Download as pdf or txt
You might also like
- Persuasive Speech OutlineDocument5 pagesPersuasive Speech Outlineapi-355421848100% (4)
- Criteria of MaturityDocument14 pagesCriteria of MaturityZyrene Lee JovenNo ratings yet
- 8 Bookshelf - NBK493367-1 PDFDocument175 pages8 Bookshelf - NBK493367-1 PDFandi dirhanNo ratings yet
- 4Document8 pages4Lakhwinder KaurNo ratings yet
- PDF 3Document5 pagesPDF 3Amina GoharyNo ratings yet
- Christy ArticleDocument13 pagesChristy ArticleKenneth MelchorNo ratings yet
- pARTO NA ESCOLIOSEDocument8 pagespARTO NA ESCOLIOSElucas guerraNo ratings yet
- Effect of Physiotherapy On Spinal AlignmentDocument8 pagesEffect of Physiotherapy On Spinal Alignmentnistormaria492No ratings yet
- WeeFIM Clinical ReviewDocument10 pagesWeeFIM Clinical Reviewsss_sarzzzNo ratings yet
- Nihms 726255Document18 pagesNihms 726255Jem Rhod CamenseNo ratings yet
- Rendeli 2005Document6 pagesRendeli 2005Dimple GoyalNo ratings yet
- 2 10.1016@j.jspd.2017.12.007-1Document6 pages2 10.1016@j.jspd.2017.12.007-1andi dirhanNo ratings yet
- Efficiency of Kinesiotaping Application in The Complex Rehabilitation of Children With Idiopathic ScoliosisDocument4 pagesEfficiency of Kinesiotaping Application in The Complex Rehabilitation of Children With Idiopathic ScoliosisSasongko Prabasworo AnindyojatiNo ratings yet
- Yao2017 PDFDocument27 pagesYao2017 PDFArie BaldwellNo ratings yet
- Pedi-Cat PCDocument7 pagesPedi-Cat PCLetícia AndradeNo ratings yet
- Jurnal 6Document17 pagesJurnal 6Dhiny RatuNo ratings yet
- Normal Lower Limb Variants in ChildrenDocument11 pagesNormal Lower Limb Variants in ChildrenIulia MoldovanNo ratings yet
- Long-Term Outcome of Infants With Positional Occipital PlagiocephalyDocument9 pagesLong-Term Outcome of Infants With Positional Occipital PlagiocephalychiaraNo ratings yet
- Lippincott Williams & Wilkins: Info/about/policies/terms - JSPDocument14 pagesLippincott Williams & Wilkins: Info/about/policies/terms - JSPThayla Amorim SantinoNo ratings yet
- Comparison of Vision-Related Quality of Life Between Wearing Orthokeratology Lenses and Spectacles in Myopic Children LDocument5 pagesComparison of Vision-Related Quality of Life Between Wearing Orthokeratology Lenses and Spectacles in Myopic Children Lกนกกานต์ ธาดาธัญลักษณ์No ratings yet
- Non-Surgical Intervention of Knee Flexion Contracture in Children With Spina Bifida: Case ReportDocument3 pagesNon-Surgical Intervention of Knee Flexion Contracture in Children With Spina Bifida: Case ReportganditNo ratings yet
- Bone & Joint 360 Children's Orthopaedics August 2014Document3 pagesBone & Joint 360 Children's Orthopaedics August 2014Cosmin AlexaNo ratings yet
- Research Proposal 2Document14 pagesResearch Proposal 2Abhishek SharmaNo ratings yet
- Aus Occup Therapy J - 2019 - Novak - Effectiveness of Paediatric Occupational Therapy For Children With Disabilities ADocument16 pagesAus Occup Therapy J - 2019 - Novak - Effectiveness of Paediatric Occupational Therapy For Children With Disabilities Ashaima nasimNo ratings yet
- ICCS Standardization Report On Urodynamic StudiesDocument8 pagesICCS Standardization Report On Urodynamic StudiesAndy WijayaNo ratings yet
- Hsieh2015 PDFDocument1 pageHsieh2015 PDFDeana MonicaNo ratings yet
- Pediatrics 2011 Brooks Peds.2010 2801 PDFDocument11 pagesPediatrics 2011 Brooks Peds.2010 2801 PDFAntonioNo ratings yet
- Schiariti 2016Document24 pagesSchiariti 2016Gustavo BrandãoNo ratings yet
- Art 6 DaDocument8 pagesArt 6 DaDiana Sofia AgredaNo ratings yet
- Active Self-Correction and Task-Oriented Exercises Reduce Spinal Deformity and Improve Quality of Life in Subjects With Mild Adolescent Idiopathic Scoliosis. Results of A Randomised Controlled TrialDocument11 pagesActive Self-Correction and Task-Oriented Exercises Reduce Spinal Deformity and Improve Quality of Life in Subjects With Mild Adolescent Idiopathic Scoliosis. Results of A Randomised Controlled TrialCarolina Drummond Rocha MoraisNo ratings yet
- PEDIJosenbyetal 2014Document9 pagesPEDIJosenbyetal 2014Alexander BenavidesNo ratings yet
- 2023 - Development and Validation of A New Tool The Sarcopenia Knowledge QuestionnaireDocument6 pages2023 - Development and Validation of A New Tool The Sarcopenia Knowledge QuestionnaireAlex LimaNo ratings yet
- Sci1301 1Document10 pagesSci1301 1Edwin Ade SaputraNo ratings yet
- 12.tummy TimeDocument27 pages12.tummy TimeAtikah AbayNo ratings yet
- Review ArticleDocument13 pagesReview ArticleIchigo RukiaNo ratings yet
- Use of The Skeletal Survey in The Evaluation of Child MaltreatmentDocument3 pagesUse of The Skeletal Survey in The Evaluation of Child MaltreatmentAprilia DhammashintaNo ratings yet
- Surgical Correction of Equinus Deformity - in - ChildrDocument15 pagesSurgical Correction of Equinus Deformity - in - ChildrGuillermo FuenmayorNo ratings yet
- Effectiveness of Klapp Exercise To Treat Angle Currence in Children With Scoliosis: Literature ReviewDocument11 pagesEffectiveness of Klapp Exercise To Treat Angle Currence in Children With Scoliosis: Literature ReviewAlejandra GiraldoNo ratings yet
- The Pediatric "Floating Knee" Injury: A State-of-the-Art Multicenter StudyDocument7 pagesThe Pediatric "Floating Knee" Injury: A State-of-the-Art Multicenter StudyManiDeep ReddyNo ratings yet
- Analyzing Spinal Curves For Prolong Sitting in University Going StudentsDocument8 pagesAnalyzing Spinal Curves For Prolong Sitting in University Going StudentsMr DanielNo ratings yet
- 2 51 1584079747 4.ijmpsapr20204Document18 pages2 51 1584079747 4.ijmpsapr20204TJPRC PublicationsNo ratings yet
- 2014 Test-Retest Reliability of The Star Excursion Balance Test in Primary School ChildrenDocument5 pages2014 Test-Retest Reliability of The Star Excursion Balance Test in Primary School ChildrenDiego Subiabre100% (1)
- Reability ODIDocument17 pagesReability ODIAnonymous mWAaDZmlJwNo ratings yet
- Suresh 2015Document6 pagesSuresh 2015ade_liaNo ratings yet
- Two Novel Clinical Tests For The Diagnosis of Hip Labral TearsDocument8 pagesTwo Novel Clinical Tests For The Diagnosis of Hip Labral TearsmontseNo ratings yet
- Yabunaka 2011Document9 pagesYabunaka 2011Carolina BorchesNo ratings yet
- DentalDocument7 pagesDentalcahayaNo ratings yet
- (Egashira, R., Et Al., 2022) Japan Frailty IndexDocument13 pages(Egashira, R., Et Al., 2022) Japan Frailty IndexPPDS Rehab Medik UnhasNo ratings yet
- The SWAL-QOL Outcomes Tool For Oropharyngeal DysphDocument13 pagesThe SWAL-QOL Outcomes Tool For Oropharyngeal DysphRaja PahleviNo ratings yet
- Circulation 2015 Pediatria PalsDocument28 pagesCirculation 2015 Pediatria Palslizzie clavijoNo ratings yet
- Jurnal UtamaDocument9 pagesJurnal UtamajanakaNo ratings yet
- Ohtas 17 1Document186 pagesOhtas 17 1Ismail GuruSingaNo ratings yet
- He 2017Document20 pagesHe 2017mostafa mahmoudNo ratings yet
- Skirko 2012Document7 pagesSkirko 2012Olivier MaronNo ratings yet
- Evidence For The Use of Spinall Collars in Stabilising Spinal Injuries in The Prehospital Setting in Trauma PatientsDocument11 pagesEvidence For The Use of Spinall Collars in Stabilising Spinal Injuries in The Prehospital Setting in Trauma PatientsSarahi Rodriguez GalindoNo ratings yet
- 1 s2.0 S188844152300190X MainDocument7 pages1 s2.0 S188844152300190X MainMaría José Ruiz PastorNo ratings yet
- Validity and Test-Retest Reliability of Children's Hand-Use Experience Questionnaire in Children With Unilateral Cerebral PalsyDocument7 pagesValidity and Test-Retest Reliability of Children's Hand-Use Experience Questionnaire in Children With Unilateral Cerebral PalsyIsabela RéduaNo ratings yet
- Height and Its Relationship To Refraction and Biometry Parameters in Singapore Chinese ChildrenDocument6 pagesHeight and Its Relationship To Refraction and Biometry Parameters in Singapore Chinese ChildrenAngkat Prasetya Abdi NegaraNo ratings yet
- Axial Length StudyDocument8 pagesAxial Length StudyMαρία ΚολέδαNo ratings yet
- American JournalDocument7 pagesAmerican JournalCerro Alegre ValparaísoNo ratings yet
- Spina Bifida Grown UpDocument10 pagesSpina Bifida Grown UpDimple GoyalNo ratings yet
- Neema Rawat Microteaching (Spina Bifida)Document67 pagesNeema Rawat Microteaching (Spina Bifida)Dimple GoyalNo ratings yet
- Cerebrospinal Fluid Research: Needs Assessment of School-Going Children and Adolescents With Spina BifidaDocument1 pageCerebrospinal Fluid Research: Needs Assessment of School-Going Children and Adolescents With Spina BifidaDimple GoyalNo ratings yet
- WarmupandcooldownDocument6 pagesWarmupandcooldownDimple GoyalNo ratings yet
- Challenge - 50 Phrasal Verbs Challenge-MergedDocument20 pagesChallenge - 50 Phrasal Verbs Challenge-MergedSajalNo ratings yet
- Sample Paper 5 - E2 ReadingDocument8 pagesSample Paper 5 - E2 ReadingVic GascónNo ratings yet
- Data For FY2020 DCFS Children in Hospitals (Courtesy Charles Golbert)Document2 pagesData For FY2020 DCFS Children in Hospitals (Courtesy Charles Golbert)NewsTeam20No ratings yet
- Alat Ukur Parenting Self Efficacy English PDFDocument16 pagesAlat Ukur Parenting Self Efficacy English PDFZaufyVerliezaNo ratings yet
- Jade-Selena Currie: Personal InfoDocument1 pageJade-Selena Currie: Personal InfoarielleNo ratings yet
- The Physical DomainDocument9 pagesThe Physical DomainPatricia RiveraNo ratings yet
- Sudden Infant Death SyndromeDocument4 pagesSudden Infant Death SyndromeShohidul IslamNo ratings yet
- Attachment Workbook New 2015Document91 pagesAttachment Workbook New 2015Naomi UmoruNo ratings yet
- Percentile RankDocument8 pagesPercentile RankJohn Philip ReyesNo ratings yet
- Cambridge Think Test 10Document3 pagesCambridge Think Test 10IgaNo ratings yet
- NCM 109 Final Exams Part IIDocument3 pagesNCM 109 Final Exams Part IIsnay axieNo ratings yet
- Developmental PsychologyDocument77 pagesDevelopmental PsychologyArkan KhairullahNo ratings yet
- Music Activity PlanDocument4 pagesMusic Activity Planapi-506346106No ratings yet
- Inglés María MaríaDocument11 pagesInglés María MaríaPaola GarcíaNo ratings yet
- SANAYSAYDocument2 pagesSANAYSAYDinalyn RequinoNo ratings yet
- Socialization: Start UpDocument13 pagesSocialization: Start UpChristian Luis De GuzmanNo ratings yet
- Sylvestre - Child Maltreatment - 2016 PDFDocument12 pagesSylvestre - Child Maltreatment - 2016 PDFRoufaida GuessoumNo ratings yet
- Sharing Books With ToddlersDocument3 pagesSharing Books With ToddlersStephanie García EscobarNo ratings yet
- Safespaces - Leaflet PDFDocument24 pagesSafespaces - Leaflet PDFKidz to Adultz ExhibitionsNo ratings yet
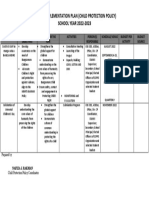
- Aip CPP 2022 2023Document1 pageAip CPP 2022 2023maamjuuNo ratings yet
- Discipline and BehaviorDocument2 pagesDiscipline and BehaviorInaM.ColetNo ratings yet
- Sleepy Students Perform WorseDocument2 pagesSleepy Students Perform WorseTriệu Mẫn Chi NguyễnNo ratings yet
- Script CPH LabDocument10 pagesScript CPH LabNichole MercedesNo ratings yet
- Halloween Should Be Spooky, Not Scary!Document2 pagesHalloween Should Be Spooky, Not Scary!NewsChannel 9No ratings yet
- Fostering Leaflet 2014Document12 pagesFostering Leaflet 2014bgtfNo ratings yet
- English StandardsDocument28 pagesEnglish StandardsSophie-Louise MercedesNo ratings yet
- KicktheButtcolouringbook VictorianAboriginalartforourlittledeadlyartists-FKBDocument24 pagesKicktheButtcolouringbook VictorianAboriginalartforourlittledeadlyartists-FKBAseel AllyNo ratings yet
- Introduction To Play TherapyDocument10 pagesIntroduction To Play TherapyJan Michael Suarez100% (1)