolina: 2018 County Health Rankings ReportGreenville NewsNo ratings yet
- Family Care Study c5Document33 pagesFamily Care Study c5Kylie Golindang100% (1)
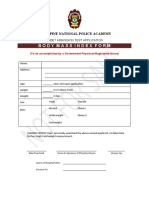
- PNPACAT BMI FormDocument1 pagePNPACAT BMI FormSamuel NaponeNo ratings yet
- Simplified PEKA B40 FOR PP SCREENSHOT CAN DELETEDocument1 pageSimplified PEKA B40 FOR PP SCREENSHOT CAN DELETEKKUTC PerlisNo ratings yet
- Care Plan MATERNITYDocument7 pagesCare Plan MATERNITYjeezawi91No ratings yet
- WCM Medical FormDocument4 pagesWCM Medical Formjewel_meltonNo ratings yet
- Child Intake FormDocument12 pagesChild Intake FormNadia AhmedNo ratings yet
- Republic of The Philippines 2Document2 pagesRepublic of The Philippines 2mike g.quimnoNo ratings yet
- Pediatric Nursing Process: I. Biographical InformationDocument11 pagesPediatric Nursing Process: I. Biographical InformationChin Michael AngNo ratings yet
- Expectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameDocument3 pagesExpectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameLeslie D. AtonNo ratings yet
- Geria Mrs. AcobDocument11 pagesGeria Mrs. Acob2C1 - YABES, JenniferNo ratings yet
- Strengthening The Filipino FamilyDocument39 pagesStrengthening The Filipino FamilyANNE THERESE GRAVINONo ratings yet
- BDC ResolutionDocument2 pagesBDC Resolutionrandy hernandezNo ratings yet
- Annual Accomplishment Report-TableDocument2 pagesAnnual Accomplishment Report-Tablerandy hernandezNo ratings yet
- Accomplishment Form of BarangayDocument2 pagesAccomplishment Form of Barangayrandy hernandezNo ratings yet
- Annex B PPAN Accomplishment Report Template BarangayDocument2 pagesAnnex B PPAN Accomplishment Report Template Barangayrandy hernandez100% (1)
- Resolution Approving The BDRRMP 2018-2022 - Talaba IIIDocument1 pageResolution Approving The BDRRMP 2018-2022 - Talaba IIIrandy hernandezNo ratings yet
- BADAC Monitoring Form 1000Document1 pageBADAC Monitoring Form 1000randy hernandezNo ratings yet
- Request SeniorDocument2 pagesRequest Seniorrandy hernandezNo ratings yet
- Authorization LetterDocument1 pageAuthorization Letterrandy hernandezNo ratings yet
- Bacoor Pet Medical MissionDocument1 pageBacoor Pet Medical Missionrandy hernandezNo ratings yet
- Republic of The Philippines Province of Cavite City of Bacoor Barangay Talaba IIIDocument4 pagesRepublic of The Philippines Province of Cavite City of Bacoor Barangay Talaba IIIrandy hernandez100% (1)
- MI VisionDocument2 pagesMI Visionrandy hernandezNo ratings yet
- Vaccine CIER Form For SeniorDocument1 pageVaccine CIER Form For Seniorrandy hernandezNo ratings yet
- VAW Desk Form 5Document2 pagesVAW Desk Form 5randy hernandezNo ratings yet
- Republic of The Philippines Province of Cavite City of Bacoor Barangay Talaba IiiDocument2 pagesRepublic of The Philippines Province of Cavite City of Bacoor Barangay Talaba Iiirandy hernandez100% (4)
- Department of The Interior and Local GovernmentDocument19 pagesDepartment of The Interior and Local Governmentrandy hernandez100% (2)
- Weekly Clean Up Drive Form DENRDocument1 pageWeekly Clean Up Drive Form DENRrandy hernandezNo ratings yet
- Bpops Plan FormDocument12 pagesBpops Plan Formrandy hernandez83% (6)
- BARANGAY - : Office of The Punong BarangayDocument1 pageBARANGAY - : Office of The Punong Barangayrandy hernandezNo ratings yet