
Clasifications of Mandibular Fractures-Review
Clasifications of Mandibular Fractures-Review
You might also like
- Speakout 3rd B2+ Workbook With KeysDocument94 pagesSpeakout 3rd B2+ Workbook With KeysКатя ДмитриеваNo ratings yet
- Haresh BiodataDocument2 pagesHaresh Biodataharesh_ahir200063% (30)
- Mandible Fracture AO CMFDocument16 pagesMandible Fracture AO CMFREM biusNo ratings yet
- FLOSA ClsificationDocument3 pagesFLOSA ClsificationMatin Ahmad KhanNo ratings yet
- Classification of Malocclusion Revisited 2016Document7 pagesClassification of Malocclusion Revisited 2016Dharampal SinghNo ratings yet
- Art-11-Mageet Malocclusion ClassifictnDocument7 pagesArt-11-Mageet Malocclusion ClassifictnDharampal SinghNo ratings yet
- 6StomEduJArt Mageet AODec2016Document8 pages6StomEduJArt Mageet AODec2016Zulfiani SyachbaniahNo ratings yet
- Orthodontics Classification of Skeletal PDFDocument7 pagesOrthodontics Classification of Skeletal PDFPriyank RaiNo ratings yet
- Classification of Skeletal and Dental Malocclusion: RevisitedDocument8 pagesClassification of Skeletal and Dental Malocclusion: RevisitedRajkumar CouppoussamyNo ratings yet
- Adil Osman MageetDocument8 pagesAdil Osman MageetnadiaNo ratings yet
- Classification of Skeletal and Dental Malocclusion: RevisitedDocument8 pagesClassification of Skeletal and Dental Malocclusion: RevisitedGladys SakurakoNo ratings yet
- Classification of Skeletal and Dental Malocclusion: RevisitedDocument8 pagesClassification of Skeletal and Dental Malocclusion: RevisitedDiba Eka DiputriNo ratings yet
- Classification of Skeletal and Dental Malocclusion: RevisitedDocument8 pagesClassification of Skeletal and Dental Malocclusion: RevisitedIoana LazarNo ratings yet
- Classification of MalocclusionDocument8 pagesClassification of MalocclusionDevata RaviNo ratings yet
- Oral Surgery - Dr. Labeed SamiDocument22 pagesOral Surgery - Dr. Labeed SamiMohammed TarekNo ratings yet
- Copy1-Fraktur Mandibula (Edit)Document25 pagesCopy1-Fraktur Mandibula (Edit)debby nirmasariNo ratings yet
- Classification of Manfibular FractureDocument16 pagesClassification of Manfibular FractureFaheem AhmedNo ratings yet
- Anatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsDocument24 pagesAnatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsAlvaro Jose Uribe TamaraNo ratings yet
- Correcting The Class II Subdivision MalocclusionDocument2 pagesCorrecting The Class II Subdivision MalocclusionplsssssNo ratings yet
- Comparison of Orthodontic Techniques Used ForDocument5 pagesComparison of Orthodontic Techniques Used ForAdina SerbanNo ratings yet
- "Unilateral Subcondylar Fracture Treated by Close Reduction: A CaseDocument3 pages"Unilateral Subcondylar Fracture Treated by Close Reduction: A CaseAlbertine JaneNo ratings yet
- Craniofacial Deformities Review of Etiologies Distribution and TDocument16 pagesCraniofacial Deformities Review of Etiologies Distribution and TambersNo ratings yet
- Management of Class 3 MalocclusionDocument8 pagesManagement of Class 3 MalocclusionAkhil SinghNo ratings yet
- Review Artilces Annals and Essences of DentistryDocument14 pagesReview Artilces Annals and Essences of DentistryRahul Kumar DiwakarNo ratings yet
- CCD 9 342Document5 pagesCCD 9 342Anonymous 9PcFdakHcNo ratings yet
- Ge 2016Document9 pagesGe 2016Amani AouameurNo ratings yet
- Doraczynska Kowalik2017Document9 pagesDoraczynska Kowalik2017mahaaNo ratings yet
- Jurnal Asli JR Radiologi - Unusual Giant Complex Odontoma A Case ReportDocument4 pagesJurnal Asli JR Radiologi - Unusual Giant Complex Odontoma A Case ReportAliaNo ratings yet
- Orthodontic Camouflage in Skeletal Class III Malocclusion A Contemporary ReviewDocument5 pagesOrthodontic Camouflage in Skeletal Class III Malocclusion A Contemporary ReviewNatasha Ank100% (1)
- Classification Systems For Orofacial Clefts: 10.5005/jp-Journals-10037-1035Document5 pagesClassification Systems For Orofacial Clefts: 10.5005/jp-Journals-10037-1035assususuNo ratings yet
- Cleft Lip and Palate An Evidence Based Review PDFDocument16 pagesCleft Lip and Palate An Evidence Based Review PDFariskaNo ratings yet
- Surgical Management of Complex Mandibular Fracture: Case ReportDocument5 pagesSurgical Management of Complex Mandibular Fracture: Case ReportlindaNo ratings yet
- The Cleft-Columellar Angle A Useful Variable To deDocument7 pagesThe Cleft-Columellar Angle A Useful Variable To deaprilandralekaNo ratings yet
- Open Bite, A Review of Etiology and Manageme PDFDocument8 pagesOpen Bite, A Review of Etiology and Manageme PDFVieussens JoffreyNo ratings yet
- Mutifocal FracturesDocument4 pagesMutifocal FracturesElmer NarvaezNo ratings yet
- A To Z Orthodontics. Volume 19: Craniofacial Deformity: January 2011Document18 pagesA To Z Orthodontics. Volume 19: Craniofacial Deformity: January 2011MD MAHMUDUL HASAN NAEEMNo ratings yet
- Trauma Q&ADocument8 pagesTrauma Q&ANoor MaxeemNo ratings yet
- Fixed Functional Appliances For Treatment of Class II Malocclusions Effects and LimitationsDocument35 pagesFixed Functional Appliances For Treatment of Class II Malocclusions Effects and LimitationsAya ElsayedNo ratings yet
- Management of Lefort Fractures: Vijay Ebenezer, R. Balakrishnan and Anatha PadmanabhanDocument4 pagesManagement of Lefort Fractures: Vijay Ebenezer, R. Balakrishnan and Anatha PadmanabhanSuci NourmalizaNo ratings yet
- Broadie 2Document12 pagesBroadie 2Stefana NanuNo ratings yet
- LISCHER, B.E. The diagnosis of malocclusion. Dent. Cosmos 53412-22,1911.Document16 pagesLISCHER, B.E. The diagnosis of malocclusion. Dent. Cosmos 53412-22,1911.abigail.piresNo ratings yet
- Mandibular Condylar and Subcondylar Fractures PDFDocument16 pagesMandibular Condylar and Subcondylar Fractures PDFWayan Sutresna YasaNo ratings yet
- Classification of MalDocument7 pagesClassification of MalWeiliem AbubakarNo ratings yet
- Microssomia Ajodo 2014 PDFDocument16 pagesMicrossomia Ajodo 2014 PDFFabiane AzeredoNo ratings yet
- Class IIIElastics 2010Document11 pagesClass IIIElastics 2010febriNo ratings yet
- Cystic Lesions of MandibleDocument18 pagesCystic Lesions of MandibleRahul ShindeNo ratings yet
- Maxillofacial Defects and Their Classification: A Review.: ArticleDocument7 pagesMaxillofacial Defects and Their Classification: A Review.: ArticleVivek ShankarNo ratings yet
- Janson2010 PDFDocument10 pagesJanson2010 PDFMonojit DuttaNo ratings yet
- Class II - DD and MX PDFDocument14 pagesClass II - DD and MX PDFserahNo ratings yet
- 2016 SergioDocument10 pages2016 SergioazizhamoudNo ratings yet
- Sas 15 Den 032Document19 pagesSas 15 Den 032Alexa De GuzmanNo ratings yet
- Radiology of Cleft Lip and Palate: Imaging For The Prenatal Period and Throughout LifeDocument12 pagesRadiology of Cleft Lip and Palate: Imaging For The Prenatal Period and Throughout LifeAmeria Briliana ShoumiNo ratings yet
- How To Evaluate Dental Cavities in Horses: Stephen S. Galloway, DVMDocument8 pagesHow To Evaluate Dental Cavities in Horses: Stephen S. Galloway, DVMReza ChandraNo ratings yet
- Borderline Class III Patient and Treatment Options A Comprehensive Review PDFDocument3 pagesBorderline Class III Patient and Treatment Options A Comprehensive Review PDFOsama MohamedNo ratings yet
- Maxillofacial (Midface) FracturesDocument16 pagesMaxillofacial (Midface) FracturesYeraldin EspañaNo ratings yet
- 2215 3411 Odovtos 20 02 31Document7 pages2215 3411 Odovtos 20 02 31habeebNo ratings yet
- Class II Malocclusions Diagnostic and Clinical Considerations With and Without Treatment. Seminars in Orthodontics 12 (1) 11-24, Mar 2006. S. BisharaDocument14 pagesClass II Malocclusions Diagnostic and Clinical Considerations With and Without Treatment. Seminars in Orthodontics 12 (1) 11-24, Mar 2006. S. BisharaAhmad EgbariaNo ratings yet
- The Relationship Between Cranial Base Angle and Various Malocclusion TypesDocument5 pagesThe Relationship Between Cranial Base Angle and Various Malocclusion TypesAlvaro ChacónNo ratings yet
- 2015 Cleft Lip and Palate An Evidence-Based ReviewDocument16 pages2015 Cleft Lip and Palate An Evidence-Based ReviewDimitris RodriguezNo ratings yet
- 1 s2.0 S0929664609602643 MainDocument10 pages1 s2.0 S0929664609602643 MainCrisu CrisuuNo ratings yet
- Mahakal Institute of Pharamaceutical Studies, UjjainDocument8 pagesMahakal Institute of Pharamaceutical Studies, UjjainsafiyaNo ratings yet
- Safety Data Sheet: Revision Date: 15/06/2012 According To (EC) No. 1907/2006 (REACH), Annex II - United Kingdom (UK)Document8 pagesSafety Data Sheet: Revision Date: 15/06/2012 According To (EC) No. 1907/2006 (REACH), Annex II - United Kingdom (UK)AmirmasoudNo ratings yet
- Unit 2 - Role of Social Worker in Health FieldDocument10 pagesUnit 2 - Role of Social Worker in Health FieldDharek IleshNo ratings yet
- Temidayo Osunronbi Himanshu Sharma: Original Article - Spine - CordDocument10 pagesTemidayo Osunronbi Himanshu Sharma: Original Article - Spine - CordnulintavaNo ratings yet
- BDSM Experiences, Relationships, and Scenes in Southern DominantsDocument198 pagesBDSM Experiences, Relationships, and Scenes in Southern DominantsYvonne Yap Ying YingNo ratings yet
- A 33-Year-Old Woman With Trichoptysis, Diagnosed With Infiltrative Mature Mediastinal Teratoma: A Case ReportDocument15 pagesA 33-Year-Old Woman With Trichoptysis, Diagnosed With Infiltrative Mature Mediastinal Teratoma: A Case ReportElok NurfaiqohNo ratings yet
- NSTP FeatureDocument2 pagesNSTP FeatureCharisseNo ratings yet
- Alison Morton-Cooper Health Care and The Autism Spectrum A Guide For Health Professionals, Parents and Carers 2004Document130 pagesAlison Morton-Cooper Health Care and The Autism Spectrum A Guide For Health Professionals, Parents and Carers 2004lillouana100% (1)
- Vamana Karma-Understanding Mode of ActionDocument12 pagesVamana Karma-Understanding Mode of ActionsmsmastiNo ratings yet
- Health 7 LAS Quarter 3 1 1Document62 pagesHealth 7 LAS Quarter 3 1 1raymart zalunNo ratings yet
- CS2 Booklet 7 (Mortality Projection) 2019 FINALDocument38 pagesCS2 Booklet 7 (Mortality Projection) 2019 FINALAnsh ParmarNo ratings yet
- BioavailabilityDocument15 pagesBioavailabilitywriter noreenNo ratings yet
- Pe 8 Q1 W1-8-Module-2023Document59 pagesPe 8 Q1 W1-8-Module-2023Arianne B. CabañezNo ratings yet
- Section 1 - Chemical Product and Company Information: Safety Data Sheet - Sulfur Hexafluoride (SF)Document8 pagesSection 1 - Chemical Product and Company Information: Safety Data Sheet - Sulfur Hexafluoride (SF)sufizamaniNo ratings yet
- Module 3 - SociologyDocument74 pagesModule 3 - SociologyakshayaNo ratings yet
- Chromium, Hexavalent, Method 8023, 02-2009, 9th EdDocument6 pagesChromium, Hexavalent, Method 8023, 02-2009, 9th EdTicha MaharaniNo ratings yet
- Nutrition Therapy For Adults With Diabetes or Prediabetes A Consensus Report - 2019 PDFDocument24 pagesNutrition Therapy For Adults With Diabetes or Prediabetes A Consensus Report - 2019 PDFNicolás Di SantoroNo ratings yet
- Comparison of The Solubilization Effect of Micronized PoloxamersDocument1 pageComparison of The Solubilization Effect of Micronized Poloxamerssaeedazadi1352No ratings yet
- GASTROINTESTINALDocument8 pagesGASTROINTESTINALrheantiffany0815No ratings yet
- Risk For Impaired Skin IntegrityDocument4 pagesRisk For Impaired Skin IntegrityArelys Rodriguez100% (2)
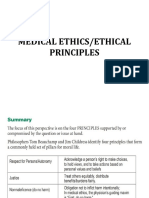
- Medical Ethics/Ethical PrinciplesDocument20 pagesMedical Ethics/Ethical PrinciplesPALATTAO, AUBRIE L. BSMT2-8No ratings yet
- Exam 4th GradingDocument8 pagesExam 4th Gradingedward surtido100% (1)
- Hci Report Group3Document15 pagesHci Report Group3api-302906387No ratings yet
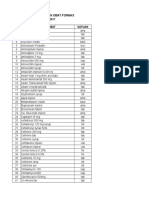
- Daftar Formulariumobat SementaraDocument26 pagesDaftar Formulariumobat SementarafarmasiNo ratings yet
- Descriptive Questions Asked in Previous Years IBPS PO Mains ExamDocument5 pagesDescriptive Questions Asked in Previous Years IBPS PO Mains ExamAnwesha SahooNo ratings yet
- 2007ccj Research EssayDocument10 pages2007ccj Research EssayGeorgie FriedrichsNo ratings yet
- ALT GPT (IFCC) Single Vial: BiolaboDocument2 pagesALT GPT (IFCC) Single Vial: Biolabowindy ajengNo ratings yet
- Aldridge A Short Introduction To CounsellingDocument22 pagesAldridge A Short Introduction To Counsellingbyron chieNo ratings yet
























































































Download as pdf or txt
You might also like
- Speakout 3rd B2+ Workbook With KeysDocument94 pagesSpeakout 3rd B2+ Workbook With KeysКатя ДмитриеваNo ratings yet
- Haresh BiodataDocument2 pagesHaresh Biodataharesh_ahir200063% (30)
- Mandible Fracture AO CMFDocument16 pagesMandible Fracture AO CMFREM biusNo ratings yet
- FLOSA ClsificationDocument3 pagesFLOSA ClsificationMatin Ahmad KhanNo ratings yet
- Classification of Malocclusion Revisited 2016Document7 pagesClassification of Malocclusion Revisited 2016Dharampal SinghNo ratings yet
- Art-11-Mageet Malocclusion ClassifictnDocument7 pagesArt-11-Mageet Malocclusion ClassifictnDharampal SinghNo ratings yet
- 6StomEduJArt Mageet AODec2016Document8 pages6StomEduJArt Mageet AODec2016Zulfiani SyachbaniahNo ratings yet
- Orthodontics Classification of Skeletal PDFDocument7 pagesOrthodontics Classification of Skeletal PDFPriyank RaiNo ratings yet
- Classification of Skeletal and Dental Malocclusion: RevisitedDocument8 pagesClassification of Skeletal and Dental Malocclusion: RevisitedRajkumar CouppoussamyNo ratings yet
- Adil Osman MageetDocument8 pagesAdil Osman MageetnadiaNo ratings yet
- Classification of Skeletal and Dental Malocclusion: RevisitedDocument8 pagesClassification of Skeletal and Dental Malocclusion: RevisitedGladys SakurakoNo ratings yet
- Classification of Skeletal and Dental Malocclusion: RevisitedDocument8 pagesClassification of Skeletal and Dental Malocclusion: RevisitedDiba Eka DiputriNo ratings yet
- Classification of Skeletal and Dental Malocclusion: RevisitedDocument8 pagesClassification of Skeletal and Dental Malocclusion: RevisitedIoana LazarNo ratings yet
- Classification of MalocclusionDocument8 pagesClassification of MalocclusionDevata RaviNo ratings yet
- Oral Surgery - Dr. Labeed SamiDocument22 pagesOral Surgery - Dr. Labeed SamiMohammed TarekNo ratings yet
- Copy1-Fraktur Mandibula (Edit)Document25 pagesCopy1-Fraktur Mandibula (Edit)debby nirmasariNo ratings yet
- Classification of Manfibular FractureDocument16 pagesClassification of Manfibular FractureFaheem AhmedNo ratings yet
- Anatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsDocument24 pagesAnatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsAlvaro Jose Uribe TamaraNo ratings yet
- Correcting The Class II Subdivision MalocclusionDocument2 pagesCorrecting The Class II Subdivision MalocclusionplsssssNo ratings yet
- Comparison of Orthodontic Techniques Used ForDocument5 pagesComparison of Orthodontic Techniques Used ForAdina SerbanNo ratings yet
- "Unilateral Subcondylar Fracture Treated by Close Reduction: A CaseDocument3 pages"Unilateral Subcondylar Fracture Treated by Close Reduction: A CaseAlbertine JaneNo ratings yet
- Craniofacial Deformities Review of Etiologies Distribution and TDocument16 pagesCraniofacial Deformities Review of Etiologies Distribution and TambersNo ratings yet
- Management of Class 3 MalocclusionDocument8 pagesManagement of Class 3 MalocclusionAkhil SinghNo ratings yet
- Review Artilces Annals and Essences of DentistryDocument14 pagesReview Artilces Annals and Essences of DentistryRahul Kumar DiwakarNo ratings yet
- CCD 9 342Document5 pagesCCD 9 342Anonymous 9PcFdakHcNo ratings yet
- Ge 2016Document9 pagesGe 2016Amani AouameurNo ratings yet
- Doraczynska Kowalik2017Document9 pagesDoraczynska Kowalik2017mahaaNo ratings yet
- Jurnal Asli JR Radiologi - Unusual Giant Complex Odontoma A Case ReportDocument4 pagesJurnal Asli JR Radiologi - Unusual Giant Complex Odontoma A Case ReportAliaNo ratings yet
- Orthodontic Camouflage in Skeletal Class III Malocclusion A Contemporary ReviewDocument5 pagesOrthodontic Camouflage in Skeletal Class III Malocclusion A Contemporary ReviewNatasha Ank100% (1)
- Classification Systems For Orofacial Clefts: 10.5005/jp-Journals-10037-1035Document5 pagesClassification Systems For Orofacial Clefts: 10.5005/jp-Journals-10037-1035assususuNo ratings yet
- Cleft Lip and Palate An Evidence Based Review PDFDocument16 pagesCleft Lip and Palate An Evidence Based Review PDFariskaNo ratings yet
- Surgical Management of Complex Mandibular Fracture: Case ReportDocument5 pagesSurgical Management of Complex Mandibular Fracture: Case ReportlindaNo ratings yet
- The Cleft-Columellar Angle A Useful Variable To deDocument7 pagesThe Cleft-Columellar Angle A Useful Variable To deaprilandralekaNo ratings yet
- Open Bite, A Review of Etiology and Manageme PDFDocument8 pagesOpen Bite, A Review of Etiology and Manageme PDFVieussens JoffreyNo ratings yet
- Mutifocal FracturesDocument4 pagesMutifocal FracturesElmer NarvaezNo ratings yet
- A To Z Orthodontics. Volume 19: Craniofacial Deformity: January 2011Document18 pagesA To Z Orthodontics. Volume 19: Craniofacial Deformity: January 2011MD MAHMUDUL HASAN NAEEMNo ratings yet
- Trauma Q&ADocument8 pagesTrauma Q&ANoor MaxeemNo ratings yet
- Fixed Functional Appliances For Treatment of Class II Malocclusions Effects and LimitationsDocument35 pagesFixed Functional Appliances For Treatment of Class II Malocclusions Effects and LimitationsAya ElsayedNo ratings yet
- Management of Lefort Fractures: Vijay Ebenezer, R. Balakrishnan and Anatha PadmanabhanDocument4 pagesManagement of Lefort Fractures: Vijay Ebenezer, R. Balakrishnan and Anatha PadmanabhanSuci NourmalizaNo ratings yet
- Broadie 2Document12 pagesBroadie 2Stefana NanuNo ratings yet
- LISCHER, B.E. The diagnosis of malocclusion. Dent. Cosmos 53412-22,1911.Document16 pagesLISCHER, B.E. The diagnosis of malocclusion. Dent. Cosmos 53412-22,1911.abigail.piresNo ratings yet
- Mandibular Condylar and Subcondylar Fractures PDFDocument16 pagesMandibular Condylar and Subcondylar Fractures PDFWayan Sutresna YasaNo ratings yet
- Classification of MalDocument7 pagesClassification of MalWeiliem AbubakarNo ratings yet
- Microssomia Ajodo 2014 PDFDocument16 pagesMicrossomia Ajodo 2014 PDFFabiane AzeredoNo ratings yet
- Class IIIElastics 2010Document11 pagesClass IIIElastics 2010febriNo ratings yet
- Cystic Lesions of MandibleDocument18 pagesCystic Lesions of MandibleRahul ShindeNo ratings yet
- Maxillofacial Defects and Their Classification: A Review.: ArticleDocument7 pagesMaxillofacial Defects and Their Classification: A Review.: ArticleVivek ShankarNo ratings yet
- Janson2010 PDFDocument10 pagesJanson2010 PDFMonojit DuttaNo ratings yet
- Class II - DD and MX PDFDocument14 pagesClass II - DD and MX PDFserahNo ratings yet
- 2016 SergioDocument10 pages2016 SergioazizhamoudNo ratings yet
- Sas 15 Den 032Document19 pagesSas 15 Den 032Alexa De GuzmanNo ratings yet
- Radiology of Cleft Lip and Palate: Imaging For The Prenatal Period and Throughout LifeDocument12 pagesRadiology of Cleft Lip and Palate: Imaging For The Prenatal Period and Throughout LifeAmeria Briliana ShoumiNo ratings yet
- How To Evaluate Dental Cavities in Horses: Stephen S. Galloway, DVMDocument8 pagesHow To Evaluate Dental Cavities in Horses: Stephen S. Galloway, DVMReza ChandraNo ratings yet
- Borderline Class III Patient and Treatment Options A Comprehensive Review PDFDocument3 pagesBorderline Class III Patient and Treatment Options A Comprehensive Review PDFOsama MohamedNo ratings yet
- Maxillofacial (Midface) FracturesDocument16 pagesMaxillofacial (Midface) FracturesYeraldin EspañaNo ratings yet
- 2215 3411 Odovtos 20 02 31Document7 pages2215 3411 Odovtos 20 02 31habeebNo ratings yet
- Class II Malocclusions Diagnostic and Clinical Considerations With and Without Treatment. Seminars in Orthodontics 12 (1) 11-24, Mar 2006. S. BisharaDocument14 pagesClass II Malocclusions Diagnostic and Clinical Considerations With and Without Treatment. Seminars in Orthodontics 12 (1) 11-24, Mar 2006. S. BisharaAhmad EgbariaNo ratings yet
- The Relationship Between Cranial Base Angle and Various Malocclusion TypesDocument5 pagesThe Relationship Between Cranial Base Angle and Various Malocclusion TypesAlvaro ChacónNo ratings yet
- 2015 Cleft Lip and Palate An Evidence-Based ReviewDocument16 pages2015 Cleft Lip and Palate An Evidence-Based ReviewDimitris RodriguezNo ratings yet
- 1 s2.0 S0929664609602643 MainDocument10 pages1 s2.0 S0929664609602643 MainCrisu CrisuuNo ratings yet
- Mahakal Institute of Pharamaceutical Studies, UjjainDocument8 pagesMahakal Institute of Pharamaceutical Studies, UjjainsafiyaNo ratings yet
- Safety Data Sheet: Revision Date: 15/06/2012 According To (EC) No. 1907/2006 (REACH), Annex II - United Kingdom (UK)Document8 pagesSafety Data Sheet: Revision Date: 15/06/2012 According To (EC) No. 1907/2006 (REACH), Annex II - United Kingdom (UK)AmirmasoudNo ratings yet
- Unit 2 - Role of Social Worker in Health FieldDocument10 pagesUnit 2 - Role of Social Worker in Health FieldDharek IleshNo ratings yet
- Temidayo Osunronbi Himanshu Sharma: Original Article - Spine - CordDocument10 pagesTemidayo Osunronbi Himanshu Sharma: Original Article - Spine - CordnulintavaNo ratings yet
- BDSM Experiences, Relationships, and Scenes in Southern DominantsDocument198 pagesBDSM Experiences, Relationships, and Scenes in Southern DominantsYvonne Yap Ying YingNo ratings yet
- A 33-Year-Old Woman With Trichoptysis, Diagnosed With Infiltrative Mature Mediastinal Teratoma: A Case ReportDocument15 pagesA 33-Year-Old Woman With Trichoptysis, Diagnosed With Infiltrative Mature Mediastinal Teratoma: A Case ReportElok NurfaiqohNo ratings yet
- NSTP FeatureDocument2 pagesNSTP FeatureCharisseNo ratings yet
- Alison Morton-Cooper Health Care and The Autism Spectrum A Guide For Health Professionals, Parents and Carers 2004Document130 pagesAlison Morton-Cooper Health Care and The Autism Spectrum A Guide For Health Professionals, Parents and Carers 2004lillouana100% (1)
- Vamana Karma-Understanding Mode of ActionDocument12 pagesVamana Karma-Understanding Mode of ActionsmsmastiNo ratings yet
- Health 7 LAS Quarter 3 1 1Document62 pagesHealth 7 LAS Quarter 3 1 1raymart zalunNo ratings yet
- CS2 Booklet 7 (Mortality Projection) 2019 FINALDocument38 pagesCS2 Booklet 7 (Mortality Projection) 2019 FINALAnsh ParmarNo ratings yet
- BioavailabilityDocument15 pagesBioavailabilitywriter noreenNo ratings yet
- Pe 8 Q1 W1-8-Module-2023Document59 pagesPe 8 Q1 W1-8-Module-2023Arianne B. CabañezNo ratings yet
- Section 1 - Chemical Product and Company Information: Safety Data Sheet - Sulfur Hexafluoride (SF)Document8 pagesSection 1 - Chemical Product and Company Information: Safety Data Sheet - Sulfur Hexafluoride (SF)sufizamaniNo ratings yet
- Module 3 - SociologyDocument74 pagesModule 3 - SociologyakshayaNo ratings yet
- Chromium, Hexavalent, Method 8023, 02-2009, 9th EdDocument6 pagesChromium, Hexavalent, Method 8023, 02-2009, 9th EdTicha MaharaniNo ratings yet
- Nutrition Therapy For Adults With Diabetes or Prediabetes A Consensus Report - 2019 PDFDocument24 pagesNutrition Therapy For Adults With Diabetes or Prediabetes A Consensus Report - 2019 PDFNicolás Di SantoroNo ratings yet
- Comparison of The Solubilization Effect of Micronized PoloxamersDocument1 pageComparison of The Solubilization Effect of Micronized Poloxamerssaeedazadi1352No ratings yet
- GASTROINTESTINALDocument8 pagesGASTROINTESTINALrheantiffany0815No ratings yet
- Risk For Impaired Skin IntegrityDocument4 pagesRisk For Impaired Skin IntegrityArelys Rodriguez100% (2)
- Medical Ethics/Ethical PrinciplesDocument20 pagesMedical Ethics/Ethical PrinciplesPALATTAO, AUBRIE L. BSMT2-8No ratings yet
- Exam 4th GradingDocument8 pagesExam 4th Gradingedward surtido100% (1)
- Hci Report Group3Document15 pagesHci Report Group3api-302906387No ratings yet
- Daftar Formulariumobat SementaraDocument26 pagesDaftar Formulariumobat SementarafarmasiNo ratings yet
- Descriptive Questions Asked in Previous Years IBPS PO Mains ExamDocument5 pagesDescriptive Questions Asked in Previous Years IBPS PO Mains ExamAnwesha SahooNo ratings yet
- 2007ccj Research EssayDocument10 pages2007ccj Research EssayGeorgie FriedrichsNo ratings yet
- ALT GPT (IFCC) Single Vial: BiolaboDocument2 pagesALT GPT (IFCC) Single Vial: Biolabowindy ajengNo ratings yet
- Aldridge A Short Introduction To CounsellingDocument22 pagesAldridge A Short Introduction To Counsellingbyron chieNo ratings yet