Download as pdf or txt
You might also like
- Chapter 3 Elements For Design ConceptDocument76 pagesChapter 3 Elements For Design ConceptXarbie Rebadomia100% (2)
- Three-Dimensional Imaging in Orthodontics: ReviewDocument9 pagesThree-Dimensional Imaging in Orthodontics: Reviewdrzana78No ratings yet
- An Approach For Three-Dimensional Visualization Using High-Resolution MRI of The Temporomandibular JointDocument7 pagesAn Approach For Three-Dimensional Visualization Using High-Resolution MRI of The Temporomandibular JointПавло БурлаковNo ratings yet
- Qims 11 04 1447Document11 pagesQims 11 04 1447hanna.newestNo ratings yet
- Rotator Cuff Tear: ImagingDocument7 pagesRotator Cuff Tear: ImagingAurelie VainNo ratings yet
- Assessing The Diagnostic Precision of Cone Beam Computed Tomography (CBCT) in Temporomandibular Joint Arthritis: A Comprehensive ReviewDocument4 pagesAssessing The Diagnostic Precision of Cone Beam Computed Tomography (CBCT) in Temporomandibular Joint Arthritis: A Comprehensive ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Interpretation of Mandibular Condyle Fractures Using 2d-And 3D-Computed TomographyDocument6 pagesInterpretation of Mandibular Condyle Fractures Using 2d-And 3D-Computed TomographyhaneefmdfNo ratings yet
- Dentistry 12 00082Document13 pagesDentistry 12 00082adiNo ratings yet
- Tian 2012Document6 pagesTian 2012Orto MespNo ratings yet
- Condylar Volume and Surface in Caucasian Young Adult SubjectsDocument10 pagesCondylar Volume and Surface in Caucasian Young Adult SubjectsДенис КравченкоNo ratings yet
- Use of Three Dimensional Computerized Tomography Reconstruction in Complex Facial TraumaDocument7 pagesUse of Three Dimensional Computerized Tomography Reconstruction in Complex Facial TraumaMuh IqbalNo ratings yet
- 3D Echocardiography in Mitral Valve ProlapseDocument18 pages3D Echocardiography in Mitral Valve Prolapsericardo villaNo ratings yet
- PUSs 0041 1723876Document7 pagesPUSs 0041 1723876MarinaNo ratings yet
- Texture Spectrum Coupled With Entropy and Homogeneity Image Fea-Tures For Myocardium Muscle CharacterizationDocument10 pagesTexture Spectrum Coupled With Entropy and Homogeneity Image Fea-Tures For Myocardium Muscle CharacterizationDimona MoldovanuNo ratings yet
- Hossein JDocument6 pagesHossein JyaniNo ratings yet
- Diagnostic Value and Forensic Relevance of A Novel Photorealistic 3D Reconstruction TechniqueDocument7 pagesDiagnostic Value and Forensic Relevance of A Novel Photorealistic 3D Reconstruction TechniqueYosef CnnNo ratings yet
- Computers in Biology and Medicine: SciencedirectDocument7 pagesComputers in Biology and Medicine: SciencedirectlulukzNo ratings yet
- 2021 Treatment of The Temporomandibular Joint Ankylosis With A Customized Prosthesis in A Single Stage The Use of 3D Cutting Guides and Virtual Surgical PlanningDocument4 pages2021 Treatment of The Temporomandibular Joint Ankylosis With A Customized Prosthesis in A Single Stage The Use of 3D Cutting Guides and Virtual Surgical PlanningAlbert OliveraNo ratings yet
- BMC Musculoskeletal DisordersDocument7 pagesBMC Musculoskeletal DisordersTinkovan IonNo ratings yet
- Httpssci Hub - Sedownloads2020!10!24e9athlani2020.pdfdownload TrueDocument9 pagesHttpssci Hub - Sedownloads2020!10!24e9athlani2020.pdfdownload TrueJosé Miguel Molina MárquezNo ratings yet
- NJMS 3 2Document8 pagesNJMS 3 2anca_adam_26No ratings yet
- Assessment of Central Cartilaginous Tumor of The Appendicular Bone: Inter-Observer and Intermodality Agreement and Comparison of Diagnostic Performance of CT and MRIDocument11 pagesAssessment of Central Cartilaginous Tumor of The Appendicular Bone: Inter-Observer and Intermodality Agreement and Comparison of Diagnostic Performance of CT and MRIsilvana mendoncaNo ratings yet
- The Role of MRI Quantitative Assessment in PreoperativeDocument8 pagesThe Role of MRI Quantitative Assessment in PreoperativeRonWuNo ratings yet
- Three-Dimensional Cone Beam Computed Tomography Analysis of Temporomandibular Joint Response To The Twin-Block Functional ApplianceDocument12 pagesThree-Dimensional Cone Beam Computed Tomography Analysis of Temporomandibular Joint Response To The Twin-Block Functional AppliancealejandroNo ratings yet
- 17 Rajpal EtalDocument4 pages17 Rajpal EtaleditorijmrhsNo ratings yet
- Lumbosacral Plexus # 6Document6 pagesLumbosacral Plexus # 6Arcel De Luca G.No ratings yet
- Classification of Knee MRIDocument3 pagesClassification of Knee MRIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Contemporary Imaging For The Diagnosis and Treatment of Traumatic Dental Injuries: A ReviewDocument8 pagesContemporary Imaging For The Diagnosis and Treatment of Traumatic Dental Injuries: A Reviewkartika tiaraNo ratings yet
- JDigitalImaging Alessio 2019Document12 pagesJDigitalImaging Alessio 2019titelcosminelNo ratings yet
- Improved MaskrcnnDocument13 pagesImproved MaskrcnnVainavi SamantNo ratings yet
- Advanced Radiographic Techniques PDFDocument21 pagesAdvanced Radiographic Techniques PDFelokfaiqNo ratings yet
- International Journal of Radiography Imaging & Radiation TherapyDocument13 pagesInternational Journal of Radiography Imaging & Radiation TherapyAtul Kumar GoyalNo ratings yet
- BJR 20140542Document8 pagesBJR 20140542Sava Marius ConstantinNo ratings yet
- Diffusion-Weighted MR Imaging Gor Characterizing Muskuloskeletal LessionDocument17 pagesDiffusion-Weighted MR Imaging Gor Characterizing Muskuloskeletal LessionTika wahyuNo ratings yet
- Jips 20 387Document7 pagesJips 20 387anca_adam_26No ratings yet
- Prevalence, Diameter and Furring of Mandibular Incisive Canal in North Indian Subpopulation: A CBCT StudyDocument10 pagesPrevalence, Diameter and Furring of Mandibular Incisive Canal in North Indian Subpopulation: A CBCT StudyIJAR JOURNALNo ratings yet
- Detecting Statistically Significant Changes in Cartilage Thickness With Sub-Voxel PrecisionDocument1 pageDetecting Statistically Significant Changes in Cartilage Thickness With Sub-Voxel PrecisionadmonsalvoNo ratings yet
- Idea Proyecto 2Document13 pagesIdea Proyecto 2Marianne GillyNo ratings yet
- Accuracy of Xray and Mri in Defining Tumor MarginDocument7 pagesAccuracy of Xray and Mri in Defining Tumor MarginDinda SaviraNo ratings yet
- On The Opportunities and Challenges in Microwave Medical Sensing and ImagingDocument16 pagesOn The Opportunities and Challenges in Microwave Medical Sensing and Imagingpravinmali.pcNo ratings yet
- Research ArticleDocument11 pagesResearch Articletsania nkdNo ratings yet
- Max Illo Facial SurgeryDocument92 pagesMax Illo Facial Surgerychueychuan100% (1)
- Jurnal 3 - Imaging Anatomy of The Jaw and Dentition With Cone Beam Computed Tomography - Febby Sitti NurDocument11 pagesJurnal 3 - Imaging Anatomy of The Jaw and Dentition With Cone Beam Computed Tomography - Febby Sitti NurFEBBY SITTINo ratings yet
- Semi Automated Three Dimensional Condylar Reconstruction.Document5 pagesSemi Automated Three Dimensional Condylar Reconstruction.tamisatnamNo ratings yet
- Medical Image Analysis: Chenchu Xu, Joanne Howey, Pavlo Ohorodnyk, Mike Roth, Heye Zhang, Shuo LiDocument14 pagesMedical Image Analysis: Chenchu Xu, Joanne Howey, Pavlo Ohorodnyk, Mike Roth, Heye Zhang, Shuo LiSong Tae HaNo ratings yet
- Assessment of Imaging Factors Associated With Baker's Cyst Rupture On Knee MRIDocument7 pagesAssessment of Imaging Factors Associated With Baker's Cyst Rupture On Knee MRInikoje3448No ratings yet
- Edelson 2008Document11 pagesEdelson 2008reginapriscillaNo ratings yet
- A Three-Dimensional Cephalometric Analysis of Japanese Adults and Its Usefulness in Orthognathic Surgery A Retrospective StudyDocument11 pagesA Three-Dimensional Cephalometric Analysis of Japanese Adults and Its Usefulness in Orthognathic Surgery A Retrospective StudyPhachara SiripraphonrojNo ratings yet
- Annals of 3D Printed MedicineDocument7 pagesAnnals of 3D Printed MedicineИльяИльяNo ratings yet
- Kamnitsas2017 PDFDocument51 pagesKamnitsas2017 PDFsri_lntNo ratings yet
- Comparison of Cone-Beam Imaging With Orthopantomography and Computerized Tomography For Assessment in Presurgical Implant DentistryDocument10 pagesComparison of Cone-Beam Imaging With Orthopantomography and Computerized Tomography For Assessment in Presurgical Implant DentistryMihai DascalescuNo ratings yet
- Frameless Stereotactic Radiosurgery For Treatment of Multiple Sclerosis Erelated Trigeminal NeuralgiaDocument11 pagesFrameless Stereotactic Radiosurgery For Treatment of Multiple Sclerosis Erelated Trigeminal NeuralgiafespositoNo ratings yet
- Cone Beamed Computerized Dental Tomography in DentistryDocument5 pagesCone Beamed Computerized Dental Tomography in DentistryMeris JugadorNo ratings yet
- Erwin Rasyid,+2 3 3Document7 pagesErwin Rasyid,+2 3 3ikaNo ratings yet
- Three-Dimensional Computerized Orthognathic Surgical Treatment PlanningDocument10 pagesThree-Dimensional Computerized Orthognathic Surgical Treatment PlanningRajan KarmakarNo ratings yet
- The Egyptian Journal of Radiology and Nuclear Medicine: Mennatallah Hatem Shalaby, Shady Samir, Ahmed DeifDocument5 pagesThe Egyptian Journal of Radiology and Nuclear Medicine: Mennatallah Hatem Shalaby, Shady Samir, Ahmed DeifAhmad Ibrahim SalemNo ratings yet
- Analysis of Root Resorption in Dentistry Using Collaborative Tools & StrategiesDocument6 pagesAnalysis of Root Resorption in Dentistry Using Collaborative Tools & StrategiesIJERDNo ratings yet
- 2015 EJR Murtz 1,5 Vs 3T Braquial e SacralDocument7 pages2015 EJR Murtz 1,5 Vs 3T Braquial e SacralCaio DouradoNo ratings yet
- Aplicaciones Del CBCT en DTMDocument10 pagesAplicaciones Del CBCT en DTMDavid MonroyNo ratings yet
- 2017 - Use of MRI in Orthodontics - A ReviewDocument3 pages2017 - Use of MRI in Orthodontics - A ReviewSrdjan StojanovskiNo ratings yet
- Brain CTwith 64 and 16 Slice CTscancomparisonofimagequalityandradiationdosewithstandardprotocolsDocument5 pagesBrain CTwith 64 and 16 Slice CTscancomparisonofimagequalityandradiationdosewithstandardprotocolsIsaias Orlando Muchaypiña CanalesNo ratings yet
- (Vincent G. Duffy (Eds.) ) Digital Human Modeling. PDFDocument551 pages(Vincent G. Duffy (Eds.) ) Digital Human Modeling. PDFdiana nistoranNo ratings yet
- The Relationship Between Competition Stress and BiologicalDocument109 pagesThe Relationship Between Competition Stress and BiologicalizhamNo ratings yet
- B.arch Program Detailed Syllabus July 2020 FINALDocument272 pagesB.arch Program Detailed Syllabus July 2020 FINALSheeren Sitara ChelladuraiNo ratings yet
- HOLOGIC DXA Horizon SpecsDocument4 pagesHOLOGIC DXA Horizon SpecsJuan Pablo RamirezNo ratings yet
- AnthropometricsDocument5 pagesAnthropometricsNoel Dela CruzNo ratings yet
- LDDocument11 pagesLDSatish PaswanNo ratings yet
- Engineering Anthropometry and Workspace DesignDocument50 pagesEngineering Anthropometry and Workspace DesignFransiska KikiNo ratings yet
- BMI ClassificationDocument2 pagesBMI ClassificationRazi MaulanaNo ratings yet
- Nutritional Assessment For Children and AdolescentsDocument32 pagesNutritional Assessment For Children and AdolescentsOduntan DanielNo ratings yet
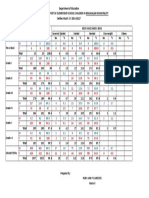
- Department of Education School Nutritional Status RecordDocument17 pagesDepartment of Education School Nutritional Status RecordSwitkizzes SwitkizzesNo ratings yet
- Analysis of Repeat Radiography and Corrective Measures in Teaching Hospital in Tertiary Health Care CentreDocument4 pagesAnalysis of Repeat Radiography and Corrective Measures in Teaching Hospital in Tertiary Health Care CentreIJAR JOURNALNo ratings yet
- Vinno M80 Brochures PDFDocument4 pagesVinno M80 Brochures PDFRim GhorbelNo ratings yet
- Che 208 CW-2Document2 pagesChe 208 CW-2Saria ChowdhuryNo ratings yet
- BMI SantanDocument1 pageBMI SantanRoque GeraleNo ratings yet
- Oral and Maxillofacial ImagingDocument34 pagesOral and Maxillofacial ImagingAtika Iftikhar MirNo ratings yet
- Ecografo Mindray DC 40 CatalogoDocument4 pagesEcografo Mindray DC 40 CatalogoCegnos TemucoNo ratings yet
- LST Published Price List 21jan2020 en PDFDocument1 pageLST Published Price List 21jan2020 en PDFIyad ShahatitNo ratings yet
- Importance in ArchitectureDocument10 pagesImportance in ArchitecturejamsnssNo ratings yet
- Radiology Procedure ManualDocument26 pagesRadiology Procedure Manualpurnima4uonlyNo ratings yet
- Nutritional Status TemplateDocument1 pageNutritional Status TemplateShangkiee Amora-TamborNo ratings yet
- SBFP Form 1: Master List Beneficiaries For School-Based Feeding Program (SBFP)Document18 pagesSBFP Form 1: Master List Beneficiaries For School-Based Feeding Program (SBFP)Verena RagaNo ratings yet
- Food Habits and Nutrient Intake of Bankers in Lagos StateDocument3 pagesFood Habits and Nutrient Intake of Bankers in Lagos StateIOSRjournalNo ratings yet
- Assignment 2 FingerprintsDocument6 pagesAssignment 2 Fingerprintsapi-242667307No ratings yet
- Original Article International Anthropometric Study of Facial Morphology in Various Ethnic Groups/RacesDocument32 pagesOriginal Article International Anthropometric Study of Facial Morphology in Various Ethnic Groups/RacesReem AltameemiNo ratings yet
- 2 To 20 Years: Girls Body Mass Index-For-Age Percentiles: Date Age Weight Stature Bmi CommentsDocument2 pages2 To 20 Years: Girls Body Mass Index-For-Age Percentiles: Date Age Weight Stature Bmi CommentsTaha Mohammed TahaNo ratings yet
- I.21.109 Sayan Samanta Presentation On PET CTDocument20 pagesI.21.109 Sayan Samanta Presentation On PET CTSayan SamantaNo ratings yet
- Radiology Downtime Workflow HSIJBDocument4 pagesRadiology Downtime Workflow HSIJBNazreenNo ratings yet
- 2021 Regional Nutrition SituationDocument38 pages2021 Regional Nutrition SituationMash JumahariNo ratings yet