Download as pdf or txt
You might also like
- Osteopathic and Chiropractic Techniques PDFDocument298 pagesOsteopathic and Chiropractic Techniques PDFupender yadav96% (26)
- Conners Rating Scale For Parents Revised LDocument3 pagesConners Rating Scale For Parents Revised LNorhafizah AhmadNo ratings yet
- C Post Concussion ChecklistDocument1 pageC Post Concussion Checklistalston96No ratings yet
- CBI-R Cambridge Behavioural InventoryDocument2 pagesCBI-R Cambridge Behavioural InventoryNikos AndronasNo ratings yet
- Symptom Checklist 90-R: Please Enter Only ONE. For The Past Week, How Much Were You Bothered byDocument4 pagesSymptom Checklist 90-R: Please Enter Only ONE. For The Past Week, How Much Were You Bothered byanon_289647426100% (1)
- Wender Utah Rating ScaleDocument3 pagesWender Utah Rating ScaleGabyNoriegaNo ratings yet
- Gonstead Chiropractic MethodsDocument3 pagesGonstead Chiropractic MethodsJennifer0% (1)
- Metabolic-Assessment-Form FullDocument6 pagesMetabolic-Assessment-Form FullOlesiaNo ratings yet
- OFFICE FORMS Hypoglycemia QuestionnaireDocument1 pageOFFICE FORMS Hypoglycemia QuestionnairelawsonbradNo ratings yet
- Smgebhnaf34082013 Fill ReaderDocument2 pagesSmgebhnaf34082013 Fill Readerapi-240397215No ratings yet
- Hypoglycemia QuestionnaireDocument1 pageHypoglycemia QuestionnairelawsonbradNo ratings yet
- CHVStest 20141516Document2 pagesCHVStest 20141516dabidnavarroNo ratings yet
- Neurotransmitter Assessment Form AE260Document3 pagesNeurotransmitter Assessment Form AE260OlesiaNo ratings yet
- IPOS Renal Paciente - SemanaDocument2 pagesIPOS Renal Paciente - SemanaUNEME HEMODIALISISNo ratings yet
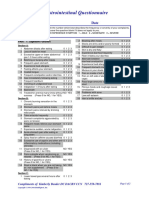
- Gastrointestional QuestionnaireDocument2 pagesGastrointestional QuestionnaireEva SabillaNo ratings yet
- Digestion AssessmentDocument6 pagesDigestion AssessmentElisa ValdésNo ratings yet
- Sleep TestingDocument1 pageSleep TestingTroy O'BrienNo ratings yet
- Ullanlinna Narcolepsy ScaleDocument1 pageUllanlinna Narcolepsy Scalehcrislopes5617No ratings yet
- EAT 26TestScoringKey 11 1 17Document1 pageEAT 26TestScoringKey 11 1 17Sabrina Braga Castanheira da CostaNo ratings yet
- Questionnaire For ClientDocument4 pagesQuestionnaire For Clientzhaoyuanzhe112No ratings yet
- Eating DisordersDocument3 pagesEating DisordersNo OneNo ratings yet
- HormoneSelfTest 1 1Document4 pagesHormoneSelfTest 1 1Yo DraNo ratings yet
- Eating Attitudes TestDocument2 pagesEating Attitudes Testvunnati04No ratings yet
- Conners Rating Scale For Parents Revised L ExampleDocument3 pagesConners Rating Scale For Parents Revised L ExamplesirinyamdNo ratings yet
- Anxiety Scale: Dr. Reneé Roberts, PsychologistDocument3 pagesAnxiety Scale: Dr. Reneé Roberts, Psychologistpreeti vermaNo ratings yet
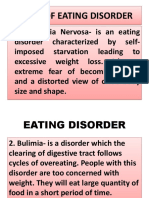
- Kinds of Eating Disorder PPDocument10 pagesKinds of Eating Disorder PPfelitaNo ratings yet
- The Burns Depression ChecklistDocument2 pagesThe Burns Depression Checklistim247black50% (2)
- NR 17 - Excessive Fatigue Symptom InventoryDocument2 pagesNR 17 - Excessive Fatigue Symptom InventoryCPSSTNo ratings yet
- CNS Symptom Check List 100: (E.g., Homework, Chores, Paperwork, Etc.)Document3 pagesCNS Symptom Check List 100: (E.g., Homework, Chores, Paperwork, Etc.)Nadhirah RahimNo ratings yet
- Endocrine ConditionsDocument5 pagesEndocrine ConditionsGlen DizonNo ratings yet
- PHQ 9Document1 pagePHQ 9adiithao93No ratings yet
- Ryshelle Piamonte Bsed-Eng2-2Document7 pagesRyshelle Piamonte Bsed-Eng2-2RYSHELLE PIAMONTENo ratings yet
- Survey Questionnaire Dry Run Humss Respondent:15 Sex:Male-7 Female-8 Seldom-1 Occasionally-3 Often-5 Always-6Document3 pagesSurvey Questionnaire Dry Run Humss Respondent:15 Sex:Male-7 Female-8 Seldom-1 Occasionally-3 Often-5 Always-6Banana RamaNo ratings yet
- Diabetes PresentationDocument20 pagesDiabetes PresentationSondang Margaret L. TobingNo ratings yet
- DrRitamarie FunctionalDigestiveScorecard PDFDocument8 pagesDrRitamarie FunctionalDigestiveScorecard PDFsaipujitha1996100% (1)
- Eating Attitudes Test 26 EAT 26 Scoring Calculator OnlineDocument4 pagesEating Attitudes Test 26 EAT 26 Scoring Calculator Onlinevunnati04No ratings yet
- Systems Survey Form: Group 1Document4 pagesSystems Survey Form: Group 1Chris EshlemanNo ratings yet
- Anorexia Nervosa and Anorexia BulimiaDocument3 pagesAnorexia Nervosa and Anorexia Bulimiainsta aNo ratings yet
- Sleep InterviewDocument4 pagesSleep InterviewFatemah BeygNo ratings yet
- Assignment PsychologyDocument23 pagesAssignment Psychologythivyaashini SellaNo ratings yet
- Questionnaires (BAI, BDI II, PSS, QLESDocument6 pagesQuestionnaires (BAI, BDI II, PSS, QLESJasleen KaurNo ratings yet
- Questionnaire Document PDFDocument1 pageQuestionnaire Document PDFWanpis PhotographyNo ratings yet
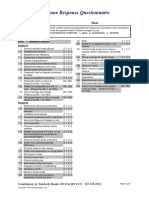
- Immune Response Questionnaire: Name DateDocument2 pagesImmune Response Questionnaire: Name DateSPE CommitteeNo ratings yet
- PHQ and GAD One Page - FillableDocument1 pagePHQ and GAD One Page - Fillablelisa stewartNo ratings yet
- Eating DisordersDocument15 pagesEating DisordersЯ мусурманNo ratings yet
- Wender Utah Adult ADHD ScaleDocument3 pagesWender Utah Adult ADHD ScaleBharatNo ratings yet
- Breathing TAI - NijmegenFormDocument1 pageBreathing TAI - NijmegenFormLynseyNo ratings yet
- Electronic Supplementary MaterialDocument4 pagesElectronic Supplementary MaterialVirgíniaVitalinaNo ratings yet
- Ibs QolDocument3 pagesIbs QolsamuelNo ratings yet
- Eating DisordersDocument23 pagesEating Disordersipilham001No ratings yet
- Pdf-Eating-Disorders Finals PDFDocument6 pagesPdf-Eating-Disorders Finals PDFVictor MurilloNo ratings yet
- Trauma Symptons ChecklistDocument7 pagesTrauma Symptons Checklistmnktcp2sc5No ratings yet
- Eat-26 Assessment FormDocument3 pagesEat-26 Assessment FormJAY MOMENTNo ratings yet
- Eating Habits, Sleep & Stress ManagementDocument22 pagesEating Habits, Sleep & Stress ManagementAnnabelle Grace Carreon PerezNo ratings yet
- Signalenkaart Buro PUUR MOOC 2017 en GoedDocument1 pageSignalenkaart Buro PUUR MOOC 2017 en GoedLeo RamirezNo ratings yet
- PHQ-9 and GAD-7 Form - ADocument1 pagePHQ-9 and GAD-7 Form - AIrving MaldonadoNo ratings yet
- Perinatal Anxiety Screening Scale (PASS)Document4 pagesPerinatal Anxiety Screening Scale (PASS)sri wahyuni100% (1)
- Health Appraisal QuestionnaireDocument5 pagesHealth Appraisal QuestionnaireSteveNo ratings yet
- FDI Child and ParentDocument2 pagesFDI Child and ParentOg DoogyNo ratings yet
- Domain 4Document49 pagesDomain 4Ayu KrisNo ratings yet
- Best Practicesfor Specimen CollectionDocument2 pagesBest Practicesfor Specimen CollectionOlesiaNo ratings yet
- Essence Tri FoldDocument6 pagesEssence Tri FoldOlesiaNo ratings yet
- Metabolic Assessment Form Nutritional Key 022515 Version 2Document4 pagesMetabolic Assessment Form Nutritional Key 022515 Version 2OlesiaNo ratings yet
- Neurotransmitter Assessment Form AE260Document3 pagesNeurotransmitter Assessment Form AE260OlesiaNo ratings yet
- Emerging Glucose-Lowering Therapies A GuideDocument6 pagesEmerging Glucose-Lowering Therapies A GuideOlesiaNo ratings yet
- The Gut: A Key To The Pathogenesis of Type 2 Diabetes?: ReviewDocument4 pagesThe Gut: A Key To The Pathogenesis of Type 2 Diabetes?: ReviewOlesiaNo ratings yet
- MonacoReport - AnnalsofGlobalHealthReport Complete Nov16 FINALDocument93 pagesMonacoReport - AnnalsofGlobalHealthReport Complete Nov16 FINALOlesiaNo ratings yet
- Timing of Insulin Injections Adherence and GlycemiDocument12 pagesTiming of Insulin Injections Adherence and GlycemiOlesiaNo ratings yet
- Quercetin - HealthDocument5 pagesQuercetin - HealthOlesiaNo ratings yet
- Unit 14: Physiological Disorders The Research Guide: NameDocument16 pagesUnit 14: Physiological Disorders The Research Guide: NameOlesiaNo ratings yet
- Appropriate Titration of Basal Insulin in Type 2 Diabetes and The Potential Role of The PharmacistDocument21 pagesAppropriate Titration of Basal Insulin in Type 2 Diabetes and The Potential Role of The PharmacistOlesiaNo ratings yet
- A Review of Torque Release Technique®Document5 pagesA Review of Torque Release Technique®Ed RibeiroNo ratings yet
- Graston TechniqueDocument8 pagesGraston TechniqueSvetlana PolyakovaNo ratings yet
- Onsent To Hiropractic Reatment: BenefitsDocument2 pagesOnsent To Hiropractic Reatment: BenefitsRajender BishtNo ratings yet
- Certification in Chiropractic Techniques: Legitimate Care or Tomfoolery? Sam HomolaDocument9 pagesCertification in Chiropractic Techniques: Legitimate Care or Tomfoolery? Sam HomolaAlejandro LópezNo ratings yet
- Forces of Commonly Used Chiropractic Techniques For Children: A Review of The LiteratureDocument10 pagesForces of Commonly Used Chiropractic Techniques For Children: A Review of The LiteratureAlejandro LópezNo ratings yet
- Toggle RecoilDocument7 pagesToggle RecoilEduardo OlivaNo ratings yet
- Sacro Occipital Technique: Update 2003Document45 pagesSacro Occipital Technique: Update 2003Edgardo BivimasNo ratings yet
- Welcome To FIT CHIROPRACTIC and Wellness CenterDocument38 pagesWelcome To FIT CHIROPRACTIC and Wellness CenterKemberly Semaña PentonNo ratings yet
- Klinik For Manuel Medicin05bDocument4 pagesKlinik For Manuel Medicin05bFerris BuhlerNo ratings yet
- GlossaryDocument120 pagesGlossarynlesevNo ratings yet
- Comparison of Compressive Myofascial Release and The Graston Technique For Improving Ankle-Dorsiflexion Range of MotionDocument8 pagesComparison of Compressive Myofascial Release and The Graston Technique For Improving Ankle-Dorsiflexion Range of MotionHevin GokulNo ratings yet
- Gonstead Chiropractic Technique GCT PDFDocument9 pagesGonstead Chiropractic Technique GCT PDFАртем СтепанецNo ratings yet
- Flip Class Reflection 1Document3 pagesFlip Class Reflection 1api-301784889No ratings yet
- Adjunctive TherapyDocument5 pagesAdjunctive Therapyromeojr100% (1)
- Technique in The Classroom at Palmer College of CHDocument13 pagesTechnique in The Classroom at Palmer College of CH呂桂村No ratings yet
- Chiropractic Treatment Techniques-2016Document9 pagesChiropractic Treatment Techniques-2016Dr. Mateen ShaikhNo ratings yet
- Chiropractic IntroductionDocument17 pagesChiropractic IntroductionDr. Krishna N. Sharma100% (1)
- Chiropractic Philosophy Art Science Support Integrating Orthopedic NeurologyDocument5 pagesChiropractic Philosophy Art Science Support Integrating Orthopedic NeurologyDenise MathreNo ratings yet
- (ART. 5 PP DEPORTE) Tratamiento de Terapia Manual para La Escoliosis Idiopática AdolescenteDocument5 pages(ART. 5 PP DEPORTE) Tratamiento de Terapia Manual para La Escoliosis Idiopática AdolescenteSofia PaezNo ratings yet
- Instrument Assisted Soft Tissue MobilizationDocument5 pagesInstrument Assisted Soft Tissue MobilizationJordan QuillNo ratings yet
- A Review of Chiropractic Care in WomensDocument4 pagesA Review of Chiropractic Care in Womensyulinda aswanNo ratings yet
- User ManualDocument21 pagesUser ManualClecio BrandãoNo ratings yet
- How To Avoid Back Pain PDFDocument13 pagesHow To Avoid Back Pain PDFHugo AzzolinaNo ratings yet