Download as docx, pdf, or txt
You might also like
- Victorian AOD Intake ToolDocument5 pagesVictorian AOD Intake ToolHarjotBrarNo ratings yet
- Ekg FastlaneDocument10 pagesEkg FastlaneAida UzunovicNo ratings yet
- Manship App FormDocument4 pagesManship App Formjonheric2009No ratings yet
- Student Registration Form: (Last) (First) (Mi)Document1 pageStudent Registration Form: (Last) (First) (Mi)Gregory UtupoNo ratings yet
- Admission FormDocument6 pagesAdmission FormMichael EllisNo ratings yet
- APPLICATIONPediatric Radiology Fellowship071911RevisionpdfDocument3 pagesAPPLICATIONPediatric Radiology Fellowship071911RevisionpdfASIK1144No ratings yet
- Holmesglen App FormDocument8 pagesHolmesglen App FormssshalNo ratings yet
- IEU Application Form PolandDocument1 pageIEU Application Form PolandKbNo ratings yet
- Application Form For Undergraduate Programs: Program InformationDocument4 pagesApplication Form For Undergraduate Programs: Program InformationAbrar FarhanNo ratings yet
- Undergraduate Program Form Spring 2022Document4 pagesUndergraduate Program Form Spring 2022MAHABUBUL ISLAM NAYEMNo ratings yet
- Application Form 2023Document4 pagesApplication Form 2023eugene CortezNo ratings yet
- CIM Application Form 1 2020 2021Document4 pagesCIM Application Form 1 2020 2021Apple StarkNo ratings yet
- West Bengal Application FormDocument5 pagesWest Bengal Application Formmahesh100% (7)
- Application Form: For University Use OnlyDocument6 pagesApplication Form: For University Use OnlyCik IkoNo ratings yet
- Advt. No.9-2018 - 0Document7 pagesAdvt. No.9-2018 - 0salmansaleemNo ratings yet
- Espoir Academy Admission Application Editable 3.0Document3 pagesEspoir Academy Admission Application Editable 3.0regan.chetty07No ratings yet
- Sri Ramakrishna Engineering College: Student RecordDocument1 pageSri Ramakrishna Engineering College: Student RecordPriyanka. SNo ratings yet
- Application FormDocument7 pagesApplication Formadu kusiNo ratings yet
- Application Form (Chev/1)Document8 pagesApplication Form (Chev/1)aver04No ratings yet
- 2024 Borderlink Application OSDocument8 pages2024 Borderlink Application OSmchiromare75No ratings yet
- App FormDocument4 pagesApp FormTshiamo TabaneNo ratings yet
- University of Jhang: Admission FormDocument5 pagesUniversity of Jhang: Admission FormFairy QueenNo ratings yet
- University of Jhang: Admission FormDocument5 pagesUniversity of Jhang: Admission FormFairy QueenNo ratings yet
- VSB Student App Schools Nov2011Document3 pagesVSB Student App Schools Nov2011testNo ratings yet
- G Online Inspire ReadWriteData DocTemp 20221130215108433865981Document2 pagesG Online Inspire ReadWriteData DocTemp 20221130215108433865981Jitendra BNo ratings yet
- G Online Inspire ReadWriteData DocTemp 20220510213628451910617Document2 pagesG Online Inspire ReadWriteData DocTemp 20220510213628451910617aditya kumarNo ratings yet
- CSL Enrollment ContractDocument5 pagesCSL Enrollment ContractShenequa ScottNo ratings yet
- COSDEC Application Form 2023 SwakopmundDocument4 pagesCOSDEC Application Form 2023 SwakopmundvanwykchristajNo ratings yet
- (Form 1-B) Personal Data: San Beda University Graduate School of LawDocument2 pages(Form 1-B) Personal Data: San Beda University Graduate School of LawKash K. AsdaonNo ratings yet
- New Registration Form 2022Document2 pagesNew Registration Form 2022bp.7611No ratings yet
- Patient Registration Form 1 2018 Adult UpdatedDocument4 pagesPatient Registration Form 1 2018 Adult UpdatedEskinderNo ratings yet
- Case Management Assessment FormDocument13 pagesCase Management Assessment FormDiksha PadamNo ratings yet
- Full Time Application Form SU2023Document6 pagesFull Time Application Form SU2023Mohamed ElsagerNo ratings yet
- Youth Club App11Document3 pagesYouth Club App11api-357278378No ratings yet
- Student Registration FormDocument9 pagesStudent Registration FormAyu MuffinsNo ratings yet
- Alpha and Omega Bible Institutes Admin FormDocument3 pagesAlpha and Omega Bible Institutes Admin FormPaul MalekeNo ratings yet
- Application For Admission FormDocument2 pagesApplication For Admission FormVahid100% (1)
- 7 A 0 ADocument2 pages7 A 0 Antswakimathibela13No ratings yet
- Non-Adsb Student Registration FormDocument2 pagesNon-Adsb Student Registration FormAmeerah PoliquinNo ratings yet
- Kingsford Enrolment Application Form v2.0 LatestDocument2 pagesKingsford Enrolment Application Form v2.0 Latestalicante.rodel0iNo ratings yet
- IAESTE Nominated FormDocument1 pageIAESTE Nominated FormTomislav ČopNo ratings yet
- Case Management Assessment FormDocument13 pagesCase Management Assessment Formiman diarNo ratings yet
- Admission Form 2020 2021Document4 pagesAdmission Form 2020 2021FARMAN SHAIKH SAHABNo ratings yet
- Membership Form - Updated-Apr2023Document1 pageMembership Form - Updated-Apr2023Michael Vincent Estrada ObeñaNo ratings yet
- Application Form For The Post of Professor Associate Asst Professor 1Document7 pagesApplication Form For The Post of Professor Associate Asst Professor 1makwanadrashti1998No ratings yet
- State University of New York Application For New York State Residency Status For Tuition Billing PurposesDocument4 pagesState University of New York Application For New York State Residency Status For Tuition Billing PurposesDmitriy Oksenkrug-MizengendlerNo ratings yet
- Post RN - BSCN Program - 0Document4 pagesPost RN - BSCN Program - 0reynoldNo ratings yet
- Application Form - Libs 2019 2020Document4 pagesApplication Form - Libs 2019 2020Ajay AJNo ratings yet
- Personal Information Form (PIF) (Non-Taleo Only)Document2 pagesPersonal Information Form (PIF) (Non-Taleo Only)Daniel JuniorNo ratings yet
- Delhi Public Library Membership FormDocument1 pageDelhi Public Library Membership Formheart Touching Vedios Dil se Dil TakNo ratings yet
- BPS Application Documents Form Grade 1 7 2022Document7 pagesBPS Application Documents Form Grade 1 7 2022Raeesa SNo ratings yet
- Kaplan Pathways UK Application FormDocument4 pagesKaplan Pathways UK Application FormNguyễn Thu ThuỷNo ratings yet
- Student Biodata FormDocument1 pageStudent Biodata FormdalocanogacedominicNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormmaelisaNo ratings yet
- Annexure I (Student Profile) 1Document1 pageAnnexure I (Student Profile) 1Pravin KaushalNo ratings yet
- Application For Student Bursary Scheme 2022Document3 pagesApplication For Student Bursary Scheme 2022Prashant Singh RajputNo ratings yet
- International Application Form: Agent/ Representative Details Program SelectionDocument3 pagesInternational Application Form: Agent/ Representative Details Program SelectionKc Kirsten Kimberly MalbunNo ratings yet
- BCF FORM - DatamanDocument8 pagesBCF FORM - DatamanMudassirNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- Admission FormDocument1 pageAdmission FormJaycrisNo ratings yet
- 4 3 Minutes TemplateDocument2 pages4 3 Minutes TemplatedawnNo ratings yet
- 1976 Applied Maths Higher Level Questions 1Document4 pages1976 Applied Maths Higher Level Questions 1dawnNo ratings yet
- 1978 Applied Maths Higher Level Questions 1Document4 pages1978 Applied Maths Higher Level Questions 1dawnNo ratings yet
- British Vogue 2016Document1 pageBritish Vogue 2016dawnNo ratings yet
- 1977 Applied Maths Higher Level Questions 1Document4 pages1977 Applied Maths Higher Level Questions 1dawnNo ratings yet
- 1980 Applied Maths Higher Level Questions 1.: gcosβDocument3 pages1980 Applied Maths Higher Level Questions 1.: gcosβdawnNo ratings yet
- Safewards Mutual Help Meeting Minutes TemplateDocument1 pageSafewards Mutual Help Meeting Minutes TemplatedawnNo ratings yet
- 1970 Applied Maths Higher Level Questions 1Document4 pages1970 Applied Maths Higher Level Questions 1dawnNo ratings yet
- 002 Meeting Minute TemplateDocument4 pages002 Meeting Minute TemplatedawnNo ratings yet
- Action Minutes FormatDocument2 pagesAction Minutes FormatdawnNo ratings yet
- Board Meeting Agenda TemplateDocument3 pagesBoard Meeting Agenda TemplatedawnNo ratings yet
- Appl For Ind NumberDocument1 pageAppl For Ind NumberdawnNo ratings yet
- GEPIK Application FormDocument12 pagesGEPIK Application FormdawnNo ratings yet
- CGNZ 2021 Institute of Directors Board Meetings Minutes TemplateDocument1 pageCGNZ 2021 Institute of Directors Board Meetings Minutes TemplatedawnNo ratings yet
- British Vogue 2017Document1 pageBritish Vogue 2017dawnNo ratings yet
- WW Lev.2 No.8Document33 pagesWW Lev.2 No.8dawnNo ratings yet
- MT Meeting Notes TemplateDocument3 pagesMT Meeting Notes TemplatedawnNo ratings yet
- CR No.8Document20 pagesCR No.8dawnNo ratings yet
- Mentor ApplicationDocument1 pageMentor ApplicationdawnNo ratings yet
- WW Lev.1 No.8Document29 pagesWW Lev.1 No.8dawnNo ratings yet
- British Vogue 2018Document1 pageBritish Vogue 2018dawnNo ratings yet
- HRP 501 Template MinutesDocument4 pagesHRP 501 Template MinutesdawnNo ratings yet
- Libguides 2.0 Minutes Template 2Document2 pagesLibguides 2.0 Minutes Template 2dawnNo ratings yet
- CD AffidavitDocument1 pageCD AffidavitdawnNo ratings yet
- Site Meeting Minutes v2.2Document10 pagesSite Meeting Minutes v2.2dawnNo ratings yet
- Meeting Agenda and Minutes TemplateDocument2 pagesMeeting Agenda and Minutes TemplatedawnNo ratings yet
- Pop WW Lev1Document7 pagesPop WW Lev1dawnNo ratings yet
- Meeting Minutes TemplateDocument5 pagesMeeting Minutes TemplatedawnNo ratings yet
- NC Meeting Minutes Template enDocument2 pagesNC Meeting Minutes Template endawnNo ratings yet
- Trump WW Lev.2Document11 pagesTrump WW Lev.2dawnNo ratings yet
- Dr. Sunetta Monga, Core Outcome Set Development For Adolescent Depression TrialsDocument2 pagesDr. Sunetta Monga, Core Outcome Set Development For Adolescent Depression TrialsU of T MedicineNo ratings yet
- Dr. Didik Fetal Urogenital Anomalies Fetal Urogenital Anomalies PDFDocument25 pagesDr. Didik Fetal Urogenital Anomalies Fetal Urogenital Anomalies PDFJTNo ratings yet
- 2 3 Resource Book 2013Document4 pages2 3 Resource Book 2013api-246595728No ratings yet
- Voice & DysphagiaDocument8 pagesVoice & DysphagiaarpitaNo ratings yet
- Child AdoptionDocument3 pagesChild AdoptionKaren ReasonNo ratings yet
- Sigmund Freud BiographyDocument3 pagesSigmund Freud Biographyargatu100% (3)
- Module-5 Envirionmental Impact Assessment Dr. Saravanakumar Evs Chy1002Document33 pagesModule-5 Envirionmental Impact Assessment Dr. Saravanakumar Evs Chy1002Asheee100% (1)
- Collective Trauma Summit 2021 - Laurie - Leitch - The Social Resilience ModelDocument2 pagesCollective Trauma Summit 2021 - Laurie - Leitch - The Social Resilience ModelEmilia LarraondoNo ratings yet
- UV Light in Food PreservationDocument5 pagesUV Light in Food Preservation20125320No ratings yet
- Scanning Protocol Abdomen PelvisDocument2 pagesScanning Protocol Abdomen PelvisNur IzzwaniNo ratings yet
- 06 Senior Citizen PolicyDocument26 pages06 Senior Citizen PolicyJaimson FrancisNo ratings yet
- Orbitotomi MedscapeDocument9 pagesOrbitotomi MedscapeBonita AsyigahNo ratings yet
- Var TMP TMP Generated AABBTechnicalManual18thEd2014 AABB Technical Manual 18th Ed 2014Document824 pagesVar TMP TMP Generated AABBTechnicalManual18thEd2014 AABB Technical Manual 18th Ed 2014Hoàng Nguyễn VănNo ratings yet
- Solution Manual For Chemistry The Science in Context 5th Edition Thomas R Gilbert Rein V Kirss Natalie Foster Stacey Lowery Bretz Geoffrey DaviesDocument36 pagesSolution Manual For Chemistry The Science in Context 5th Edition Thomas R Gilbert Rein V Kirss Natalie Foster Stacey Lowery Bretz Geoffrey Daviescrampyunwashedj3tq2100% (49)
- Discussion Text ExerciseDocument4 pagesDiscussion Text ExerciseSri WachyuningsihNo ratings yet
- Ee BD ManualDocument37 pagesEe BD Manualsergey62No ratings yet
- Case Study Answers: Noon Business SchoolDocument6 pagesCase Study Answers: Noon Business SchoolMuhammad Arslan AkramNo ratings yet
- Program-Mechanical Engineering Code - 22509 Unit Outcome 2 - Explain The MainDocument28 pagesProgram-Mechanical Engineering Code - 22509 Unit Outcome 2 - Explain The MainKunal AhiwaleNo ratings yet
- 6 Nutritional InterventionDocument33 pages6 Nutritional InterventionNegeso JaraNo ratings yet
- Round 2 Total Seats For PG 2021 CounsellingDocument600 pagesRound 2 Total Seats For PG 2021 CounsellingSrikar BharadwajNo ratings yet
- Health Care Delivery Concerns, National Health andDocument26 pagesHealth Care Delivery Concerns, National Health andKavi rajputNo ratings yet
- Pengaruh Body Massage Terhadap Tingkat Depresi Ibu Nifas Di Bidan Praktik Mandiri Siyamtiningsih KaranganyarDocument8 pagesPengaruh Body Massage Terhadap Tingkat Depresi Ibu Nifas Di Bidan Praktik Mandiri Siyamtiningsih KaranganyarEnzel LinaNo ratings yet
- Activity Completion Report: District Brigada Eskwela Kick - Off CeremonyDocument13 pagesActivity Completion Report: District Brigada Eskwela Kick - Off CeremonyNoriza BocaboNo ratings yet
- Naskah Publikasi P1337430116020Document8 pagesNaskah Publikasi P1337430116020May JilbabNo ratings yet
- Puskesmas Soromandi Bima District of West Nusa Tenggara)Document7 pagesPuskesmas Soromandi Bima District of West Nusa Tenggara)chandra irawanNo ratings yet
- Active COVID-19 Workplace Outbreaks in Oregon (Published 10/7)Document5 pagesActive COVID-19 Workplace Outbreaks in Oregon (Published 10/7)KGW News100% (2)
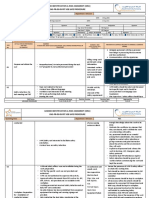
- OHS-PR-09-03-F07 JOB SAFE PROCEDURE (19) Installation of Conductor JumperDocument14 pagesOHS-PR-09-03-F07 JOB SAFE PROCEDURE (19) Installation of Conductor Jumpermohammed tofiqNo ratings yet
- Kawasaki Disease: Focus On Clinical Manifestation: Dr. I B Agung Winaya, SpaDocument24 pagesKawasaki Disease: Focus On Clinical Manifestation: Dr. I B Agung Winaya, SpaBayu SetiaNo ratings yet