Download as pdf or txt
You might also like
- General Organic and Biochemistry Connecting Chemistry To Your Life Second Edition PDFDocument886 pagesGeneral Organic and Biochemistry Connecting Chemistry To Your Life Second Edition PDF12k6100% (6)
- As 2683-2000 Hose and Hose Assemblies For Distribution of Petroleum and Petroleum Products (Excepting LPG)Document7 pagesAs 2683-2000 Hose and Hose Assemblies For Distribution of Petroleum and Petroleum Products (Excepting LPG)SAI Global - APACNo ratings yet
- DR Kaleem Khan Assistant Professor JNMCHDocument63 pagesDR Kaleem Khan Assistant Professor JNMCHKaleem KhanNo ratings yet
- Urine Analysis PracticalDocument53 pagesUrine Analysis PracticalMubasharAbrar100% (3)
- Other Body FluidsDocument53 pagesOther Body FluidsletspreiiiNo ratings yet
- Antibacterial Activity of Wiregrass (Eleusine Indica) and Pandanus Specie Leaves Extract Against Escherichia ColiDocument28 pagesAntibacterial Activity of Wiregrass (Eleusine Indica) and Pandanus Specie Leaves Extract Against Escherichia ColiKristian Dave Diva100% (6)
- Synthesis of PolyamideDocument7 pagesSynthesis of PolyamideNg Seang Earn100% (2)
- ORGANIC POISONS - Doc PPXDocument29 pagesORGANIC POISONS - Doc PPXifrahnadeem393No ratings yet
- Classification of Poisons (According To Mode of Action)Document133 pagesClassification of Poisons (According To Mode of Action)dr rizwanNo ratings yet
- Carbolic Acid Poisoning: BY Thianeswar .I.S Ii MbbsDocument22 pagesCarbolic Acid Poisoning: BY Thianeswar .I.S Ii MbbsThianesh ty100% (2)
- Carbolic Acid & Oxalic AcidDocument46 pagesCarbolic Acid & Oxalic AcidImteaz ahamadNo ratings yet
- Corrosive PoisonsDocument33 pagesCorrosive PoisonsThank MubarakNo ratings yet
- 2 ToxicologyDocument18 pages2 Toxicologyنوف الحربي.No ratings yet
- Bleach PresentationDocument22 pagesBleach PresentationMohil PratapNo ratings yet
- Special ToxicologyDocument127 pagesSpecial ToxicologyNooria ButtNo ratings yet
- Carbolic AcidsDocument7 pagesCarbolic AcidsDr. Tahir MunirNo ratings yet
- Clinical Toxicology: Dr. Sura Al Zoubi Faculty of Medicine 31503203Document32 pagesClinical Toxicology: Dr. Sura Al Zoubi Faculty of Medicine 31503203Moutaz SH AmayrhNo ratings yet
- 2.physical ch. urine د.هناديDocument22 pages2.physical ch. urine د.هناديAbdulmalik Al-harthyNo ratings yet
- 2 AnticholinesterasesDocument55 pages2 AnticholinesterasesSudhakar LakavathNo ratings yet
- Urinalysis PDFDocument56 pagesUrinalysis PDFTio AjhaNo ratings yet
- AcidsDocument48 pagesAcidsDr.Sathish M SNo ratings yet
- Carbohydrate MetabolismDocument30 pagesCarbohydrate MetabolismDipak YogiNo ratings yet
- Rine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al MaqadmaDocument39 pagesRine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al Maqadmaiman zainuddin100% (1)
- Poisoning ?2Document31 pagesPoisoning ?2anusreesidharthanNo ratings yet
- Poisoning in Children: Prepared By, Gayathri R 2 Yr MSC (N)Document124 pagesPoisoning in Children: Prepared By, Gayathri R 2 Yr MSC (N)Gayathri RNo ratings yet
- Methyl AlcoholDocument29 pagesMethyl AlcoholRuchira NishshankaNo ratings yet
- Analysis of Abnormal UrineDocument12 pagesAnalysis of Abnormal Urinesingonstrings365No ratings yet
- Oxalic AcidDocument12 pagesOxalic AcidChandan Mahakud100% (1)
- Corrosives 1Document13 pagesCorrosives 1ShuvashishSunuwarNo ratings yet
- Organochloride Poisoning EditedDocument14 pagesOrganochloride Poisoning EditedSatyakiranNo ratings yet
- Carbolic AcidDocument5 pagesCarbolic AcidShuvashishSunuwarNo ratings yet
- CholeraDocument11 pagesCholeraElaine ZafeNo ratings yet
- Role of Mucokinetics in Respiratory Medicine: Dr. M.K.SharmaDocument55 pagesRole of Mucokinetics in Respiratory Medicine: Dr. M.K.Sharmaingrid_panturu5576No ratings yet
- Volatile PoisonsDocument23 pagesVolatile PoisonshaidaraalkhafajiNo ratings yet
- Cholera Mi Lecture MDocument35 pagesCholera Mi Lecture MJohnson OlawaleNo ratings yet
- UrinalysisDocument83 pagesUrinalysisJasneetaNo ratings yet
- Urine and Blood PPT (Handout Print Form) Chua, RDocument10 pagesUrine and Blood PPT (Handout Print Form) Chua, RKirsten Hazel Mejia100% (1)
- Horse ColicDocument66 pagesHorse ColicDr. Ghalib S. RidhaNo ratings yet
- Poisoning in ChildrenDocument44 pagesPoisoning in ChildrenYohanes FirmansyahNo ratings yet
- Op and Oc Comp ToxiDocument37 pagesOp and Oc Comp ToxiSRINIVASAN GnanasabapathyNo ratings yet
- VibrioDocument32 pagesVibrioVishnuKumarNo ratings yet
- Urine-Analysis 140420Document74 pagesUrine-Analysis 140420sabao kizuiteNo ratings yet
- Increasing The Elimination of Toxins in The BodyDocument33 pagesIncreasing The Elimination of Toxins in The BodyhllbakriNo ratings yet
- Urine AnalysisDocument28 pagesUrine Analysisomatre210No ratings yet
- Poisoning by Plants With Calcium Oxalate Crystals: Batch Number: 25 Group 1 Roll NumbersDocument19 pagesPoisoning by Plants With Calcium Oxalate Crystals: Batch Number: 25 Group 1 Roll NumbersJimmie ClassicNo ratings yet
- Gastric FluidDocument33 pagesGastric FluidJaellah MatawaNo ratings yet
- Urine AnalysisDocument33 pagesUrine AnalysisajaysomNo ratings yet
- Chloramphenicol: Prof DR Shah Murad 0314-2243415Document47 pagesChloramphenicol: Prof DR Shah Murad 0314-2243415PROF DR SHAHMURADNo ratings yet
- اليزيد UrinalysisDocument48 pagesاليزيد UrinalysisRa'aft Al-SamawiNo ratings yet
- Coorosive 22Document44 pagesCoorosive 22mohammaddammagNo ratings yet
- UrineDocument55 pagesUrineAbuzarNo ratings yet
- Changes in Composition of Urine Stored at Room TemperatureDocument39 pagesChanges in Composition of Urine Stored at Room TemperatureAjay SomeshwarNo ratings yet
- Carbon Monoxide Poisoning 4th YrDocument17 pagesCarbon Monoxide Poisoning 4th YrkhadzxNo ratings yet
- AlkaptonuriaDocument12 pagesAlkaptonuriaGirish Kishor PaiNo ratings yet
- Examination of Body Fluids (Urinalysis)Document109 pagesExamination of Body Fluids (Urinalysis)kiedd_04100% (9)
- بايو عملي م١Document5 pagesبايو عملي م١tm31880388No ratings yet
- Anti Gout: by Dr. Saba TariqDocument32 pagesAnti Gout: by Dr. Saba TariqDr. Saba TariqNo ratings yet
- Formation of Urine: NephronDocument44 pagesFormation of Urine: NephronajaysomNo ratings yet
- Alcohol ToxicityDocument81 pagesAlcohol ToxicityKarim RezaNo ratings yet
- Characteristics of UrineDocument32 pagesCharacteristics of UrineMEGHANA GOSWAMINo ratings yet
- Adi - IntoxicationDocument52 pagesAdi - IntoxicationAdi WidanaNo ratings yet
- The Slim Book of Health Pearls: Symptoms Never to IgnoreFrom EverandThe Slim Book of Health Pearls: Symptoms Never to IgnoreNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- HB 0934 002 1090331 HB QA Cador Pathogen Mini 1214 WWDocument40 pagesHB 0934 002 1090331 HB QA Cador Pathogen Mini 1214 WWcarlosNo ratings yet
- Material Selection in Oil and Gas 1684649857Document15 pagesMaterial Selection in Oil and Gas 1684649857Sh MNNo ratings yet
- Filtro Aceite SPORLAN OF-303Document2 pagesFiltro Aceite SPORLAN OF-303IDEA RefrisolICENo ratings yet
- Multi Pressure Vapour Compression Refrigeration SystemDocument11 pagesMulti Pressure Vapour Compression Refrigeration SystemDeepakNo ratings yet
- Const Safety Exe PlanDocument17 pagesConst Safety Exe PlanbbhattNo ratings yet
- Pesticides USAID DocumentDocument222 pagesPesticides USAID DocumentDinesh Runiwal100% (1)
- RM Phase - I Test Planner 2023-24Document12 pagesRM Phase - I Test Planner 2023-24arindamgiricontaiNo ratings yet
- Air Conditioning PDFDocument74 pagesAir Conditioning PDFDatu JonathanNo ratings yet
- 814 PDFDocument11 pages814 PDFBrijesh SharmaNo ratings yet
- Amir Toghyani A4 - Ei ArtikDocument98 pagesAmir Toghyani A4 - Ei ArtikfNo ratings yet
- Petrotest Product 13-0285 enDocument3 pagesPetrotest Product 13-0285 endchyNo ratings yet
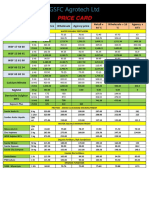
- Price CardDocument2 pagesPrice Cardvim patelNo ratings yet
- DS Granipan F30Document1 pageDS Granipan F30faridNo ratings yet
- MigDocument6 pagesMigPensel KoNtotNo ratings yet
- Ketoconazole Cream 1142Document2 pagesKetoconazole Cream 1142BSSNo ratings yet
- Extraction of Essential Oils Present in Aniseed (Saunf), Carum (Ajwain) and Cardamom (Ilaichi)Document16 pagesExtraction of Essential Oils Present in Aniseed (Saunf), Carum (Ajwain) and Cardamom (Ilaichi)suhani bansalNo ratings yet
- Piping Class Specification - CNE-001-2006-E-08-M-L-10126Document20 pagesPiping Class Specification - CNE-001-2006-E-08-M-L-10126Mubashir fareedNo ratings yet
- Humisteam X-Plus: User ManualDocument60 pagesHumisteam X-Plus: User Manualdencio0429No ratings yet
- ChitosanDocument4 pagesChitosanZalikha ZainiNo ratings yet
- 34 Samss 514 PDFDocument10 pages34 Samss 514 PDFprabaNo ratings yet
- Proposed Utilities Piping & Fittings of Soaps & Cometics PlantDocument1 pageProposed Utilities Piping & Fittings of Soaps & Cometics PlantLuigi Andrew MercadoNo ratings yet
- Research Project Data e LogbookDocument8 pagesResearch Project Data e LogbookEl John CalicaNo ratings yet
- Practice Set - 4Document2 pagesPractice Set - 4rishavkmNo ratings yet
- STPM Biology Past Year QuestionDocument8 pagesSTPM Biology Past Year QuestionMc Donalds Ohl Ohlsen100% (2)
- Hazardous WasteDocument32 pagesHazardous WasteDavid Banda MbazumaNo ratings yet
- Index - 8.8 Eu PharmDocument56 pagesIndex - 8.8 Eu PharmAnonymous iOYpj92No ratings yet