
Chin Dermatitis in A Cat 8656 Article
Chin Dermatitis in A Cat 8656 Article
You might also like
- July 23, 2009 Through August 24, 2009 JPMorgan Chase BankDocument4 pagesJuly 23, 2009 Through August 24, 2009 JPMorgan Chase BankMaria Blackburn33% (3)
- Multi Choice Tech 1 AnswerDocument20 pagesMulti Choice Tech 1 AnswerquyennqNo ratings yet
- Test Report Form: Candidate DetailsDocument1 pageTest Report Form: Candidate DetailsPranav BabbarNo ratings yet
- Adventure Travel Sample Marketing PlanDocument26 pagesAdventure Travel Sample Marketing PlanPalo Alto Software100% (9)
- Dispersive Characteristics of Clay Soil by Double HydrometerDocument3 pagesDispersive Characteristics of Clay Soil by Double Hydrometerโก อู๋No ratings yet
- Linear Organoid Nevus in A Dog (Pages 69-73)Document5 pagesLinear Organoid Nevus in A Dog (Pages 69-73)jenNo ratings yet
- Jurnal RSMH Palembang: Black Dot Type Capitis Tinea Appreciates Bacterial FoliculitisDocument5 pagesJurnal RSMH Palembang: Black Dot Type Capitis Tinea Appreciates Bacterial FoliculitisLailatuz ZakiyahNo ratings yet
- Lecture 4 - Bacterial Skin DiseasesDocument13 pagesLecture 4 - Bacterial Skin DiseasesticoypiperNo ratings yet
- PV0412 Mueller ADDocument4 pagesPV0412 Mueller ADtahlokoNo ratings yet
- Trichoscopic Diagnosis of Cutaneous Pelodera Strongyloides Infestation in A DogDocument5 pagesTrichoscopic Diagnosis of Cutaneous Pelodera Strongyloides Infestation in A DogRebeka MenezesNo ratings yet
- TVP 2018 0102 Banovic Canine Atopic Dermatitis 11Document18 pagesTVP 2018 0102 Banovic Canine Atopic Dermatitis 11Kimchi LynnNo ratings yet
- ElízabethDocument12 pagesElízabethJahir QHNo ratings yet
- Shell Rot Infection in Red Eared Turtle: August 2017Document3 pagesShell Rot Infection in Red Eared Turtle: August 2017dwi putriNo ratings yet
- UP Devon Rex Vet DermDocument7 pagesUP Devon Rex Vet Dermandrostona980No ratings yet
- An Idiopathic Facial Dermatitis of Persian CatsDocument7 pagesAn Idiopathic Facial Dermatitis of Persian CatsjenNo ratings yet
- Sterile Eosinophilic Pustule, Canine Subcorneal Pustular Dermatitis, Feline Hypereosinophilic Syndrome, Idiopathic Sterile GranulomaDocument15 pagesSterile Eosinophilic Pustule, Canine Subcorneal Pustular Dermatitis, Feline Hypereosinophilic Syndrome, Idiopathic Sterile GranulomaBiancaNo ratings yet
- Management of Corneal Ulcer PDFDocument2 pagesManagement of Corneal Ulcer PDFYosiita KartinaaNo ratings yet
- 1 s2.0 S2211753918301441 MainDocument4 pages1 s2.0 S2211753918301441 MainMateoNo ratings yet
- Gigitan SeranggaaDocument10 pagesGigitan Seranggaaashahs andjadgiNo ratings yet
- Scedosporium Apiospermum Keratomycosis in A DogDocument4 pagesScedosporium Apiospermum Keratomycosis in A DogDavid Argüelles AndradeNo ratings yet
- Capsules: (The in Brief)Document1 pageCapsules: (The in Brief)JeevaNo ratings yet
- Darier-White Disease: A Rare Genetic DisorderDocument4 pagesDarier-White Disease: A Rare Genetic Disorderanis utamiNo ratings yet
- NJKKMDocument4 pagesNJKKMAyu MabariaNo ratings yet
- Pyoderma DogsDocument7 pagesPyoderma DogstorqtechNo ratings yet
- Chronic Generalized Dermatophilosis in A BuffaloDocument3 pagesChronic Generalized Dermatophilosis in A BuffaloHendroNo ratings yet
- Ciclosporin Therapy For Canine Generalized Discoid LupusDocument6 pagesCiclosporin Therapy For Canine Generalized Discoid LupusPatrícia StancuNo ratings yet
- Mucinosis Por Un FarmadoDocument4 pagesMucinosis Por Un FarmadoLuluu CortésNo ratings yet
- Keratolyse Ponctuee Foot 1870519Document1 pageKeratolyse Ponctuee Foot 1870519redhaNo ratings yet
- Clinicalcytology 4 1125Document5 pagesClinicalcytology 4 1125Paula TorcheNo ratings yet
- BiodataDocument11 pagesBiodatabentubz100% (2)
- Inflammatory Tinea Capitis. A Clinical Case Presentation Treated With Oral TerbinafineDocument2 pagesInflammatory Tinea Capitis. A Clinical Case Presentation Treated With Oral TerbinafineSuci Triana PutriNo ratings yet
- Surface Infections 1st & 3rd Sept-2022Document7 pagesSurface Infections 1st & 3rd Sept-2022Doctor iVJNo ratings yet
- Tinea Versicolor of The Neck As Side Effect of Topical Steroids For Alopecia AreataDocument12 pagesTinea Versicolor of The Neck As Side Effect of Topical Steroids For Alopecia AreataNazihan Safitri AlkatiriNo ratings yet
- Progressive Langerhans' Cell Histiocytosis in A Puppy (Pages 241-246)Document6 pagesProgressive Langerhans' Cell Histiocytosis in A Puppy (Pages 241-246)jenNo ratings yet
- Acrodermatitis EnteropathicaDocument4 pagesAcrodermatitis EnteropathicaIntan FajrinNo ratings yet
- Case Report Tinea Corporis: By: Nurul Ayni Supervisor: Irma Tarida L, Dr. SP - KKDocument22 pagesCase Report Tinea Corporis: By: Nurul Ayni Supervisor: Irma Tarida L, Dr. SP - KKnurulayniNo ratings yet
- Lichen Amyloidosis With Combined Topical Therapy: A Case ReportDocument3 pagesLichen Amyloidosis With Combined Topical Therapy: A Case ReportmutmainnahNo ratings yet
- 10.2478 - Macvetrev 2019 0025Document3 pages10.2478 - Macvetrev 2019 0025Dayana MariaNo ratings yet
- Parasitxpert Newsletter2 PreviewDocument6 pagesParasitxpert Newsletter2 PreviewBirdella GwenNo ratings yet
- $RG8JJJ1Document82 pages$RG8JJJ1Rasha mohammadNo ratings yet
- Dirofilaria Ojo PerroDocument7 pagesDirofilaria Ojo PerroMaría Cristina Alayo RodríguezNo ratings yet
- Pi Is 2352512622004027Document4 pagesPi Is 23525126220040277dsp7xvs8dNo ratings yet
- Dermatology WorkbookDocument162 pagesDermatology Workbookwisegot586No ratings yet
- Acrodermatitis Enteropathica - A Case Report: Rashmi Mittal, Sudha R, Murugan S, Adikrishnan, Shobana S, Anandan SDocument3 pagesAcrodermatitis Enteropathica - A Case Report: Rashmi Mittal, Sudha R, Murugan S, Adikrishnan, Shobana S, Anandan SMarcelitaTaliaDuwiriNo ratings yet
- Jurnal NexgardDocument5 pagesJurnal NexgardadelliaputryNo ratings yet
- Case Report DemodicosisDocument8 pagesCase Report DemodicosisMateoNo ratings yet
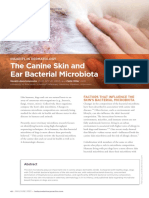
- TVP-2023-0506 Canine Ear MicrobiotaDocument6 pagesTVP-2023-0506 Canine Ear MicrobiotavetthamilNo ratings yet
- Wood Lamp Examination: Top 10 Forgotten Diagnostic ProceduresDocument1 pageWood Lamp Examination: Top 10 Forgotten Diagnostic Procedureslynn_mintoNo ratings yet
- 86 90 Case Report - Leishmaniasis - Audi - PDF 86 90 PDFDocument5 pages86 90 Case Report - Leishmaniasis - Audi - PDF 86 90 PDFJeddhie MoraNo ratings yet
- Lecture 4 - Bacterial Skin DiseasesDocument13 pagesLecture 4 - Bacterial Skin DiseasesandinadgNo ratings yet
- Chronic Mucocutaneous Candidiasis: A Case ReportDocument4 pagesChronic Mucocutaneous Candidiasis: A Case Reportselandia nisrinaNo ratings yet
- Atypical Manifestations of Tinea Corporis: Case ReportsDocument5 pagesAtypical Manifestations of Tinea Corporis: Case ReportsMuhammad HafizuddinNo ratings yet
- 3.fungal Corneal UlcerDocument33 pages3.fungal Corneal Ulcersajjad hossainNo ratings yet
- Mange in DogsDocument5 pagesMange in DogsMadhu DN100% (1)
- WL10Document2 pagesWL10sonaljain14143No ratings yet
- Akucewich, 2008Document9 pagesAkucewich, 2008Jessica VanyaNo ratings yet
- Vop 12566Document11 pagesVop 12566Blanca A SerranoNo ratings yet
- Skin Diseases of HamstersDocument12 pagesSkin Diseases of Hamstersqueen3400No ratings yet
- Treatment of Demodicosis With Pyoderma in Siberian Husky: A Case StudyDocument12 pagesTreatment of Demodicosis With Pyoderma in Siberian Husky: A Case StudyNuky RizkyNo ratings yet
- AD Review PDFDocument13 pagesAD Review PDFalfarizyjefryNo ratings yet
- Treatment of Demodicosis in Dogs: 2011 Clinical Practice GuidelinesDocument13 pagesTreatment of Demodicosis in Dogs: 2011 Clinical Practice GuidelinestahlokoNo ratings yet
- Dermatologic Problems of RabbitsDocument10 pagesDermatologic Problems of RabbitsLoreto Rojas PeraltaNo ratings yet
- Superficial Pyoderma: FeaturesDocument3 pagesSuperficial Pyoderma: FeaturesSitti AraNo ratings yet
- Synchro Studio 8: Getting Started and What's New in Version 8Document35 pagesSynchro Studio 8: Getting Started and What's New in Version 8Fernando Luis FerrerNo ratings yet
- Wine Storage - Sub Zero ICB424GSDocument2 pagesWine Storage - Sub Zero ICB424GSphilaskNo ratings yet
- Dossier & Dossier Assessment Process 2Document60 pagesDossier & Dossier Assessment Process 2sisay kassuNo ratings yet
- Lesson 2Document16 pagesLesson 2Vusani NeguyuniNo ratings yet
- Have Something Done EXERCISESDocument3 pagesHave Something Done EXERCISEScarlos laredoNo ratings yet
- 211-Article Text-399-1-10-20180522 PDFDocument42 pages211-Article Text-399-1-10-20180522 PDFAlex KanathNo ratings yet
- Variasi Dan Manfaat Teh Herbalife Nutrition: David Heber, M.D., PH.D., FACP, FASN Chairman Herbalife Nutrition InstituteDocument24 pagesVariasi Dan Manfaat Teh Herbalife Nutrition: David Heber, M.D., PH.D., FACP, FASN Chairman Herbalife Nutrition InstituteNimadefebyNo ratings yet
- Instruction Book Manual de Instrucciones Livre D'InstructionsDocument79 pagesInstruction Book Manual de Instrucciones Livre D'InstructionsWilfrido RosadoNo ratings yet
- Sailor Moon Episode 123 Sweet DreamsDocument4 pagesSailor Moon Episode 123 Sweet DreamssuveertamNo ratings yet
- Low-Cost Arrival Assistance Service Vietnam AirportDocument9 pagesLow-Cost Arrival Assistance Service Vietnam AirportvietnamfasttrackserviceNo ratings yet
- UntitledDocument22 pagesUntitledMoniNo ratings yet
- The Cattell-Horn-Carroll Theory of Cognitive AbilitiesDocument13 pagesThe Cattell-Horn-Carroll Theory of Cognitive Abilitiessergio_poblete_ortegaNo ratings yet
- CochinBase Tender E 13042021detailDocument27 pagesCochinBase Tender E 13042021detailisan.structural TjsvgalavanNo ratings yet
- PHP Viva QuestionsDocument8 pagesPHP Viva QuestionsFake AccountNo ratings yet
- INDIA Gherkin enDocument6 pagesINDIA Gherkin enmichelbgggNo ratings yet
- Listening and Note-Taking Week 01Document6 pagesListening and Note-Taking Week 01AlvinPennNo ratings yet
- The Importance of Mineral Elements For Humans, Domestic Animals and Plants: A ReviewDocument3 pagesThe Importance of Mineral Elements For Humans, Domestic Animals and Plants: A ReviewMaricel Canlas MacatoNo ratings yet
- Quantum Tunneling and Spin 14Document14 pagesQuantum Tunneling and Spin 14plfratarNo ratings yet
- Name: - ClassDocument4 pagesName: - ClassGumbNo ratings yet
- DIY GREENHOUSE by KMS - ChangelogDocument4 pagesDIY GREENHOUSE by KMS - Changeloglm pronNo ratings yet
- Siliporite Opx Pellets Revision 11 - 2017Document2 pagesSiliporite Opx Pellets Revision 11 - 2017Juan Victor Sulvaran Arellano100% (2)
- Friction Stir Processing PDFDocument7 pagesFriction Stir Processing PDFYazid HelalNo ratings yet
- HelicoptersDocument11 pagesHelicoptersJordan MosesNo ratings yet
- Session 2Document4 pagesSession 2vijayakumar100% (1)
- Dow Integraflux™ Ultrafiltration Modules: Product Data SheetDocument3 pagesDow Integraflux™ Ultrafiltration Modules: Product Data SheetArunkumar ChandaranNo ratings yet























































































Download as pdf or txt
You might also like
- July 23, 2009 Through August 24, 2009 JPMorgan Chase BankDocument4 pagesJuly 23, 2009 Through August 24, 2009 JPMorgan Chase BankMaria Blackburn33% (3)
- Multi Choice Tech 1 AnswerDocument20 pagesMulti Choice Tech 1 AnswerquyennqNo ratings yet
- Test Report Form: Candidate DetailsDocument1 pageTest Report Form: Candidate DetailsPranav BabbarNo ratings yet
- Adventure Travel Sample Marketing PlanDocument26 pagesAdventure Travel Sample Marketing PlanPalo Alto Software100% (9)
- Dispersive Characteristics of Clay Soil by Double HydrometerDocument3 pagesDispersive Characteristics of Clay Soil by Double Hydrometerโก อู๋No ratings yet
- Linear Organoid Nevus in A Dog (Pages 69-73)Document5 pagesLinear Organoid Nevus in A Dog (Pages 69-73)jenNo ratings yet
- Jurnal RSMH Palembang: Black Dot Type Capitis Tinea Appreciates Bacterial FoliculitisDocument5 pagesJurnal RSMH Palembang: Black Dot Type Capitis Tinea Appreciates Bacterial FoliculitisLailatuz ZakiyahNo ratings yet
- Lecture 4 - Bacterial Skin DiseasesDocument13 pagesLecture 4 - Bacterial Skin DiseasesticoypiperNo ratings yet
- PV0412 Mueller ADDocument4 pagesPV0412 Mueller ADtahlokoNo ratings yet
- Trichoscopic Diagnosis of Cutaneous Pelodera Strongyloides Infestation in A DogDocument5 pagesTrichoscopic Diagnosis of Cutaneous Pelodera Strongyloides Infestation in A DogRebeka MenezesNo ratings yet
- TVP 2018 0102 Banovic Canine Atopic Dermatitis 11Document18 pagesTVP 2018 0102 Banovic Canine Atopic Dermatitis 11Kimchi LynnNo ratings yet
- ElízabethDocument12 pagesElízabethJahir QHNo ratings yet
- Shell Rot Infection in Red Eared Turtle: August 2017Document3 pagesShell Rot Infection in Red Eared Turtle: August 2017dwi putriNo ratings yet
- UP Devon Rex Vet DermDocument7 pagesUP Devon Rex Vet Dermandrostona980No ratings yet
- An Idiopathic Facial Dermatitis of Persian CatsDocument7 pagesAn Idiopathic Facial Dermatitis of Persian CatsjenNo ratings yet
- Sterile Eosinophilic Pustule, Canine Subcorneal Pustular Dermatitis, Feline Hypereosinophilic Syndrome, Idiopathic Sterile GranulomaDocument15 pagesSterile Eosinophilic Pustule, Canine Subcorneal Pustular Dermatitis, Feline Hypereosinophilic Syndrome, Idiopathic Sterile GranulomaBiancaNo ratings yet
- Management of Corneal Ulcer PDFDocument2 pagesManagement of Corneal Ulcer PDFYosiita KartinaaNo ratings yet
- 1 s2.0 S2211753918301441 MainDocument4 pages1 s2.0 S2211753918301441 MainMateoNo ratings yet
- Gigitan SeranggaaDocument10 pagesGigitan Seranggaaashahs andjadgiNo ratings yet
- Scedosporium Apiospermum Keratomycosis in A DogDocument4 pagesScedosporium Apiospermum Keratomycosis in A DogDavid Argüelles AndradeNo ratings yet
- Capsules: (The in Brief)Document1 pageCapsules: (The in Brief)JeevaNo ratings yet
- Darier-White Disease: A Rare Genetic DisorderDocument4 pagesDarier-White Disease: A Rare Genetic Disorderanis utamiNo ratings yet
- NJKKMDocument4 pagesNJKKMAyu MabariaNo ratings yet
- Pyoderma DogsDocument7 pagesPyoderma DogstorqtechNo ratings yet
- Chronic Generalized Dermatophilosis in A BuffaloDocument3 pagesChronic Generalized Dermatophilosis in A BuffaloHendroNo ratings yet
- Ciclosporin Therapy For Canine Generalized Discoid LupusDocument6 pagesCiclosporin Therapy For Canine Generalized Discoid LupusPatrícia StancuNo ratings yet
- Mucinosis Por Un FarmadoDocument4 pagesMucinosis Por Un FarmadoLuluu CortésNo ratings yet
- Keratolyse Ponctuee Foot 1870519Document1 pageKeratolyse Ponctuee Foot 1870519redhaNo ratings yet
- Clinicalcytology 4 1125Document5 pagesClinicalcytology 4 1125Paula TorcheNo ratings yet
- BiodataDocument11 pagesBiodatabentubz100% (2)
- Inflammatory Tinea Capitis. A Clinical Case Presentation Treated With Oral TerbinafineDocument2 pagesInflammatory Tinea Capitis. A Clinical Case Presentation Treated With Oral TerbinafineSuci Triana PutriNo ratings yet
- Surface Infections 1st & 3rd Sept-2022Document7 pagesSurface Infections 1st & 3rd Sept-2022Doctor iVJNo ratings yet
- Tinea Versicolor of The Neck As Side Effect of Topical Steroids For Alopecia AreataDocument12 pagesTinea Versicolor of The Neck As Side Effect of Topical Steroids For Alopecia AreataNazihan Safitri AlkatiriNo ratings yet
- Progressive Langerhans' Cell Histiocytosis in A Puppy (Pages 241-246)Document6 pagesProgressive Langerhans' Cell Histiocytosis in A Puppy (Pages 241-246)jenNo ratings yet
- Acrodermatitis EnteropathicaDocument4 pagesAcrodermatitis EnteropathicaIntan FajrinNo ratings yet
- Case Report Tinea Corporis: By: Nurul Ayni Supervisor: Irma Tarida L, Dr. SP - KKDocument22 pagesCase Report Tinea Corporis: By: Nurul Ayni Supervisor: Irma Tarida L, Dr. SP - KKnurulayniNo ratings yet
- Lichen Amyloidosis With Combined Topical Therapy: A Case ReportDocument3 pagesLichen Amyloidosis With Combined Topical Therapy: A Case ReportmutmainnahNo ratings yet
- 10.2478 - Macvetrev 2019 0025Document3 pages10.2478 - Macvetrev 2019 0025Dayana MariaNo ratings yet
- Parasitxpert Newsletter2 PreviewDocument6 pagesParasitxpert Newsletter2 PreviewBirdella GwenNo ratings yet
- $RG8JJJ1Document82 pages$RG8JJJ1Rasha mohammadNo ratings yet
- Dirofilaria Ojo PerroDocument7 pagesDirofilaria Ojo PerroMaría Cristina Alayo RodríguezNo ratings yet
- Pi Is 2352512622004027Document4 pagesPi Is 23525126220040277dsp7xvs8dNo ratings yet
- Dermatology WorkbookDocument162 pagesDermatology Workbookwisegot586No ratings yet
- Acrodermatitis Enteropathica - A Case Report: Rashmi Mittal, Sudha R, Murugan S, Adikrishnan, Shobana S, Anandan SDocument3 pagesAcrodermatitis Enteropathica - A Case Report: Rashmi Mittal, Sudha R, Murugan S, Adikrishnan, Shobana S, Anandan SMarcelitaTaliaDuwiriNo ratings yet
- Jurnal NexgardDocument5 pagesJurnal NexgardadelliaputryNo ratings yet
- Case Report DemodicosisDocument8 pagesCase Report DemodicosisMateoNo ratings yet
- TVP-2023-0506 Canine Ear MicrobiotaDocument6 pagesTVP-2023-0506 Canine Ear MicrobiotavetthamilNo ratings yet
- Wood Lamp Examination: Top 10 Forgotten Diagnostic ProceduresDocument1 pageWood Lamp Examination: Top 10 Forgotten Diagnostic Procedureslynn_mintoNo ratings yet
- 86 90 Case Report - Leishmaniasis - Audi - PDF 86 90 PDFDocument5 pages86 90 Case Report - Leishmaniasis - Audi - PDF 86 90 PDFJeddhie MoraNo ratings yet
- Lecture 4 - Bacterial Skin DiseasesDocument13 pagesLecture 4 - Bacterial Skin DiseasesandinadgNo ratings yet
- Chronic Mucocutaneous Candidiasis: A Case ReportDocument4 pagesChronic Mucocutaneous Candidiasis: A Case Reportselandia nisrinaNo ratings yet
- Atypical Manifestations of Tinea Corporis: Case ReportsDocument5 pagesAtypical Manifestations of Tinea Corporis: Case ReportsMuhammad HafizuddinNo ratings yet
- 3.fungal Corneal UlcerDocument33 pages3.fungal Corneal Ulcersajjad hossainNo ratings yet
- Mange in DogsDocument5 pagesMange in DogsMadhu DN100% (1)
- WL10Document2 pagesWL10sonaljain14143No ratings yet
- Akucewich, 2008Document9 pagesAkucewich, 2008Jessica VanyaNo ratings yet
- Vop 12566Document11 pagesVop 12566Blanca A SerranoNo ratings yet
- Skin Diseases of HamstersDocument12 pagesSkin Diseases of Hamstersqueen3400No ratings yet
- Treatment of Demodicosis With Pyoderma in Siberian Husky: A Case StudyDocument12 pagesTreatment of Demodicosis With Pyoderma in Siberian Husky: A Case StudyNuky RizkyNo ratings yet
- AD Review PDFDocument13 pagesAD Review PDFalfarizyjefryNo ratings yet
- Treatment of Demodicosis in Dogs: 2011 Clinical Practice GuidelinesDocument13 pagesTreatment of Demodicosis in Dogs: 2011 Clinical Practice GuidelinestahlokoNo ratings yet
- Dermatologic Problems of RabbitsDocument10 pagesDermatologic Problems of RabbitsLoreto Rojas PeraltaNo ratings yet
- Superficial Pyoderma: FeaturesDocument3 pagesSuperficial Pyoderma: FeaturesSitti AraNo ratings yet
- Synchro Studio 8: Getting Started and What's New in Version 8Document35 pagesSynchro Studio 8: Getting Started and What's New in Version 8Fernando Luis FerrerNo ratings yet
- Wine Storage - Sub Zero ICB424GSDocument2 pagesWine Storage - Sub Zero ICB424GSphilaskNo ratings yet
- Dossier & Dossier Assessment Process 2Document60 pagesDossier & Dossier Assessment Process 2sisay kassuNo ratings yet
- Lesson 2Document16 pagesLesson 2Vusani NeguyuniNo ratings yet
- Have Something Done EXERCISESDocument3 pagesHave Something Done EXERCISEScarlos laredoNo ratings yet
- 211-Article Text-399-1-10-20180522 PDFDocument42 pages211-Article Text-399-1-10-20180522 PDFAlex KanathNo ratings yet
- Variasi Dan Manfaat Teh Herbalife Nutrition: David Heber, M.D., PH.D., FACP, FASN Chairman Herbalife Nutrition InstituteDocument24 pagesVariasi Dan Manfaat Teh Herbalife Nutrition: David Heber, M.D., PH.D., FACP, FASN Chairman Herbalife Nutrition InstituteNimadefebyNo ratings yet
- Instruction Book Manual de Instrucciones Livre D'InstructionsDocument79 pagesInstruction Book Manual de Instrucciones Livre D'InstructionsWilfrido RosadoNo ratings yet
- Sailor Moon Episode 123 Sweet DreamsDocument4 pagesSailor Moon Episode 123 Sweet DreamssuveertamNo ratings yet
- Low-Cost Arrival Assistance Service Vietnam AirportDocument9 pagesLow-Cost Arrival Assistance Service Vietnam AirportvietnamfasttrackserviceNo ratings yet
- UntitledDocument22 pagesUntitledMoniNo ratings yet
- The Cattell-Horn-Carroll Theory of Cognitive AbilitiesDocument13 pagesThe Cattell-Horn-Carroll Theory of Cognitive Abilitiessergio_poblete_ortegaNo ratings yet
- CochinBase Tender E 13042021detailDocument27 pagesCochinBase Tender E 13042021detailisan.structural TjsvgalavanNo ratings yet
- PHP Viva QuestionsDocument8 pagesPHP Viva QuestionsFake AccountNo ratings yet
- INDIA Gherkin enDocument6 pagesINDIA Gherkin enmichelbgggNo ratings yet
- Listening and Note-Taking Week 01Document6 pagesListening and Note-Taking Week 01AlvinPennNo ratings yet
- The Importance of Mineral Elements For Humans, Domestic Animals and Plants: A ReviewDocument3 pagesThe Importance of Mineral Elements For Humans, Domestic Animals and Plants: A ReviewMaricel Canlas MacatoNo ratings yet
- Quantum Tunneling and Spin 14Document14 pagesQuantum Tunneling and Spin 14plfratarNo ratings yet
- Name: - ClassDocument4 pagesName: - ClassGumbNo ratings yet
- DIY GREENHOUSE by KMS - ChangelogDocument4 pagesDIY GREENHOUSE by KMS - Changeloglm pronNo ratings yet
- Siliporite Opx Pellets Revision 11 - 2017Document2 pagesSiliporite Opx Pellets Revision 11 - 2017Juan Victor Sulvaran Arellano100% (2)
- Friction Stir Processing PDFDocument7 pagesFriction Stir Processing PDFYazid HelalNo ratings yet
- HelicoptersDocument11 pagesHelicoptersJordan MosesNo ratings yet
- Session 2Document4 pagesSession 2vijayakumar100% (1)
- Dow Integraflux™ Ultrafiltration Modules: Product Data SheetDocument3 pagesDow Integraflux™ Ultrafiltration Modules: Product Data SheetArunkumar ChandaranNo ratings yet