Professional Documents
Culture Documents
6 Forastiere2003
6 Forastiere2003
Uploaded by
RivssOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
6 Forastiere2003
6 Forastiere2003
Uploaded by
RivssCopyright:
Available Formats
new england
The
journal of medicine
established in 1812 november 27 , 2003 vol. 349 no. 22
Concurrent Chemotherapy and Radiotherapy
for Organ Preservation in Advanced Laryngeal Cancer
Arlene A. Forastiere, M.D., Helmuth Goepfert, M.D., Moshe Maor, M.D., Thomas F. Pajak, Ph.D., Randal Weber, M.D.,
William Morrison, M.D., Bonnie Glisson, M.D., Andy Trotti, M.D., John A. Ridge, M.D., Ph.D., Clifford Chao, M.D.,
Glen Peters, M.D., Ding-Jen Lee, M.D., Ph.D., Andrea Leaf, M.D., John Ensley, M.D., and Jay Cooper, M.D.
abstract
background
Induction chemotherapy with cisplatin plus fluorouracil followed by radiotherapy is the From the Sidney Kimmel Comprehensive
standard alternative to total laryngectomy for patients with locally advanced laryngeal Cancer Center at Johns Hopkins, Baltimore
(A.A.F., D.-J.L.); the University of Texas
cancer. The value of adding chemotherapy to radiotherapy and the optimal timing of M.D. Anderson Cancer Center, Houston
chemotherapy are unknown. (H.G., M.M., R.W., W.M., B.G., C.C.); Radi-
ation Therapy Oncology Group Headquar-
ters, Philadelphia (T.F.P.); the H. Lee Mof-
methods fitt Cancer Center and Research Institute,
We randomly assigned patients with locally advanced cancer of the larynx to one of University of South Florida, Tampa (A.T.);
three treatments: induction cisplatin plus fluorouracil followed by radiotherapy, radio- Fox Chase Cancer Center, Philadelphia
(J.A.R.); the Department of Radiation On-
therapy with concurrent administration of cisplatin, or radiotherapy alone. The primary cology, University of Alabama, Birmingham
end point was preservation of the larynx. (G.P.); the Department of Veterans Affairs
New York Harbor Healthcare System,
Brooklyn (A.L.); the Karmanos Cancer In-
results stitute, Wayne State University School of
A total of 547 patients were randomly assigned to one of the three study groups. The me- Medicine, Detroit (J.E.); and the Depart-
dian follow-up period was 3.8 years. At two years, the proportion of patients who had an ment of Radiation Oncology, New York Uni-
versity Medical Center, New York (J.C.). Ad-
intact larynx after radiotherapy with concurrent cisplatin (88 percent) differed signifi- dress reprint requests to Dr. Forastiere at
cantly from the proportions in the groups given induction chemotherapy followed by ra- the Sidney Kimmel Comprehensive Cancer
diotherapy (75 percent, P=0.005) or radiotherapy alone (70 percent, P<0.001). The rate Center at Johns Hopkins, 1650 Orleans St.,
Suite G90, Baltimore, MD 21231-1000, or
of locoregional control was also significantly better with radiotherapy and concurrent at af@jhmi.edu.
cisplatin (78 percent, vs. 61 percent with induction cisplatin plus fluorouracil followed by
radiotherapy and 56 percent with radiotherapy alone). Both of the chemotherapy-based N Engl J Med 2003;349:2091-8.
Copyright © 2003 Massachusetts Medical Society.
regimens suppressed distant metastases and resulted in better disease-free survival than
radiotherapy alone. However, overall survival rates were similar in all three groups. The
rate of high-grade toxic effects was greater with the chemotherapy-based regimens (81
percent with induction cisplatin plus fluorouracil followed by radiotherapy and 82 per-
cent with radiotherapy with concurrent cisplatin, vs. 61 percent with radiotherapy alone).
The mucosal toxicity of concurrent radiotherapy and cisplatin was nearly twice as fre-
quent as the mucosal toxicity of the other two treatments during radiotherapy.
conclusions
In patients with laryngeal cancer, radiotherapy with concurrent administration of cis-
platin is superior to induction chemotherapy followed by radiotherapy or radiotherapy
alone for laryngeal preservation and locoregional control.
n engl j med 349;22 www.nejm.org november 27, 2003 2091
The New England Journal of Medicine
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on October 28, 2014. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
with a stage T1 primary tumor (defined as tumor
e ach year, approximately 9500 per-
sons in the United States receive the diag-
nosis of cancer of the larynx.1 Until the
early 1990s, the standard treatment for locally ad-
vanced disease was total laryngectomy. This practice
limited to one subsite of the supraglottis or limited
to the vocal cords, with normal vocal-cord mobility,
according to the tumor–node–metastasis [TNM]
staging system) or with large-volume stage T4 dis-
changed, however, after the landmark trial conduct- ease (defined as a tumor penetrating through the
ed by the Department of Veterans Affairs Laryngeal cartilage or extending more than 1 cm into the base
Cancer Study Group, in which induction chemo- of the tongue) were not eligible. The disease had to
therapy (cisplatin plus fluorouracil) followed by ra- be considered curable with surgery and postopera-
diotherapy was compared with surgery plus adju- tive radiotherapy. A Karnofsky performance score of
vant radiotherapy.2 The larynx was preserved in 64 at least 60 (on a scale from 0 to 100, with higher
percent of the patients who received the nonsurgical scores indicating better performance and with a
treatment, and the two-year survival rate was 68 per- score of 60 indicating that the patient requires occa-
cent in both groups. No significant difference in sional assistance but is able to care for most of his
survival has been reported after more than 10 years or her own needs) was required. To be eligible, pa-
of follow-up.3 The ability to preserve the larynx with- tients also had to have a white-cell count of at least
out jeopardizing survival established the use of in- 3500 per cubic millimeter, a platelet count of at least
duction chemotherapy followed by radiotherapy as 100,000 per cubic millimeter, a normal serum calci-
an alternative to laryngectomy for locally advanced um level, and a creatinine clearance of at least 50 ml
laryngeal cancer. per minute. All the patients gave written informed
To determine the contributions of chemotherapy consent in accordance with institutional guidelines.
and radiotherapy to larynx-preserving treatment, the Pretreatment staging, involving laryngoscopy,
Radiation Therapy Oncology Group and the Head measurement of the tumor, and high-resolution
and Neck Intergroup conducted a randomized trial computed tomographic (CT) scanning of the pri-
(RTOG 91-11) to investigate three radiation-based mary tumor and the neck, was performed within
treatments: induction cisplatin plus fluorouracil fol- four weeks before entry into the study. To rule out
lowed by radiotherapy if there was a response to the synchronous primary cancers, either CT imaging of
chemotherapy (a regimen identical to that given the the chest and barium esophagography or pan-
“experimental” group in the Department of Veter- endoscopy (i.e., esophagoscopy and bronchoscopy)
ans Affairs Laryngeal Cancer Study Group trial), ra- was performed. Imaging was performed as clinical-
diotherapy with concurrent administration of cis- ly indicated to rule out metastatic disease.
platin, and radiotherapy alone. The rationale for the
second group was based on the enhancement of ra- treatment
diation effects on tumor cells by concurrent treat- Chemotherapy
ment with cisplatin. The primary objective of the tri- Induction chemotherapy consisted of cisplatin giv-
al was to compare the rates of laryngeal preservation en intravenously at a dose of 100 mg per square
associated with the three treatments. The study in- meter of body-surface area on day 1 and fluorouracil
volved investigators from the Radiation Therapy On- given at a dose of 1000 mg per square meter every 24
cology Group (the coordinating group), the South- hours by continuous intravenous infusion for 120
west Oncology Group, and the Eastern Cooperative hours, every three weeks for two courses. Patients
Oncology Group. then underwent evaluation by indirect laryngoscopy
and CT imaging of the neck. If these examinations
methods showed a complete or partial response of the pri-
mary tumor and no sign of progression in the neck,
patients a third course of cisplatin plus fluorouracil was
Patients were eligible if they had biopsy-proven, pre- given, followed by radiotherapy. Patients with a less
viously untreated stage III or IV (according to the than partial response of the primary tumor or with
staging system of the American Joint Commission progression in the neck underwent laryngectomy
on Cancer) squamous-cell carcinoma of the glottic followed by adjuvant radiotherapy. Patients as-
or supraglottic larynx, the surgical treatment of signed to radiotherapy with concurrent cisplatin
which would require total laryngectomy. Patients received intravenous cisplatin at a dose of 100 mg
2092 n engl j med 349;22 www.nejm.org november 27 , 2003
The New England Journal of Medicine
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on October 28, 2014. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
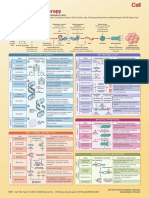
organ-preservation treatments for advanced laryngeal cancer
per square meter on days 1, 22, and 43 of radio- study design
therapy. Randomization
Patients were stratified according to the site of the
Radiotherapy primary tumor (glottic or supraglottic), N stage
The dose of radiation and radiotherapy schedule (stage N0 or N1 or stage N2 or N3), and primary tu-
were the same in all three study groups. The dose of mor stage (T2; T3 with fixed cord involvement; T3
radiation to the primary tumor and clinically posi- with no cord fixation but with invasion of the post-
tive nodes was 70 Gy, given in 35 fractions of 2 Gy cricoird area, medial wall of the pyriform sinus, or
each over a seven-week period. The entire neck, in- preepiglottic tissues; or T4). The randomization
cluding the supraclavicular areas and the posterior scheme described by Zelen6 was used to achieve bal-
neck, was irradiated with a minimum of 50 Gy. The ance in the treatment assignments among the insti-
dose to the clinically positive nodes was supple- tutions.
mented with the beams that covered the primary
tumor, with electrons, or with tangential anteropos- Study End Points
terior beams. The patients assigned to induction The primary end point was preservation of the lar-
chemotherapy followed by radiotherapy who under- ynx. Treatment was considered to have failed on the
went salvage surgery because of a poor response to date laryngectomy was performed. Other end points
the chemotherapy received adjuvant radiotherapy analyzed were overall survival, disease-free survival,
(50 to 70 Gy), depending on the status of the mar- local control, locoregional control, the time to dis-
gins on pathological review. tant metastasis, and laryngectomy-free survival. All
events were measured from the date of randomiza-
Surgery tion to the date of their occurrence or the date of the
Patients who had either a single lymph node 3 cm last follow-up visit. Toxic effects were graded ac-
or greater in diameter or multiple lymph-node me- cording to the National Cancer Institute Common
tastases on initial clinical staging of the neck were Toxicity Criteria, version 1.0, during induction che-
required to undergo neck dissection eight weeks motherapy and according to the Radiation Therapy
after the completion of radiotherapy. Laryngectomy Oncology Group toxicity criteria during radiother-
was performed in patients who had histologically apy. All deaths occurring during treatment or with-
proven persistent or recurrent carcinoma after the in 30 days after the completion of treatment were
completion of treatment or who had an inadequate considered to be possibly treatment-related.
response after two courses of induction chemo-
therapy. statistical analysis
The trial was designed to test whether concurrent
follow-up after the completion chemotherapy and radiotherapy or radiotherapy
of treatment alone resulted in higher rates of laryngeal preser-
All the patients were evaluated eight weeks after the vation than that achieved with standard induction
completion of therapy by examination of the head chemotherapy followed by radiotherapy. Since the
and neck and CT imaging. If persistent disease was protocol involved the comparison of two groups re-
suspected, examination while the patient was under ceiving experimental treatments with a single con-
anesthesia and direct laryngoscopy were performed. trol group, Dunnett’s two-sided test7 was used to
Complete examination of the head and neck, with adjust for multiple comparisons. The sample size
evaluation for late toxicity, was performed at sched- was calculated with the use of Bristol’s modifica-
uled follow-up visits. tion.8 The study was designed to detect an absolute
Two questionnaires, to be completed by the pa- difference of 15 percent with type I and type II error
tients, were used to evaluate quality of life: the Func- rates of 0.05 and 0.20. The sample size was further
tional Assessment of Cancer Therapy — Head and increased by 10 percent to account for patients
Neck Scale, version 2,4 and the University of Wash- deemed ineligible or lost to follow-up before two
ington Quality of Life instrument.5 These question- years had elapsed. The targeted sample size was 546
naires were to be filled out at base line and at each patients, assuming a two-year laryngectomy-free
follow-up visit. Results with respect to swallowing survival rate of 65 percent.
ability and speech are reported in this article. Rates of overall survival, disease-free survival,
n engl j med 349;22 www.nejm.org november 27, 2003 2093
The New England Journal of Medicine
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on October 28, 2014. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
incidence10 and were tested according to Gray’s
Table 1. Characteristics of the Patients According to the Treatment Group.*
method.11
Cisplatin plus Radiotherapy Differences in the timing of protocol-specified
Fluorouracil with assessments of disease among the treatment groups
Followed by Concurrent Radiotherapy
Radiation Cisplatin Alone could bias the results. For example, patients in the
Characteristic (N=173) (N=172) (N=173) induction-chemotherapy group could proceed to
Age laryngectomy earlier than the other patients because
<60 yr — no. (%) 91 (53) 83 (48) 89 (51)
of the evaluation performed at six weeks. To mini-
mize such bias, all laryngectomies performed with-
≥60 yr — no. (%) 82 (47) 89 (52) 84 (49)
in the first six months after the start of treatment
Median — yr 59 60 59
were considered to be early treatment failures and
Range — yr 36–78 26–78 31–79
were analyzed as if they had occurred at the same
Sex — no. (%) time.
Male 131 (76) 137 (80) 133 (77)
Female 42 (24) 35 (20) 40 (23)
results
Karnofsky performance score
— no. (%) patient population
100 35 (20) 32 (19) 26 (15) From August 1992 to May 2000, 547 patients were
90 88 (51) 106 (62) 93 (54) enrolled and randomly assigned to one of the three
80 38 (22) 27 (16) 41 (24) treatment groups. Twenty-one of these patients
70 10 (6) 6 (3) 10 (6) proved to be ineligible, one withdrew consent after
60 2 (1) 1 (1) 3 (2) randomization, and seven were excluded because
Site of tumor — no. (%) eligibility or outcome information was not submit-
Supraglottis 118 (68) 114 (66) 124 (72) ted. Thus, data from 518 patients were included in
Glottis 55 (32) 58 (34) 49 (28)
the analysis. The characteristics of the patients are
shown in Table 1. The site of the primary tumor and
American Joint Commission on
Cancer stage — no. (%) stage of disease were balanced among the three
III 111 (64) 115 (67) 111 (64) treatment groups.
IV 62 (36) 57 (33) 62 (36)
toxic effects
Tumor–node–metastasis stage
— no. (%)† Severe acute toxic effects are listed in Table 2. During
T stage induction chemotherapy with cisplatin and fluoro-
T2 19 (11) 21 (12) 20 (12) uracil, toxicity was manifested primarily as neutro-
T3 with fixed cord 82 (47) 82 (48) 76 (44) penia, stomatitis, and nausea or vomiting.
involvement
T3 without cord fixation 54 (31) 52 (30) 61 (35) The grade and frequency of toxic effects occur-
T4 18 (10) 17 (10) 16 (9) ring during radiotherapy recorded in the group that
N stage received induction cisplatin plus fluorouracil fol-
N0 87 (50) 86 (50) 87 (50) lowed by radiotherapy and the group that received
N1 38 (22) 39 (23) 32 (18)
N2A 2 (1) 7 (4) 3 (2)
radiotherapy alone were nearly identical and con-
N2B 17 (10) 13 (8) 13 (8) sisted mainly of grade 3 in-field effects on the skin
N2C 26 (15) 23 (13) 36 (21) and mucous membrane. In contrast, patients receiv-
N3 3 (2) 4 (2) 2 (1)
ing radiotherapy with concurrent cisplatin had che-
motherapy-related toxic effects (e.g., neutropenia
* Because of rounding, not all percentages total 100.
† T denotes tumor, and N node. The designation T4 was limited to low-volume and nausea or vomiting) and increased rates of se-
disease that did not extend into the tongue base by more than 1 cm or pene- vere radiation-related mucosal, pharyngeal, and
trate through cartilage. esophageal effects.
The incidence of grade 3 or 4 late toxic effects
and laryngectomy-free survival were estimated by was 24 percent in the group that received induction
means of the Kaplan–Meier method with the log- cisplatin plus fluorouracil followed by radiothera-
rank test.9 Rates of laryngeal preservation, local py, 30 percent in the group that received radiother-
control, locoregional control, and distant metas- apy with concurrent cisplatin, and 36 percent in
tasis were estimated by the method of cumulative the group that received radiotherapy alone. Most of
2094 n engl j med 349;22 www.nejm.org november 27 , 2003
The New England Journal of Medicine
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on October 28, 2014. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
organ-preservation treatments for advanced laryngeal cancer
Table 2. Grade 3 or 4 Acute Toxic Effects, According to the Treatment Group.*
Radiotherapy with Concurrent Radiotherapy Alone
Toxic Effect Cisplatin plus Fluorouracil Followed by Radiotherapy Cisplatin (N=171) (N=171)
Chemotherapy Period Radiotherapy Period
(N=168) (N=156)
grade 3 grade 4 total grade 3 grade 4 total grade 3 grade 4 total grade 3 grade 4 total
number of patients (percent)
Hematologic 43 44 87 (52) 13 10 23 (15) 64 17 81 (47) 3 2 5 (3)
Infection 4 5 9 (5) 2 0 2 (1) 7 0 7 (4) 2 0 2 (1)
Mucosal (stomatitis) 27 7 34 (20) 36 2 38 (24) 64 9 73 (43) 40 1 41 (24)
Pharyngeal or esophageal — — — 30 0 30 (19) 60 0 60 (35) 32 0 32 (19)
Laryngeal — — — 20 1 21 (13) 29 2 31 (18) 23 5 28 (16)
Dermatologic — — — 16 0 16 (10) 10 2 12 (7) 15 0 15 (9)
(in radiation field)
Nausea or vomiting 20 3 23 (14) 0 0 0 28 7 35 (20) 0 0 0
Renal or genitourinary 3 0 3 (2) 2 0 2 (1) 6 1 7 (4) 0 0 0
Neurologic 5 1 6 (4) 0 0 0 8 1 9 (5) 0 0 0
Other 20 7 27 (16) 16 2 18 (12) 58 11 69 (40) 9 1 10 (6)
Overall maximal severity 62 49 111 (66) 66 13 79 (51) 99 32 131 (77) 71 9 80 (47)
* Dashes denote not applicable.
these effects were grade 3 and referable to the larynx, to receive a third course of chemotherapy and a full
pharynx and esophagus, salivary glands, and subcu- course of radiotherapy. Of these, 134 received the
taneous tissues. third course; the remaining 10 discontinued che-
The total rates of severe toxic effects (acute and motherapy.
late) reported for all phases of the study were 81 per- Among the 24 patients in whom the response of
cent in the group assigned to induction cisplatin the primary tumor to induction chemotherapy was
plus fluorouracil followed by radiotherapy, 82 per- less than partial, only 7 proceeded to immediate
cent in the group assigned to radiotherapy with con- laryngectomy. Of the remaining 17 patients, 11 re-
current cisplatin, and 61 percent in the group as- ceived additional chemotherapy or radiotherapy. All
signed to radiotherapy alone. The total numbers 11 had a complete response, and only 1 subsequent-
of deaths that may have been related to treatment ly required a laryngectomy. Of the 172 patients ran-
were five (3 percent), nine (5 percent), and five domly assigned to receive radiotherapy with con-
(3 percent), respectively; the relation of the death to current cisplatin, 120 (70 percent) received all three
treatment was confirmed for four, eight, and two of planned doses of cisplatin and 40 (23 percent) re-
these deaths, respectively. ceived two doses.
Most of the patients (84 percent of those as-
response to treatment and compliance signed to induction cisplatin plus fluorouracil fol-
A total of 168 of the 173 patients assigned to receive lowed by radiotherapy, 91 percent of those assigned
induction cisplatin plus fluorouracil followed by ra- to radiotherapy with concurrent cisplatin, and 94
diotherapy received induction chemotherapy. The percent of those assigned to radiotherapy alone) re-
response of the primary tumor after two courses of ceived more than 95 percent of the intended dose of
cisplatin and fluorouracil was complete in 36 of radiotherapy (i.e., at least 67 Gy). At the completion
these patients (21 percent) and partial in 108 (64 of radiotherapy, 150 of the patients assigned to in-
percent). Eighty-four patients had nodal involve- duction cisplatin plus fluorouracil followed by ra-
ment, and the response was complete in 19 of them diotherapy, 154 of those assigned to radiotherapy
(23 percent), partial in 34 (40 percent), and stable with concurrent cisplatin, and 148 of those assigned
in 15 (18 percent). Thus, 144 patients could proceed to radiotherapy alone had had a complete response.
n engl j med 349;22 www.nejm.org november 27, 2003 2095
The New England Journal of Medicine
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on October 28, 2014. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
preservation of the larynx to radiotherapy with concurrent cisplatin, and 80
The rate of laryngeal preservation at a median fol- percent of those assigned to radiotherapy alone.
low-up of 3.8 years was significantly higher among There was no difference among the three treatment
patients receiving radiotherapy with concurrent cis- groups with regard to speech at either 12 or 24
platin (145 of 172 patients [84 percent]) than among months of follow-up. The reporting of moderate
those receiving induction chemotherapy followed speech impairment (difficulty in pronouncing some
by radiotherapy (125 of 173 patients [72 percent], words and being understood on the telephone) or
P=0.005) or radiotherapy alone (116 of 173 patients worse speech impairment did not differ among the
[67 percent], P<0.001). There was no significant dif- groups at one year (6 percent, 11 percent, and 13
ference between the group receiving induction che- percent, respectively) or two years (3 percent, 6 per-
motherapy followed by radiotherapy and the group cent, and 8 percent, respectively).
receiving radiotherapy alone (P=0.27) (Fig. 1). At one year, 23 percent of the patients assigned
to radiotherapy with concurrent cisplatin were able
speech and swallowing to swallow only soft foods or liquids, and 3 percent
Information on speech and swallowing collected could not swallow at all. By contrast, of the patients
from patients who were disease-free and had an in- assigned to induction cisplatin plus fluorouracil fol-
tact larynx was available from 74 percent of those as- lowed by radiotherapy, 9 percent were limited to soft
signed to induction cisplatin plus fluorouracil fol- foods or liquids, and none were unable to swallow
lowed by radiotherapy, 78 percent of those assigned (P=0.004). The results for the patients who received
only radiotherapy did not differ significantly from
those for the patients in the other two groups; 15
percent were limited to soft foods or liquids, and
100 3 percent could not swallow. At two years, there
Radiotherapy with concurrent cisplatin
was no significant difference among the groups in
Chemotherapy followed by radiotherapy the percentage of patients reporting difficulty in
Laryngeal Preservation
75
swallowing (16 percent of those assigned to induc-
(% of patients)
Radiotherapy alone
tion cisplatin plus fluorouracil followed by radio-
50 therapy, 15 percent of those assigned to radiother-
apy with concurrent cisplatin, and 14 percent of
25 those assigned to radiotherapy alone).
For the composite end point of laryngectomy-
free survival (on which the sample size of the trial
0 was predicated), either laryngectomy or death from
0.0 0.5 1.0 2.0 3.0 4.0 5.0
any cause constituted treatment failure. The two-
Years after Randomization
year and five-year estimated rates of this end point
No. at Risk
Chemotherapy followed 158 94 20 were 59 percent and 43 percent, respectively, for pa-
by radiotherapy tients assigned to induction cisplatin plus fluoro-
Radiotherapy with 154 107 28
concurrent cisplatin uracil followed by radiotherapy, 66 percent and 45
Radiotherapy alone 146 87 20 percent for those assigned to radiotherapy with con-
current cisplatin, and 53 percent and 38 percent for
Figure 1. Rates of Laryngeal Preservation According to the Treatment Group. those assigned to radiotherapy alone. The protocol-
At two years, the rates of laryngeal preservation were as follows: 75 percent specified test of statistical significance did not yield
(95 percent confidence interval, 68 to 81 percent) among the patients who re-
ceived induction cisplatin plus fluorouracil followed by radiotherapy, 88 per-
a significant difference (P<0.05) in pairwise com-
cent (95 percent confidence interval, 83 to 93 percent) among those who re- parisons between induction cisplatin plus fluoro-
ceived radiotherapy with concurrent cisplatin, and 70 percent (95 percent uracil followed by radiotherapy and radiotherapy
confidence interval, 63 to 76 percent) among those who received radiothera- with concurrent cisplatin (P=0.49) or between in-
py alone (P=0.005 for the comparison between induction cisplatin plus fluo- duction cisplatin plus fluorouracil followed by radio-
rouracil followed by radiotherapy and radiotherapy with concurrent cisplatin,
P=0.27 for the comparison between induction cisplatin plus fluorouracil fol-
therapy and radiotherapy alone (P=0.08). However,
lowed by radiotherapy and radiotherapy alone, and P<0.001 for the compari- there was a significant difference in laryngectomy-
son between radiotherapy with concurrent cisplatin and radiotherapy alone, free survival when concurrent radiotherapy and
by Gray’s test). cisplatin was compared with radiotherapy alone
(P=0.01).
2096 n engl j med 349;22 www.nejm.org november 27 , 2003
The New England Journal of Medicine
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on October 28, 2014. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
organ-preservation treatments for advanced laryngeal cancer
survival outcomes
The median follow-up among surviving patients 100
was 3.8 years. Two-year and five-year estimates of
Radiotherapy with concurrent cisplatin
overall survival did not differ significantly accord- 75
Locoregional Control
ing to the treatment: they were 76 percent and 55 Chemotherapy followed by radiotherapy
(% of patients)
percent, respectively, for induction cisplatin plus
fluorouracil followed by radiotherapy, 74 percent 50 Radiotherapy alone
and 54 percent for radiotherapy with concurrent cis-
platin, and 75 percent and 56 percent for radiother- 25
apy alone. Two-year and five-year estimates of dis-
ease-free survival were 52 percent and 38 percent,
respectively, for induction cisplatin plus fluoroura- 0
0.0 0.5 1.0 2.0 3.0 4.0 5.0
cil followed by radiotherapy, 61 percent and 36 per-
Years after Randomization
cent for radiotherapy with concurrent cisplatin, and
No. at Risk
44 percent and 27 percent for radiotherapy alone. Chemotherapy followed 147 89 19
Patients who received chemotherapy had signifi- by radiotherapy
Radiotherapy with 146 104 28
cantly improved disease-free survival as compared concurrent cisplatin
with those who received radiotherapy alone (P=0.02 Radiotherapy alone 127 78 19
for the comparison between induction cisplatin plus
fluorouracil followed by radiotherapy and radiother- Figure 2. Rates of Locoregional Control According to the Treatment Group.
apy alone, and P=0.006 for the comparison between At two years, the rates of locoregional control were as follows: 61 percent
radiotherapy with concurrent cisplatin and radio- (95 percent confidence interval, 54 to 69 percent) among the patients who
received induction cisplatin plus fluorouracil followed by radiotherapy, 78 per-
therapy alone). cent (95 percent confidence interval, 72 to 85 percent) among those who
received radiotherapy with concurrent cisplatin, and 56 percent (95 percent
pattern of failure confidence interval, 48 to 63 percent) among those who received radiothera-
At two years, the number of local treatment failures py alone (P=0.003 for the comparison between induction cisplatin plus fluo-
was 61 for induction cisplatin plus fluorouracil fol- rouracil followed by radiotherapy and radiotherapy with concurrent cisplatin,
P=0.16 for the comparison between induction cisplatin plus fluorouracil fol-
lowed by radiotherapy, 35 for radiotherapy with con- lowed by radiotherapy and radiotherapy alone, and P<0.001 for the compari-
current cisplatin, and 72 for radiotherapy alone. The son between radiotherapy with concurrent cisplatin and radiotherapy alone).
rates of local control were 64 percent, 80 percent,
and 58 percent, respectively. Patients who received
radiotherapy with concurrent cisplatin had signifi- therapy with concurrent cisplatin, and 16 percent of
cantly fewer failures than those who received in- those who had received radiotherapy alone. At five
duction cisplatin plus fluorouracil followed by ra- years, the cumulative recurrence rates were 15 per-
diotherapy (P=0.004) and significantly fewer than cent, 12 percent, and 22 percent, respectively. Over-
those who received radiotherapy alone (P<0.001). all, only the difference between the rates among
There was no significant difference with respect to those who received radiotherapy with concurrent
treatment failures between patients who received cisplatin and those who received radiotherapy alone
induction cisplatin plus fluorouracil followed by was significant (P=0.03).
radiotherapy and those who received radiotherapy
alone (P=0.15). Locoregional control was signifi- discussion
cantly better among the patients who received ra-
diotherapy with concurrent cisplatin than among In this trial, the overall survival among patients with
those who received either of the other treatments stage III or IV laryngeal cancer was excellent (75 per-
(Fig. 2). cent at two years) and did not differ significantly
according to the treatment. Laryngeal preservation
distant metastasis was best achieved with radiotherapy plus concurrent
Chemotherapy reduced the rate of distant metasta- cisplatin; induction chemotherapy followed by ra-
sis. At two years, distant metastases had developed diotherapy was not significantly better than radio-
in 9 percent of the patients who had received induc- therapy alone. With concurrent therapy, there was
tion cisplatin plus fluorouracil followed by radio- an absolute reduction in the rate of laryngectomy
therapy, 8 percent of those who had received radio- of 43 percent.
n engl j med 349;22 www.nejm.org november 27, 2003 2097
The New England Journal of Medicine
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on October 28, 2014. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
organ-preservation treatments for advanced laryngeal cancer
In addition, we found that chemotherapy sup- al, but rates of locoregional control did not differ
pressed distant metastasis. At two years, 91 percent significantly from those achieved with radiotherapy
of the patients who had received induction cisplatin alone. In addition, total toxicity was substantially in-
plus fluorouracil followed by radiotherapy and 92 creased as compared with radiotherapy alone. Thus,
percent of those who had received radiotherapy with for patients who desire laryngeal preservation when
concurrent cisplatin were metastasis-free, as com- concurrent administration of chemotherapy and
pared with 84 percent of those who had received ra- radiotherapy is not feasible, radiotherapy alone
diotherapy alone. At five years, these rates were 85 should be recommended.
percent, 88 percent, and 78 percent, respectively. Our finding — that concurrent administration of
Hence, the development of distant metastases was chemotherapy and radiotherapy is superior to se-
not merely delayed by chemotherapy. quential therapy or radiotherapy alone for achiev-
Induction chemotherapy followed by radiother- ing locoregional control — applies only to patients
apy was as toxic as concurrent therapy. Patients as- with stage III or IV disease (a T2, T3, or low-volume
signed to induction cisplatin plus fluorouracil fol- T4 primary tumor). It does not apply to patients with
lowed by radiotherapy had chemotherapy-related significant invasion of the tongue base or gross de-
toxic effects during the induction (preradiotherapy) struction of cartilage. Radiotherapy with concurrent
phase. The rate of toxic effects on the mucous mem- cisplatin should be considered standard care for pa-
branes and skin during radiotherapy in that group tients desiring laryngeal preservation whose cancer
was nearly identical to the rate in the group assigned is within the categories of disease studied in this
to radiotherapy alone, but the group assigned to trial, and laryngectomy should be performed only
radiotherapy with concurrent cisplatin had nearly as salvage therapy. We believe that in most patients
twice the rate of mucosal effects. The increased rate with laryngeal cancer, the disease can be managed
of acute toxic effects on the mucous membranes without a primary surgical approach.
with the use of radiotherapy with concurrent cisplat- Supported by research grants (CA21661, CA37422, CA32115,
CA06294, CA-32102, CA-20319, CA-46282, and CA49957) from the
in probably contributed to the delayed recovery of National Cancer Institute.
swallowing in this group (according to patients’ re- We are indebted to Dr. Victor Marcial for the development of this
ported quality-of-life assessment). trial; to the clinical investigators, statisticians, clinical research as-
sociates, administrative staff, and dosimetrists who contributed to
Induction chemotherapy followed by radiother- the success of this trial for their dedication and hard work; to Mr.
apy, as compared with radiotherapy alone, did not Brian A. Berkey for contributions to the statistical analysis; to Ms.
significantly improve the rate of laryngeal preserva- JoAnn Stetz and Ms. Rebecca Allegretto for contributions to data
management; and to Ms. Elizabeth Martin for contributions to qual-
tion or survival. It did suppress the development of ity assurance.
distant metastases and improve disease-free surviv-
refer enc es
1. Jemal A, Murray T, Samuels A, Ghafoor The Performance Status Scale for Head and ments with a control. J Am Stat Assoc 1955;
A, Ward E, Thun MJ. Cancer statistics, 2003. Neck Cancer Patients and the Functional As- 50:1096-121.
CA Cancer J Clin 2003;53:5-26. sessment of Cancer Therapy — Head and 8. Bristol DR. Designing clinical trials for
2. The Department of Veterans Affairs La- Neck Scale: a study of utility and validity. two-sided multiple comparisons with a con-
ryngeal Cancer Study Group. Induction che- Cancer 1996;77:2294-301. trol. Control Clin Trials 1989;10:142-52.
motherapy plus radiation compared with 5. Weymuller EA Jr, Alsarraf R, Yueh B, De- 9. Kaplan EL, Meier P. Nonparametric esti-
surgery plus radiation in patients with ad- leyiannis FW, Coltrera MD. Analysis of the mation from incomplete observations. J Am
vanced laryngeal cancer. N Engl J Med 1991; performance characteristics of the University Stat Assoc 1958;53:457-81.
324:1685-90. of Washington Quality of Life instrument 10. Mantel N. Evaluation of survival data
3. Hong WK, Lippman SM, Wolf GT. Re- and its modification (UW-QOL-R). Arch Oto- and two new rank order statistics arising in
cent advances in head and neck cancer — laryngol Head Neck Surg 2001;127:489-93. its consideration. Cancer Chemother Rep
larynx preservation and cancer chemopre- 6. Zelen M. The randomization and strati- 1966;50:163-70.
vention: the Seventeenth Annual Richard fication of patients to clinical trials. J Chron- 11. Gray RJ. A class of K-sample tests for
and Hinda Rosenthal Foundation Award ic Dis 1974;27:365-75. comparing the cumulative incidence of a
Lecture. Cancer Res 1993;53:5113-20. 7. Dunnett CW. A multiple comparison competing risk. Ann Stat 1988;16:1141-54.
4. List MA, D’Antonio LL, Cella DF, et al. procedure from comparing several treat- Copyright © 2003 Massachusetts Medical Society.
2098 n engl j med 349;22 www.nejm.org november 27 , 2003
The New England Journal of Medicine
Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on October 28, 2014. For personal use only. No other uses without permission.
Copyright © 2003 Massachusetts Medical Society. All rights reserved.
You might also like
- Faiz M. KhanDocument850 pagesFaiz M. KhanMaryam MasudieNo ratings yet
- Physicians' Cancer Chemotherapy Drug Manual 2021 21st EditionDocument837 pagesPhysicians' Cancer Chemotherapy Drug Manual 2021 21st EditionAmalia Nurul UlumNo ratings yet
- First-Line Crizotinib Versus Chemotherapy in ALK-Positive Lung CancerDocument11 pagesFirst-Line Crizotinib Versus Chemotherapy in ALK-Positive Lung CancerRitam JoarderNo ratings yet
- Concurrent QTRXT For T3 LarynxDocument4 pagesConcurrent QTRXT For T3 LarynxporsanimedNo ratings yet
- Prognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated RadiotherapyDocument7 pagesPrognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated Radiotherapypp kabsemarangNo ratings yet
- Glandula SalivarDocument8 pagesGlandula SalivarporsanimedNo ratings yet
- Nej Mo A 1905287Document12 pagesNej Mo A 1905287Ari KurniawanNo ratings yet
- 2008 JAMA Anal Ca Chemo TrialDocument9 pages2008 JAMA Anal Ca Chemo TrialgammasharkNo ratings yet
- Ahmed 2011Document10 pagesAhmed 2011skribekbenjaminNo ratings yet
- EBRT in DTCDocument7 pagesEBRT in DTCElena FlorentinaNo ratings yet
- 11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayDocument8 pages11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayBridia BogarNo ratings yet
- Baumann 2013Document8 pagesBaumann 2013nimaelhajjiNo ratings yet
- Nejmp 038171Document3 pagesNejmp 038171Rifki Effendi SuyonoNo ratings yet
- 1 s2.0 036030169400461S MainDocument6 pages1 s2.0 036030169400461S MainKAGNo ratings yet
- Tanum1991 (Biopsia A Todos)Document5 pagesTanum1991 (Biopsia A Todos)ouf81No ratings yet
- Systemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal CancerDocument8 pagesSystemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal Canceralberto cabelloNo ratings yet
- Wagner1994 (No Hace Biopsia)Document7 pagesWagner1994 (No Hace Biopsia)ouf81No ratings yet
- CrizotinibDocument10 pagesCrizotinibLuca StamerraNo ratings yet
- Zaghloul 2017Document9 pagesZaghloul 2017Mauricio MerancioNo ratings yet
- MeduloblastomaDocument7 pagesMeduloblastomasilvia erfanNo ratings yet
- Kanker ParuDocument10 pagesKanker Parunovi hidayahNo ratings yet
- 10 1016@j Jfma 2018 01 015Document10 pages10 1016@j Jfma 2018 01 015darpa22No ratings yet
- 961 FullDocument5 pages961 FullWilliyoNo ratings yet
- Jco 2004 01 029Document7 pagesJco 2004 01 029सागर राऊतNo ratings yet
- Cross Trial - Preoperative Chemoradiotherapy For Esophageal or Junctional Cancer - Nejm 2012Document12 pagesCross Trial - Preoperative Chemoradiotherapy For Esophageal or Junctional Cancer - Nejm 2012api-308365861No ratings yet
- jpc05003 1070 1076 PDFDocument7 pagesjpc05003 1070 1076 PDFDaniel SmartNo ratings yet
- JCO 2003 Lin 631 7Document7 pagesJCO 2003 Lin 631 7Adhika Manggala DharmaNo ratings yet
- Klopp 2013Document8 pagesKlopp 2013Insighte ChildcareNo ratings yet
- Chapman2017 PDFDocument7 pagesChapman2017 PDFzanNo ratings yet
- Fonc 07 00177Document13 pagesFonc 07 00177Ihenanacho HappinessNo ratings yet
- RavesDocument10 pagesRavesyingming zhuNo ratings yet
- Adjuvant RadiotherapyDocument7 pagesAdjuvant Radiotherapyciko momonNo ratings yet
- Nejmoa 1112088Document11 pagesNejmoa 1112088Med MedNo ratings yet
- SouthAsianJCancer6115-2517942 065939Document5 pagesSouthAsianJCancer6115-2517942 065939Gibi SupitNo ratings yet
- Curran 2011Document9 pagesCurran 2011Nguyễn Hoàng PhúcNo ratings yet
- Accepted Manuscript: Seminars in Colon & Rectal SurgeryDocument21 pagesAccepted Manuscript: Seminars in Colon & Rectal Surgerynaylul farohahNo ratings yet
- Conventional Dose ChemotherapyDocument8 pagesConventional Dose ChemotherapyOnic AugustineNo ratings yet
- A Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerDocument9 pagesA Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerFarizka Dwinda HNo ratings yet
- Ournal of Linical Ncology: OriginalDocument10 pagesOurnal of Linical Ncology: OriginalMaulida Nurazmi OctaviaNo ratings yet
- 1 s2.0 S1051044322011903 MainDocument30 pages1 s2.0 S1051044322011903 MainEsmaeel Jafargholi RangrazNo ratings yet
- Intergroup 0123Document8 pagesIntergroup 0123radonc17No ratings yet
- Kapoor SchwannomaDocument7 pagesKapoor SchwannomaAna Clara Nunes SartoriNo ratings yet
- CapeOX ChronicleDocument22 pagesCapeOX ChronicleOttofianus Hewick KalangiNo ratings yet
- 10 Anos Cross Trial Jco2021Document11 pages10 Anos Cross Trial Jco2021alomeletyNo ratings yet
- View ContentDocument24 pagesView ContentDian AyuNo ratings yet
- Primary Concurrent Chemoradiation in Head and Neck Cancers With Weekly Cisplatin Chemotherapy: Analysis of Compliance, Toxicity and SurvivalDocument7 pagesPrimary Concurrent Chemoradiation in Head and Neck Cancers With Weekly Cisplatin Chemotherapy: Analysis of Compliance, Toxicity and Survivaldanu20No ratings yet
- 2019 Article 6402Document8 pages2019 Article 6402shahrasyiddNo ratings yet
- Ne W Engl and Journal MedicineDocument14 pagesNe W Engl and Journal Medicineapi-26302710No ratings yet
- Esophageal 1Document5 pagesEsophageal 1Prashanth KumarNo ratings yet
- Harrington 2015Document16 pagesHarrington 2015Geoffroy De VilmarestNo ratings yet
- NPCDocument8 pagesNPCArsy Mira PertiwiNo ratings yet
- Acs 06 02 167Document8 pagesAcs 06 02 167MixalisKaplanisNo ratings yet
- Ni Hms 519602Document21 pagesNi Hms 519602Nur Rissa MaharanyNo ratings yet
- (Mama) Brady1977Document7 pages(Mama) Brady1977Gabriela Silva MartinsNo ratings yet
- 3 254 1 PBDocument5 pages3 254 1 PBbeepboop20No ratings yet
- Pearls and Pitfalls in The Imaging of Targeted Therapy and Immunotherapy in Lung CancerDocument11 pagesPearls and Pitfalls in The Imaging of Targeted Therapy and Immunotherapy in Lung CancerNelson William UsnayoNo ratings yet
- MÁS RADIOTERAPIA SI RECAÍDA y Biopsia A Todos. 310 PersonasDocument13 pagesMÁS RADIOTERAPIA SI RECAÍDA y Biopsia A Todos. 310 Personasouf81No ratings yet
- Ca Tiroid 2 PDFDocument11 pagesCa Tiroid 2 PDFAlfindyNo ratings yet
- No Defiende BiopsiaDocument12 pagesNo Defiende Biopsiaouf81No ratings yet
- Local Recurrence After Breast-Conserving Surgery and RadiotherapyDocument6 pagesLocal Recurrence After Breast-Conserving Surgery and RadiotherapyLizeth Rios ZamoraNo ratings yet
- Papillary Microcarcinoma of The Thyroid-Prognostic Significance of Lymph Node Metastasis and MultifocalityDocument10 pagesPapillary Microcarcinoma of The Thyroid-Prognostic Significance of Lymph Node Metastasis and MultifocalityAZ RPNo ratings yet
- Cancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondFrom EverandCancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondNo ratings yet
- S.No. Type Medicine NameDocument6 pagesS.No. Type Medicine Namered petalsNo ratings yet
- Tabla Conversion RadiologicasDocument1 pageTabla Conversion RadiologicasRosa Esmeralda Rojas HernandezNo ratings yet
- 909-Hazardous Drugs Table - EviqDocument9 pages909-Hazardous Drugs Table - EviqMd Al AminNo ratings yet
- Monday KordeDocument19 pagesMonday KordeNational Press FoundationNo ratings yet
- TROPiCS-02 - JCO 2022Document16 pagesTROPiCS-02 - JCO 2022Nicola CrestiNo ratings yet
- Cancer Chemo TableDocument5 pagesCancer Chemo TableChristine NazarenoNo ratings yet
- งานเคมีบ าบัด กลุ่มงานเภสัชกรรม โรงพยาบาลราชวิถี ตาราง การเตรียมยา และความคงตัวของยาเคมีบ าบัด Reconstitution PreparationDocument11 pagesงานเคมีบ าบัด กลุ่มงานเภสัชกรรม โรงพยาบาลราชวิถี ตาราง การเตรียมยา และความคงตัวของยาเคมีบ าบัด Reconstitution Preparationtotoil22No ratings yet
- Quimioterapia TiposDocument2 pagesQuimioterapia TiposJorge AguilarNo ratings yet
- Acute Lymphoblastic Leukemia Treatment RegimensDocument4 pagesAcute Lymphoblastic Leukemia Treatment Regimensnur-aisyahkNo ratings yet
- Cancer Cures Cancer Treatments That Work - Top 10 Natural Cancer TreatmentsDocument8 pagesCancer Cures Cancer Treatments That Work - Top 10 Natural Cancer TreatmentsDr. Dennis Clark100% (1)
- UntitledDocument4 pagesUntitledToni FatoniNo ratings yet
- Daftar Referensi Fisika MedisDocument49 pagesDaftar Referensi Fisika MedisAdfal AfdalaNo ratings yet
- Hospital Tengku Ampuan RahimahDocument14 pagesHospital Tengku Ampuan Rahimahmyvi317No ratings yet
- New ATC Code Substance NameDocument24 pagesNew ATC Code Substance NameRieka NurulNo ratings yet
- Sistim Pencitraan Kedokteran Nuklir: Nur Rahmah Hidayati, M.SCDocument7 pagesSistim Pencitraan Kedokteran Nuklir: Nur Rahmah Hidayati, M.SCSalsabila LuvaridianNo ratings yet
- Lung CA HandoutDocument8 pagesLung CA HandoutEnzo TimbolNo ratings yet
- Lapstok Ca 231223Document2 pagesLapstok Ca 231223farmasi.cancer.alihsanNo ratings yet
- Table HandlingDocument5 pagesTable HandlingbayuNo ratings yet
- ChemoStabilityChartApril2013 Formatted 2Document90 pagesChemoStabilityChartApril2013 Formatted 2Fyana PutriNo ratings yet
- Antineoplastic Drugs Lecture 1Document14 pagesAntineoplastic Drugs Lecture 1sky.blueNo ratings yet
- Abstract Book AIRO 2019Document280 pagesAbstract Book AIRO 2019Fab SanNo ratings yet
- Doxorubicin (Conventional) : Drug Information - UpToDateDocument55 pagesDoxorubicin (Conventional) : Drug Information - UpToDateramangNo ratings yet
- Kemoterapi YONDocument66 pagesKemoterapi YONAulia Chaya KusumaNo ratings yet
- 3 - Clinical Pharmacology of ChemotherapyDocument111 pages3 - Clinical Pharmacology of ChemotherapyChinIsiangSocitoNo ratings yet
- CGHS Rates PDFDocument5 pagesCGHS Rates PDFakshay100% (1)
- Kegunaan LinacDocument2 pagesKegunaan LinaccicichepiNo ratings yet
- Radiation Oncology: DR - Durgesh Mishra Dy - Cmo, MJPJAY, MahDocument13 pagesRadiation Oncology: DR - Durgesh Mishra Dy - Cmo, MJPJAY, MahKASATSANo ratings yet
- CCO NSCLC Practical Guidance DownloadableDocument109 pagesCCO NSCLC Practical Guidance DownloadableKhai Diệp HoàngNo ratings yet