Download as pdf or txt
You might also like
- Reading Process Worksheet PalenciaDocument4 pagesReading Process Worksheet PalenciaFranz PalenciaNo ratings yet
- THERMO KING TK 61377-18-MM TKV500 and TKV600 Maintenance Manual Rev. A 01-19Document108 pagesTHERMO KING TK 61377-18-MM TKV500 and TKV600 Maintenance Manual Rev. A 01-19Vincent Marmande100% (1)
- Strategic Change - 2006 - Greener - Managing Change Before Change ManagementDocument8 pagesStrategic Change - 2006 - Greener - Managing Change Before Change ManagementdanaNo ratings yet
- CPQ810Document7 pagesCPQ810Nurhaslina HasNo ratings yet
- Electromagnetic Lab Write-UpDocument5 pagesElectromagnetic Lab Write-Upapi-375748727No ratings yet
- Inspection Checklist 1 - Footing and FoundationDocument4 pagesInspection Checklist 1 - Footing and Foundationthescubatater100% (1)
- Hell Bent: Reading Group GuideDocument5 pagesHell Bent: Reading Group GuideKiran KumarNo ratings yet
- Thesis On Oral Health Related Quality of LifeDocument5 pagesThesis On Oral Health Related Quality of Lifeafknawjof100% (2)
- PIIS1098301518322721Document7 pagesPIIS1098301518322721Francelia Quiñonez RuvalcabaNo ratings yet
- Oral Health Related Quality of Life ThesisDocument5 pagesOral Health Related Quality of Life Thesisb0sus1hyjaf2100% (2)
- QoL Obese ChildrenDocument7 pagesQoL Obese ChildrenLiga Sabatina de BaloncestoNo ratings yet
- Development and Validation of The Greek Version ofDocument9 pagesDevelopment and Validation of The Greek Version ofDimpleNo ratings yet
- Caregivers' Perception of Oral Health Related Quality of Life in A Group of Nigerian Children Living With Human Immunodeficiency VirusDocument7 pagesCaregivers' Perception of Oral Health Related Quality of Life in A Group of Nigerian Children Living With Human Immunodeficiency VirusManelyn GaneNo ratings yet
- Item-Level Analysis of The Relationship Between Orthodontic Treatment Need and Oral Health - Related Quality of Life in Korean SchoolchildrenDocument7 pagesItem-Level Analysis of The Relationship Between Orthodontic Treatment Need and Oral Health - Related Quality of Life in Korean SchoolchildrenMonojit DuttaNo ratings yet
- Impact of Ecc On The Oral Health Related Quality of Life of Preschool Children and Their FamiliesDocument8 pagesImpact of Ecc On The Oral Health Related Quality of Life of Preschool Children and Their FamiliesIJAR JOURNALNo ratings yet
- To What Extent Do Oral Disorders Compromise The Quality of LifeDocument10 pagesTo What Extent Do Oral Disorders Compromise The Quality of LifeAhmad Ulil AlbabNo ratings yet
- Uoi 142 FDocument9 pagesUoi 142 FbkprosthoNo ratings yet
- 2009 - Oral and General Health-Related Quality of Life Among Young PDFDocument6 pages2009 - Oral and General Health-Related Quality of Life Among Young PDFfarrasoyaNo ratings yet
- 2009 - Oral and General Health-Related Quality of Life Among YoungDocument6 pages2009 - Oral and General Health-Related Quality of Life Among YoungfarrasoyaNo ratings yet
- Quality of Life in Children and Adolescents With Osteogenesis Imperfecta: A Qualitative Interview Based StudyDocument9 pagesQuality of Life in Children and Adolescents With Osteogenesis Imperfecta: A Qualitative Interview Based StudyTimothy supitNo ratings yet
- Pediatric Health-Related Quality of Life Measurement Technology: A Guide For Health Care Decision MakersDocument8 pagesPediatric Health-Related Quality of Life Measurement Technology: A Guide For Health Care Decision MakersZeno MunteanuNo ratings yet
- Study Regarding The Correlation Between The Child-OIDP Index and The Dental Status in 12-Year-Old Children From Harsova, Constanta CountyDocument10 pagesStudy Regarding The Correlation Between The Child-OIDP Index and The Dental Status in 12-Year-Old Children From Harsova, Constanta Countydup11No ratings yet
- Oral Health-Related Quality of Life, Sense of Coherence and Dental Anxiety: An Epidemiological Cross-Sectional Study of Middle-Aged WomenDocument6 pagesOral Health-Related Quality of Life, Sense of Coherence and Dental Anxiety: An Epidemiological Cross-Sectional Study of Middle-Aged WomenAlexandru Codrin-IonutNo ratings yet
- Assessment of Changes in Oral Health......Document7 pagesAssessment of Changes in Oral Health......Red DoveNo ratings yet
- NIH Public Access: Promoting Healthy Lifestyles in High School AdolescentsDocument18 pagesNIH Public Access: Promoting Healthy Lifestyles in High School Adolescentsadri90No ratings yet
- Oral Health ChineseDocument9 pagesOral Health ChineseNeagu EmaNo ratings yet
- QV STUDY 2012 Quality of Life of Methilfenidate Treatment - Pin-ChenDocument6 pagesQV STUDY 2012 Quality of Life of Methilfenidate Treatment - Pin-ChenDoniLeiteNo ratings yet
- Health and Quality of Life OutcomesDocument7 pagesHealth and Quality of Life OutcomesvinayakNo ratings yet
- Clinical Pediatrics: Parental Perspectives of Early Childhood CariesDocument10 pagesClinical Pediatrics: Parental Perspectives of Early Childhood CariesBasant ShamsNo ratings yet
- Parent's Views On Factors in Uencing The Dental Health of Trinidadian Preschool ChildrenDocument10 pagesParent's Views On Factors in Uencing The Dental Health of Trinidadian Preschool ChildrenElisabeth FransiskaNo ratings yet
- Gadburyamyot2017 PDFDocument12 pagesGadburyamyot2017 PDFDavid UriosteguiNo ratings yet
- Oral Health-Related Quality of Life of Schoolchildren: Impact of Clinical and Psychosocial VariablesDocument8 pagesOral Health-Related Quality of Life of Schoolchildren: Impact of Clinical and Psychosocial VariablesJuliana MoroNo ratings yet
- Health-Related Quality of Life For Infants in The Neonatal Intensive Care UnitDocument7 pagesHealth-Related Quality of Life For Infants in The Neonatal Intensive Care Unitsri wahyuniNo ratings yet
- ANAK Efek Intervensi Perkembangan AnakDocument8 pagesANAK Efek Intervensi Perkembangan Anaksipen poltekkesbdgNo ratings yet
- Acharya 2009Document6 pagesAcharya 2009miltonlafebreNo ratings yet
- Cejas Et Al. - Quality of Life-CI: Development of An Early Childhood Parent-Proxy & Adolescent VersionDocument28 pagesCejas Et Al. - Quality of Life-CI: Development of An Early Childhood Parent-Proxy & Adolescent VersionPablo VasquezNo ratings yet
- Oral Health-Related Quality of Life Following Dental Treatment Under General Anaesthesia For Early Childhood Caries - A UK-based StudyDocument12 pagesOral Health-Related Quality of Life Following Dental Treatment Under General Anaesthesia For Early Childhood Caries - A UK-based Studynzie76No ratings yet
- Jurnal 3Document10 pagesJurnal 3Alverina Putri RiandaNo ratings yet
- 1 s2.0 S0300571223000921 MainDocument8 pages1 s2.0 S0300571223000921 MainFrancelia Quiñonez RuvalcabaNo ratings yet
- Health and Quality of LifeDocument8 pagesHealth and Quality of LifeRizalMarubobSilalahiNo ratings yet
- El Índice de Postura Del Pie, Prueba de Estocada Del Tobillo La Escala de Beighton y La Evaluación de Las Extremidades Inferiores Puntaje en Niños Sanos: Un Estudio de ConfiabilidadDocument5 pagesEl Índice de Postura Del Pie, Prueba de Estocada Del Tobillo La Escala de Beighton y La Evaluación de Las Extremidades Inferiores Puntaje en Niños Sanos: Un Estudio de ConfiabilidadNairda Teresa Arredondo CruzNo ratings yet
- Organized Physical Activity and Health in Preschool Age: A ReviewDocument8 pagesOrganized Physical Activity and Health in Preschool Age: A ReviewArie AnggaNo ratings yet
- Feeding Guidelines For Infants and Young Toddlers: Nutrition and The LifecycleDocument9 pagesFeeding Guidelines For Infants and Young Toddlers: Nutrition and The LifecycleEssa BagusNo ratings yet
- Jenny Abanto, Georgios Tsakos, Saul Martins Paiva, Thiago S. Carvalho, Daniela P. Raggio and Marcelo BöneckerDocument10 pagesJenny Abanto, Georgios Tsakos, Saul Martins Paiva, Thiago S. Carvalho, Daniela P. Raggio and Marcelo BöneckerTasya AwaliyahNo ratings yet
- Oral Health-Related Quality of Life in Children: Conceptual IssuesDocument5 pagesOral Health-Related Quality of Life in Children: Conceptual IssuesCristian OneaNo ratings yet
- Impact of Orthodontic Treatment On Oral Health-Related Quality of Life in The Slovak Republic: A Cross-Sectional StudyDocument10 pagesImpact of Orthodontic Treatment On Oral Health-Related Quality of Life in The Slovak Republic: A Cross-Sectional StudyKornist BufuNo ratings yet
- Does Growth Stunting Correlate With Oral Health in Children - A Systematic Review - PMCDocument11 pagesDoes Growth Stunting Correlate With Oral Health in Children - A Systematic Review - PMCnadiah khairunnisaNo ratings yet
- Calidad de VidaDocument9 pagesCalidad de VidaS bmNo ratings yet
- Caregiving InterventionsDocument134 pagesCaregiving InterventionsAlejandro LozanoNo ratings yet
- Subjective Health Literacy: Development of A Brief Instrument For School-Aged ChildrenDocument7 pagesSubjective Health Literacy: Development of A Brief Instrument For School-Aged ChildrenAprilia FransiskaNo ratings yet
- (Claudine Fox, Carol Joughin) Childhood-Onset EatiDocument96 pages(Claudine Fox, Carol Joughin) Childhood-Onset EatiAlma AtaNo ratings yet
- 35-Article Text-123-1-10-20210127Document9 pages35-Article Text-123-1-10-20210127Hariharan HemarajanNo ratings yet
- tmp1F38 TMPDocument6 pagestmp1F38 TMPFrontiersNo ratings yet
- Oke 2Document4 pagesOke 2Muthi'ah Ramadhani AgusNo ratings yet
- A Socio-Ecological Approach To Physical Activity Interventions in Childcare: A Systematic ReviewDocument12 pagesA Socio-Ecological Approach To Physical Activity Interventions in Childcare: A Systematic Reviewfadila azzahraNo ratings yet
- Feeding ArvedsonDocument10 pagesFeeding ArvedsonPablo Oyarzún Dubó100% (1)
- Relationship Between Perception of Oral Health, Clinical Conditions and Socio-Behavioral Factors of Mother-ChildDocument9 pagesRelationship Between Perception of Oral Health, Clinical Conditions and Socio-Behavioral Factors of Mother-ChildhalidadwiNo ratings yet
- Relationship Between Obesity and Health-Related Quality of Life in Children Aged 7 - 8 YearsDocument8 pagesRelationship Between Obesity and Health-Related Quality of Life in Children Aged 7 - 8 YearsDamjan JaksicNo ratings yet
- Cousson Et Al 2012 GerodontologyDocument8 pagesCousson Et Al 2012 Gerodontologywiena aviolitaNo ratings yet
- Health LiteracyDocument12 pagesHealth LiteracyTengiz VerulavaNo ratings yet
- 2251 6581 13 32 PDFDocument10 pages2251 6581 13 32 PDFAlexandraNo ratings yet
- ID Hubungan Status Spiritual Dengan KualitaDocument3 pagesID Hubungan Status Spiritual Dengan KualitaRetno Anggraini100% (1)
- International Journal of Pediatric Otorhinolaryngology: Lindsey Edwards, Tina Hill, Merle MahonDocument7 pagesInternational Journal of Pediatric Otorhinolaryngology: Lindsey Edwards, Tina Hill, Merle MahonNina JNo ratings yet
- Impact of Periodontal Health On The Quality of Life Among DiabeticsDocument6 pagesImpact of Periodontal Health On The Quality of Life Among DiabeticsVembri IrawatiNo ratings yet
- Therapist's Guide to Pediatric Affect and Behavior RegulationFrom EverandTherapist's Guide to Pediatric Affect and Behavior RegulationNo ratings yet
- CambraDocument6 pagesCambraShahid ShaikhNo ratings yet
- GDFGDocument5 pagesGDFGShahid ShaikhNo ratings yet
- 4Document13 pages4Shahid ShaikhNo ratings yet
- Role of Rac1-Pak Pathway in Aggressive B-Cell LymphomaDocument169 pagesRole of Rac1-Pak Pathway in Aggressive B-Cell LymphomaShahid ShaikhNo ratings yet
- Brochure IDC2017Document16 pagesBrochure IDC2017Shahid ShaikhNo ratings yet
- Sea Breeze Template: Your NameDocument9 pagesSea Breeze Template: Your NameShahid ShaikhNo ratings yet
- Pulp Therapy in Pediatric Dentistry RevisedDocument47 pagesPulp Therapy in Pediatric Dentistry RevisedShahid Shaikh100% (2)
- Comparative Evaluation of The Effect of Different Root Canal Preparation Techniques in Primary Teeth Using CBCT"Document22 pagesComparative Evaluation of The Effect of Different Root Canal Preparation Techniques in Primary Teeth Using CBCT"Shahid ShaikhNo ratings yet
- Crowns Used in Pediatric DentistrDocument85 pagesCrowns Used in Pediatric DentistrShahid Shaikh100% (1)
- Bruxism and Its TreatmentDocument22 pagesBruxism and Its TreatmentShahid ShaikhNo ratings yet
- DzireDocument324 pagesDzireDaniel Lopez VenancioNo ratings yet
- Product Characteristics and ClassificationsDocument3 pagesProduct Characteristics and Classificationstsega-alemNo ratings yet
- SONET - SDH OC192 - STM64 PICs With XFP (T4000 Router) - Sonet SDH Support - Juniper NetworksDocument4 pagesSONET - SDH OC192 - STM64 PICs With XFP (T4000 Router) - Sonet SDH Support - Juniper NetworksDhanyasriNo ratings yet
- 2volt Powerstack BatteriesDocument4 pages2volt Powerstack BatteriesYasirNo ratings yet
- Belzona 5111 Product Data SheetDocument2 pagesBelzona 5111 Product Data SheetPeter RhoadsNo ratings yet
- GloverDocument272 pagesGlovermidialaoropesaNo ratings yet
- Week 5 Spain & The ReconquistaDocument6 pagesWeek 5 Spain & The ReconquistaABigRedMonsterNo ratings yet
- In Company 3.0 Intermediate in Action Video Worksheet - Scenario Worksheet CDocument2 pagesIn Company 3.0 Intermediate in Action Video Worksheet - Scenario Worksheet CAma GavNo ratings yet
- FBFP UserGuide 2 21Document88 pagesFBFP UserGuide 2 21Zlatko OžanićNo ratings yet
- IVF STUDY For Case StudyDocument3 pagesIVF STUDY For Case StudygremlinnakuNo ratings yet
- 50 HaazinuDocument6 pages50 HaazinuTheodore James TurnerNo ratings yet
- What Is The Difference Between Cement and Concrete?Document26 pagesWhat Is The Difference Between Cement and Concrete?Al-Buruj InstituteNo ratings yet
- Cultural Variations and Social Differences (Ethnicity)Document19 pagesCultural Variations and Social Differences (Ethnicity)Jomar TeofiloNo ratings yet
- Journaling PDFDocument1 pageJournaling PDFMargarita Maria Botero PerezNo ratings yet
- Formulas To Know For Exam PDocument4 pagesFormulas To Know For Exam Pkevin.nguyen268998No ratings yet
- Road Slope Protection and Flood Control Pow Template Rev. 9Document183 pagesRoad Slope Protection and Flood Control Pow Template Rev. 9Christian Jahweh Sarvida SabadoNo ratings yet
- Forecasting ExamplesDocument14 pagesForecasting ExamplesJudith DelRosario De RoxasNo ratings yet
- DR Himanshu Gaur: Consultant Orthopaedic, Joint Replacement & Arthroscopy (Sports Injury) Surgeon BCIMS, New DelhiDocument34 pagesDR Himanshu Gaur: Consultant Orthopaedic, Joint Replacement & Arthroscopy (Sports Injury) Surgeon BCIMS, New DelhiAnjani Kumar JhaNo ratings yet
- VFR 800Document159 pagesVFR 800christian maritzNo ratings yet
- Porter's Five Forces Model of Competition-1Document14 pagesPorter's Five Forces Model of Competition-1Kanika RustagiNo ratings yet
- Abnormal Uterine BleedingDocument11 pagesAbnormal Uterine BleedingKIPA SHRESTHANo ratings yet
- Catalogo BujesDocument120 pagesCatalogo BujesJason BurtonNo ratings yet
- TLC Online Learning Pack ContentDocument15 pagesTLC Online Learning Pack ContentjennoNo ratings yet
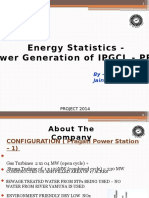
- Energy Statistics - Power Generation of IPGCL - PPCL: by - Aditi JainDocument16 pagesEnergy Statistics - Power Generation of IPGCL - PPCL: by - Aditi JainknochoutNo ratings yet