
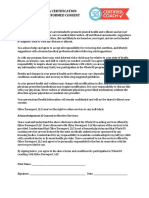
OMMA Medical Card Doctor Recommendation
OMMA Medical Card Doctor Recommendation
You might also like
- Fake Abortion Form TemplateDocument4 pagesFake Abortion Form Templateyouismyfavcolour67% (3)
- Evaluation of Change ProcessDocument12 pagesEvaluation of Change ProcessThe Hoopers100% (1)
- Emotion Code-Body Code Consent AgreementDocument1 pageEmotion Code-Body Code Consent Agreementapi-75991446100% (1)
- Holistic Questionnaire TemplateDocument1 pageHolistic Questionnaire TemplateMegs EmrysNo ratings yet
- Introduction NawalokaDocument2 pagesIntroduction Nawalokafox m100% (2)
- Legal MedicineDocument4 pagesLegal MedicineJamie TiuNo ratings yet
- AF Form 2030Document2 pagesAF Form 2030David AsadourianNo ratings yet
- Career Investigation Report - PVDocument4 pagesCareer Investigation Report - PVaryan235No ratings yet
- Callegan Medication Agreement 121418Document4 pagesCallegan Medication Agreement 121418api-457393626No ratings yet
- New Hampshire Living WillDocument7 pagesNew Hampshire Living WillRocketLawyerNo ratings yet
- Advance Directive For Medical / Surgical Treatment (Living Will) - ColoradoDocument6 pagesAdvance Directive For Medical / Surgical Treatment (Living Will) - ColoradocleincoloradoNo ratings yet
- PH Advance DirectivesDocument9 pagesPH Advance DirectivesTracy Johnson-GauffNo ratings yet
- LivingWill TexasDocument3 pagesLivingWill TexasAmesNo ratings yet
- Health Care Proxy: Appointing Your Health Care Agent in New York StateDocument8 pagesHealth Care Proxy: Appointing Your Health Care Agent in New York StateKabakçı HüsnüNo ratings yet
- Patient Consent FormDocument1 pagePatient Consent Formwaseem iqbalNo ratings yet
- Sample Treatment Agreement: Medication Misuse Medication MisuseDocument2 pagesSample Treatment Agreement: Medication Misuse Medication MisuseStella Iris MillerNo ratings yet
- Jane Doe Advance DirDocument24 pagesJane Doe Advance Dirapi-224104463No ratings yet
- Contoh General ConsentDocument1 pageContoh General ConsentMahendra AbdythamaNo ratings yet
- Oregon Medical Marijuana Act HandbookDocument24 pagesOregon Medical Marijuana Act HandbookornormlNo ratings yet
- HCP FormDocument8 pagesHCP FormMarkNo ratings yet
- Health Care ProxyDocument8 pagesHealth Care ProxyProject FINDNo ratings yet
- North Carolina Medical Board: Via Attorney of RecordDocument4 pagesNorth Carolina Medical Board: Via Attorney of RecordJennifer EmertNo ratings yet
- Durable Power of AttorneyDocument3 pagesDurable Power of AttorneyTlecoz HuitzilNo ratings yet
- Dpo Ah C Louie Wayne PittmanDocument9 pagesDpo Ah C Louie Wayne PittmanCricketandScott HintonNo ratings yet
- Sample Patient ContractDocument3 pagesSample Patient ContractImc AyurvedNo ratings yet
- Nevada Living WillDocument7 pagesNevada Living WillRocketLawyer100% (1)
- Canada Drugs Direct PAFDocument1 pageCanada Drugs Direct PAFrjohngdcNo ratings yet
- Patient Self Determination Act: Mississippi Advance Health-Care DirectiveDocument17 pagesPatient Self Determination Act: Mississippi Advance Health-Care DirectiveKristin JonesNo ratings yet
- Unlicensed Medicines - DoneDocument8 pagesUnlicensed Medicines - DonepdladvaNo ratings yet
- NY Advance Directive: Living Will & Healthcare Proxy Aka Power of AttorneyDocument15 pagesNY Advance Directive: Living Will & Healthcare Proxy Aka Power of AttorneythedundiesNo ratings yet
- Consent Form Emotion Code Body Code t3 Additional ChartsDocument1 pageConsent Form Emotion Code Body Code t3 Additional ChartsMark Trenton50% (2)
- Texas Living WillDocument5 pagesTexas Living WillRocketLawyerNo ratings yet
- Carbondale Family Medicine: Dr. Mukesh Chaudhry, M.DDocument1 pageCarbondale Family Medicine: Dr. Mukesh Chaudhry, M.Dvhel05No ratings yet
- Informed Consent and Petition For Assistance ENDocument2 pagesInformed Consent and Petition For Assistance ENgabrielaizcorbeNo ratings yet
- Informed ConsentDocument2 pagesInformed ConsentdrnacuNo ratings yet
- Informed Consent Form Whole30 2017Document1 pageInformed Consent Form Whole30 2017api-385355641No ratings yet
- Georgia Living WillDocument9 pagesGeorgia Living WillRocketLawyer100% (2)
- Notice of Privacy PracticesDocument6 pagesNotice of Privacy PracticesJames LanierNo ratings yet
- New Jersey Living WillDocument4 pagesNew Jersey Living WillRocketLawyer100% (1)
- PennsylvaniaDocument17 pagesPennsylvaniaRevNo ratings yet
- Vs County and StateDocument4 pagesVs County and StatethewizardsofcontentNo ratings yet
- Medical JurisprudenceDocument16 pagesMedical JurisprudenceCath VillarinNo ratings yet
- Michigan's Medical Marihuana ActDocument27 pagesMichigan's Medical Marihuana Actapi-25946258No ratings yet
- Combined Consent Intake GeneralDocument8 pagesCombined Consent Intake Generalkimmiej.gilbertNo ratings yet
- Reliability of No Win No Fee & Medical Negligence: GP Complaint SpecialistsDocument2 pagesReliability of No Win No Fee & Medical Negligence: GP Complaint SpecialistsEman KhanNo ratings yet
- Advanced Directive & Durable Power of Attorney For Health CareDocument6 pagesAdvanced Directive & Durable Power of Attorney For Health CareTexieraNo ratings yet
- Mapeh 6: Quarter 4 - Module 1Document10 pagesMapeh 6: Quarter 4 - Module 1ALEX CORPORALNo ratings yet
- Informed Consent For Medication: Opioid Antagonist Revia (Naltrexone) Dosing Schedule Determined by PhysicianDocument3 pagesInformed Consent For Medication: Opioid Antagonist Revia (Naltrexone) Dosing Schedule Determined by Physiciandnutter012576No ratings yet
- Sample Patient Agreement FormsDocument5 pagesSample Patient Agreement FormsEmmieNo ratings yet
- The Pharmaceutical Myth: Letting Food be Your Medicine is the Answer for Perfect HealthFrom EverandThe Pharmaceutical Myth: Letting Food be Your Medicine is the Answer for Perfect HealthNo ratings yet
- Advance Directive - CADocument20 pagesAdvance Directive - CAMiloBoiNo ratings yet
- Keywords: Ailments, Availability and Legality, Aware, Epilepsy, High, KnowledgeableDocument18 pagesKeywords: Ailments, Availability and Legality, Aware, Epilepsy, High, KnowledgeablePatrick DgNo ratings yet
- Medical Power of AttorneyDocument4 pagesMedical Power of AttorneybrettNo ratings yet
- Medical Marijuana Access & Patient Safety Inc. v. Keara Klinepeter Et AlDocument99 pagesMedical Marijuana Access & Patient Safety Inc. v. Keara Klinepeter Et AlsandydocsNo ratings yet
- Transformative Health Strategies: Integrative Medicine and the COVID-19 PandemicFrom EverandTransformative Health Strategies: Integrative Medicine and the COVID-19 PandemicNo ratings yet
- Illinois Guide For Doctors and PatientsDocument2 pagesIllinois Guide For Doctors and PatientsMPPNo ratings yet
- Marigold Vet FormsDocument6 pagesMarigold Vet FormsJocthan JirehNo ratings yet
- Power of Attorney, Durable, For Health CareDocument7 pagesPower of Attorney, Durable, For Health Caremichael nedd100% (1)
- ANA Position StatementDocument3 pagesANA Position StatementBethuel KamauNo ratings yet
- Incorrect, Refilling, Multiple and Sharing: Group #1Document17 pagesIncorrect, Refilling, Multiple and Sharing: Group #1Majoy BodolloNo ratings yet
- MH 556 09/11/06Document1 pageMH 556 09/11/06jeffrey_kingNo ratings yet
- Drug Education in The PhilippinesDocument32 pagesDrug Education in The PhilippinesTrixie Ann MenesesNo ratings yet
- Injuries of The Sporting KneeDocument3 pagesInjuries of The Sporting KneeDanar Hari AdhimuktiNo ratings yet
- Medical Negligence Litigation in Malaysia: Current Trend and Proposals For ReformDocument65 pagesMedical Negligence Litigation in Malaysia: Current Trend and Proposals For ReformAweisNo ratings yet
- Module 1 - Self-Guided Activity WorksheetDocument3 pagesModule 1 - Self-Guided Activity WorksheetAamena MultaniNo ratings yet
- Family Nursing and Family Health Nursing ProcessDocument92 pagesFamily Nursing and Family Health Nursing ProcessKailash NagarNo ratings yet
- Bookshelf NBK133363 PDFDocument945 pagesBookshelf NBK133363 PDFMolgen PanjaitanNo ratings yet
- CGMC Posting Details inDocument31 pagesCGMC Posting Details in4hc2q8tgyvNo ratings yet
- Questions and Answers From The Webinar Community Health Workers: Their Role in Preventing and Controlling Chronic ConditionsDocument13 pagesQuestions and Answers From The Webinar Community Health Workers: Their Role in Preventing and Controlling Chronic ConditionsGift EseNo ratings yet
- The Efficacy of Manual Therapy For Rotator Cuff Tendinopathy: A Systematic Review and Meta AnalysisDocument21 pagesThe Efficacy of Manual Therapy For Rotator Cuff Tendinopathy: A Systematic Review and Meta AnalysisJacinta SeguraNo ratings yet
- MDS Course Regulations 2007 Alongwith AmendmentsDocument133 pagesMDS Course Regulations 2007 Alongwith AmendmentsSyed NooraniNo ratings yet
- Does Social Class Affect Your Mental Health - PPTX 1Document16 pagesDoes Social Class Affect Your Mental Health - PPTX 1karah13No ratings yet
- Project ProposalDocument4 pagesProject ProposalAngel Faith TirolNo ratings yet
- TERAPIA NUTRICIONAL EN SEPSIS WischmeyerDocument21 pagesTERAPIA NUTRICIONAL EN SEPSIS WischmeyerHéctor Juárez GrandaNo ratings yet
- Expansion of Medicaid Coverage Critical Analysis Paper - Sletta MataDocument11 pagesExpansion of Medicaid Coverage Critical Analysis Paper - Sletta Mataapi-497063972No ratings yet
- Greene & Manfredini - Treating TMD in 21st Century.2020Document11 pagesGreene & Manfredini - Treating TMD in 21st Century.2020Beth AguiarNo ratings yet
- Comp 2 Research EssayDocument10 pagesComp 2 Research Essayapi-510711312No ratings yet
- Portfolio Job DescriptionDocument3 pagesPortfolio Job Descriptionapi-259260464No ratings yet
- Hospital-List-2!20!2007 (Ross What To Do)Document19 pagesHospital-List-2!20!2007 (Ross What To Do)ibgirl17No ratings yet
- CNE Credits Hours DetailsDocument15 pagesCNE Credits Hours DetailsKinjal VasavaNo ratings yet
- Protein Calorie MalnutritionDocument6 pagesProtein Calorie MalnutritionfirdakusumaputriNo ratings yet
- Cadila Healthca-WPS Office 444444Document22 pagesCadila Healthca-WPS Office 444444Abhimanyu gkpNo ratings yet
- Poster Papostblo Aguilar 3Document1 pagePoster Papostblo Aguilar 3Juan Pablo AguilarNo ratings yet
- Chinmay Pandya ProfileDocument1 pageChinmay Pandya Profileice_fire0073075No ratings yet
- Pengetahuan Dan Persepsi Peserta Prolanis Dalam Menjalani Pengobatan Di PuskesmasDocument7 pagesPengetahuan Dan Persepsi Peserta Prolanis Dalam Menjalani Pengobatan Di PuskesmasUmmulAklaNo ratings yet
- Intraoperative NursingDocument41 pagesIntraoperative NursingBryan Mae H. Degorio100% (11)
- Knowledge, Attitude and Awareness of Intraoral Radiographic Imaging Techniques Among Dental Students Across Chennai A Questionnaire StudyDocument6 pagesKnowledge, Attitude and Awareness of Intraoral Radiographic Imaging Techniques Among Dental Students Across Chennai A Questionnaire StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biography of Madeleine LeiningerDocument3 pagesBiography of Madeleine LeiningerNajihah :sNo ratings yet
- Ped Ob Reflection 1Document4 pagesPed Ob Reflection 1api-581678058No ratings yet





















































































Download as pdf or txt
You might also like
- Fake Abortion Form TemplateDocument4 pagesFake Abortion Form Templateyouismyfavcolour67% (3)
- Evaluation of Change ProcessDocument12 pagesEvaluation of Change ProcessThe Hoopers100% (1)
- Emotion Code-Body Code Consent AgreementDocument1 pageEmotion Code-Body Code Consent Agreementapi-75991446100% (1)
- Holistic Questionnaire TemplateDocument1 pageHolistic Questionnaire TemplateMegs EmrysNo ratings yet
- Introduction NawalokaDocument2 pagesIntroduction Nawalokafox m100% (2)
- Legal MedicineDocument4 pagesLegal MedicineJamie TiuNo ratings yet
- AF Form 2030Document2 pagesAF Form 2030David AsadourianNo ratings yet
- Career Investigation Report - PVDocument4 pagesCareer Investigation Report - PVaryan235No ratings yet
- Callegan Medication Agreement 121418Document4 pagesCallegan Medication Agreement 121418api-457393626No ratings yet
- New Hampshire Living WillDocument7 pagesNew Hampshire Living WillRocketLawyerNo ratings yet
- Advance Directive For Medical / Surgical Treatment (Living Will) - ColoradoDocument6 pagesAdvance Directive For Medical / Surgical Treatment (Living Will) - ColoradocleincoloradoNo ratings yet
- PH Advance DirectivesDocument9 pagesPH Advance DirectivesTracy Johnson-GauffNo ratings yet
- LivingWill TexasDocument3 pagesLivingWill TexasAmesNo ratings yet
- Health Care Proxy: Appointing Your Health Care Agent in New York StateDocument8 pagesHealth Care Proxy: Appointing Your Health Care Agent in New York StateKabakçı HüsnüNo ratings yet
- Patient Consent FormDocument1 pagePatient Consent Formwaseem iqbalNo ratings yet
- Sample Treatment Agreement: Medication Misuse Medication MisuseDocument2 pagesSample Treatment Agreement: Medication Misuse Medication MisuseStella Iris MillerNo ratings yet
- Jane Doe Advance DirDocument24 pagesJane Doe Advance Dirapi-224104463No ratings yet
- Contoh General ConsentDocument1 pageContoh General ConsentMahendra AbdythamaNo ratings yet
- Oregon Medical Marijuana Act HandbookDocument24 pagesOregon Medical Marijuana Act HandbookornormlNo ratings yet
- HCP FormDocument8 pagesHCP FormMarkNo ratings yet
- Health Care ProxyDocument8 pagesHealth Care ProxyProject FINDNo ratings yet
- North Carolina Medical Board: Via Attorney of RecordDocument4 pagesNorth Carolina Medical Board: Via Attorney of RecordJennifer EmertNo ratings yet
- Durable Power of AttorneyDocument3 pagesDurable Power of AttorneyTlecoz HuitzilNo ratings yet
- Dpo Ah C Louie Wayne PittmanDocument9 pagesDpo Ah C Louie Wayne PittmanCricketandScott HintonNo ratings yet
- Sample Patient ContractDocument3 pagesSample Patient ContractImc AyurvedNo ratings yet
- Nevada Living WillDocument7 pagesNevada Living WillRocketLawyer100% (1)
- Canada Drugs Direct PAFDocument1 pageCanada Drugs Direct PAFrjohngdcNo ratings yet
- Patient Self Determination Act: Mississippi Advance Health-Care DirectiveDocument17 pagesPatient Self Determination Act: Mississippi Advance Health-Care DirectiveKristin JonesNo ratings yet
- Unlicensed Medicines - DoneDocument8 pagesUnlicensed Medicines - DonepdladvaNo ratings yet
- NY Advance Directive: Living Will & Healthcare Proxy Aka Power of AttorneyDocument15 pagesNY Advance Directive: Living Will & Healthcare Proxy Aka Power of AttorneythedundiesNo ratings yet
- Consent Form Emotion Code Body Code t3 Additional ChartsDocument1 pageConsent Form Emotion Code Body Code t3 Additional ChartsMark Trenton50% (2)
- Texas Living WillDocument5 pagesTexas Living WillRocketLawyerNo ratings yet
- Carbondale Family Medicine: Dr. Mukesh Chaudhry, M.DDocument1 pageCarbondale Family Medicine: Dr. Mukesh Chaudhry, M.Dvhel05No ratings yet
- Informed Consent and Petition For Assistance ENDocument2 pagesInformed Consent and Petition For Assistance ENgabrielaizcorbeNo ratings yet
- Informed ConsentDocument2 pagesInformed ConsentdrnacuNo ratings yet
- Informed Consent Form Whole30 2017Document1 pageInformed Consent Form Whole30 2017api-385355641No ratings yet
- Georgia Living WillDocument9 pagesGeorgia Living WillRocketLawyer100% (2)
- Notice of Privacy PracticesDocument6 pagesNotice of Privacy PracticesJames LanierNo ratings yet
- New Jersey Living WillDocument4 pagesNew Jersey Living WillRocketLawyer100% (1)
- PennsylvaniaDocument17 pagesPennsylvaniaRevNo ratings yet
- Vs County and StateDocument4 pagesVs County and StatethewizardsofcontentNo ratings yet
- Medical JurisprudenceDocument16 pagesMedical JurisprudenceCath VillarinNo ratings yet
- Michigan's Medical Marihuana ActDocument27 pagesMichigan's Medical Marihuana Actapi-25946258No ratings yet
- Combined Consent Intake GeneralDocument8 pagesCombined Consent Intake Generalkimmiej.gilbertNo ratings yet
- Reliability of No Win No Fee & Medical Negligence: GP Complaint SpecialistsDocument2 pagesReliability of No Win No Fee & Medical Negligence: GP Complaint SpecialistsEman KhanNo ratings yet
- Advanced Directive & Durable Power of Attorney For Health CareDocument6 pagesAdvanced Directive & Durable Power of Attorney For Health CareTexieraNo ratings yet
- Mapeh 6: Quarter 4 - Module 1Document10 pagesMapeh 6: Quarter 4 - Module 1ALEX CORPORALNo ratings yet
- Informed Consent For Medication: Opioid Antagonist Revia (Naltrexone) Dosing Schedule Determined by PhysicianDocument3 pagesInformed Consent For Medication: Opioid Antagonist Revia (Naltrexone) Dosing Schedule Determined by Physiciandnutter012576No ratings yet
- Sample Patient Agreement FormsDocument5 pagesSample Patient Agreement FormsEmmieNo ratings yet
- The Pharmaceutical Myth: Letting Food be Your Medicine is the Answer for Perfect HealthFrom EverandThe Pharmaceutical Myth: Letting Food be Your Medicine is the Answer for Perfect HealthNo ratings yet
- Advance Directive - CADocument20 pagesAdvance Directive - CAMiloBoiNo ratings yet
- Keywords: Ailments, Availability and Legality, Aware, Epilepsy, High, KnowledgeableDocument18 pagesKeywords: Ailments, Availability and Legality, Aware, Epilepsy, High, KnowledgeablePatrick DgNo ratings yet
- Medical Power of AttorneyDocument4 pagesMedical Power of AttorneybrettNo ratings yet
- Medical Marijuana Access & Patient Safety Inc. v. Keara Klinepeter Et AlDocument99 pagesMedical Marijuana Access & Patient Safety Inc. v. Keara Klinepeter Et AlsandydocsNo ratings yet
- Transformative Health Strategies: Integrative Medicine and the COVID-19 PandemicFrom EverandTransformative Health Strategies: Integrative Medicine and the COVID-19 PandemicNo ratings yet
- Illinois Guide For Doctors and PatientsDocument2 pagesIllinois Guide For Doctors and PatientsMPPNo ratings yet
- Marigold Vet FormsDocument6 pagesMarigold Vet FormsJocthan JirehNo ratings yet
- Power of Attorney, Durable, For Health CareDocument7 pagesPower of Attorney, Durable, For Health Caremichael nedd100% (1)
- ANA Position StatementDocument3 pagesANA Position StatementBethuel KamauNo ratings yet
- Incorrect, Refilling, Multiple and Sharing: Group #1Document17 pagesIncorrect, Refilling, Multiple and Sharing: Group #1Majoy BodolloNo ratings yet
- MH 556 09/11/06Document1 pageMH 556 09/11/06jeffrey_kingNo ratings yet
- Drug Education in The PhilippinesDocument32 pagesDrug Education in The PhilippinesTrixie Ann MenesesNo ratings yet
- Injuries of The Sporting KneeDocument3 pagesInjuries of The Sporting KneeDanar Hari AdhimuktiNo ratings yet
- Medical Negligence Litigation in Malaysia: Current Trend and Proposals For ReformDocument65 pagesMedical Negligence Litigation in Malaysia: Current Trend and Proposals For ReformAweisNo ratings yet
- Module 1 - Self-Guided Activity WorksheetDocument3 pagesModule 1 - Self-Guided Activity WorksheetAamena MultaniNo ratings yet
- Family Nursing and Family Health Nursing ProcessDocument92 pagesFamily Nursing and Family Health Nursing ProcessKailash NagarNo ratings yet
- Bookshelf NBK133363 PDFDocument945 pagesBookshelf NBK133363 PDFMolgen PanjaitanNo ratings yet
- CGMC Posting Details inDocument31 pagesCGMC Posting Details in4hc2q8tgyvNo ratings yet
- Questions and Answers From The Webinar Community Health Workers: Their Role in Preventing and Controlling Chronic ConditionsDocument13 pagesQuestions and Answers From The Webinar Community Health Workers: Their Role in Preventing and Controlling Chronic ConditionsGift EseNo ratings yet
- The Efficacy of Manual Therapy For Rotator Cuff Tendinopathy: A Systematic Review and Meta AnalysisDocument21 pagesThe Efficacy of Manual Therapy For Rotator Cuff Tendinopathy: A Systematic Review and Meta AnalysisJacinta SeguraNo ratings yet
- MDS Course Regulations 2007 Alongwith AmendmentsDocument133 pagesMDS Course Regulations 2007 Alongwith AmendmentsSyed NooraniNo ratings yet
- Does Social Class Affect Your Mental Health - PPTX 1Document16 pagesDoes Social Class Affect Your Mental Health - PPTX 1karah13No ratings yet
- Project ProposalDocument4 pagesProject ProposalAngel Faith TirolNo ratings yet
- TERAPIA NUTRICIONAL EN SEPSIS WischmeyerDocument21 pagesTERAPIA NUTRICIONAL EN SEPSIS WischmeyerHéctor Juárez GrandaNo ratings yet
- Expansion of Medicaid Coverage Critical Analysis Paper - Sletta MataDocument11 pagesExpansion of Medicaid Coverage Critical Analysis Paper - Sletta Mataapi-497063972No ratings yet
- Greene & Manfredini - Treating TMD in 21st Century.2020Document11 pagesGreene & Manfredini - Treating TMD in 21st Century.2020Beth AguiarNo ratings yet
- Comp 2 Research EssayDocument10 pagesComp 2 Research Essayapi-510711312No ratings yet
- Portfolio Job DescriptionDocument3 pagesPortfolio Job Descriptionapi-259260464No ratings yet
- Hospital-List-2!20!2007 (Ross What To Do)Document19 pagesHospital-List-2!20!2007 (Ross What To Do)ibgirl17No ratings yet
- CNE Credits Hours DetailsDocument15 pagesCNE Credits Hours DetailsKinjal VasavaNo ratings yet
- Protein Calorie MalnutritionDocument6 pagesProtein Calorie MalnutritionfirdakusumaputriNo ratings yet
- Cadila Healthca-WPS Office 444444Document22 pagesCadila Healthca-WPS Office 444444Abhimanyu gkpNo ratings yet
- Poster Papostblo Aguilar 3Document1 pagePoster Papostblo Aguilar 3Juan Pablo AguilarNo ratings yet
- Chinmay Pandya ProfileDocument1 pageChinmay Pandya Profileice_fire0073075No ratings yet
- Pengetahuan Dan Persepsi Peserta Prolanis Dalam Menjalani Pengobatan Di PuskesmasDocument7 pagesPengetahuan Dan Persepsi Peserta Prolanis Dalam Menjalani Pengobatan Di PuskesmasUmmulAklaNo ratings yet
- Intraoperative NursingDocument41 pagesIntraoperative NursingBryan Mae H. Degorio100% (11)
- Knowledge, Attitude and Awareness of Intraoral Radiographic Imaging Techniques Among Dental Students Across Chennai A Questionnaire StudyDocument6 pagesKnowledge, Attitude and Awareness of Intraoral Radiographic Imaging Techniques Among Dental Students Across Chennai A Questionnaire StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biography of Madeleine LeiningerDocument3 pagesBiography of Madeleine LeiningerNajihah :sNo ratings yet
- Ped Ob Reflection 1Document4 pagesPed Ob Reflection 1api-581678058No ratings yet