Download as pdf or txt
You might also like
- Nursing Test 4 (NP Iii)Document16 pagesNursing Test 4 (NP Iii)Yuxin Liu100% (2)
- PCOL - Chapter 11 - Anti Hypertensive AgentsDocument3 pagesPCOL - Chapter 11 - Anti Hypertensive AgentsCharles BayogNo ratings yet
- Fluid, Electrolyte, and Acid-Base Disorders Robert B Schonberger 2018Document18 pagesFluid, Electrolyte, and Acid-Base Disorders Robert B Schonberger 2018Akhmad Fadhiel Noor100% (1)
- Hospital DischargeDocument15 pagesHospital DischargePrernaBhasinNo ratings yet
- Pharmacology Drug ClassificationDocument4 pagesPharmacology Drug ClassificationRPh Krishna Chandra Jagrit100% (4)
- Anoosha Roll#21Document19 pagesAnoosha Roll#21Anusha ZubairNo ratings yet
- Antianginal DrugsDocument19 pagesAntianginal DrugsAnusha ZubairNo ratings yet
- Lecture 24-25 - Antihypertensive AgentsDocument30 pagesLecture 24-25 - Antihypertensive AgentsJedoNo ratings yet
- CVS PharmacologyDocument60 pagesCVS PharmacologyGølà Sèèñàà–baale irraaNo ratings yet
- 10 and 11 Treatment of Hypertension and AnginaDocument10 pages10 and 11 Treatment of Hypertension and AnginaBrandon AviciiNo ratings yet
- 10-11 Treatment of HypertensionDocument11 pages10-11 Treatment of HypertensionHanif GandohNo ratings yet
- Pharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Document23 pagesPharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Nandraj123100% (1)
- Antihypertensives 2Document6 pagesAntihypertensives 2Manyal Kutin KoakNo ratings yet
- Antihypertensive AgentsDocument41 pagesAntihypertensive AgentsRwapembe StephenNo ratings yet
- HTN JmiDocument39 pagesHTN Jmink999999No ratings yet
- Antihypertensive DrugsDocument5 pagesAntihypertensive DrugsAiman TymerNo ratings yet
- Antihypertensives WMDocument16 pagesAntihypertensives WMALNAKINo ratings yet
- Antihypertensive Drugs (2) - 092019Document33 pagesAntihypertensive Drugs (2) - 092019muntadhar5000No ratings yet
- Anti HypertensivesDocument21 pagesAnti HypertensivesDivya RanasariaNo ratings yet
- AntihipertensiDocument39 pagesAntihipertensiHarri HardiNo ratings yet
- Anti HypertensivesDocument23 pagesAnti HypertensivesLeena AlateeqNo ratings yet
- Antihypertensive & Antianginal DrugsDocument5 pagesAntihypertensive & Antianginal Drugsdomememe1No ratings yet
- Heat Failure DrugsDocument8 pagesHeat Failure DrugsDaniel MwiluNo ratings yet
- Vasodilators 1233318450814478 3Document29 pagesVasodilators 1233318450814478 3Nehal AmjadNo ratings yet
- Anti Hypertensive 20191211Document35 pagesAnti Hypertensive 20191211helloitsmenadNo ratings yet
- Ishac M2 Cardio Antihypertensives 2010Document16 pagesIshac M2 Cardio Antihypertensives 2010Franchesca LugoNo ratings yet
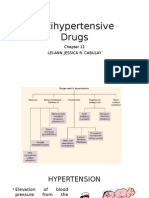
- Antihypertensive DrugsDocument37 pagesAntihypertensive Drugsleiann_jessicaNo ratings yet
- HypertensionDocument54 pagesHypertensionBadri KarkiNo ratings yet
- Antihypertensive Drugs.Document35 pagesAntihypertensive Drugs.Abdul WahabNo ratings yet
- Lec 22 ANTIHYPERTENSIVE - 2Document22 pagesLec 22 ANTIHYPERTENSIVE - 2Abdul MananNo ratings yet
- 1 Antihypertensive DrugsDocument14 pages1 Antihypertensive DrugsReda SoNo ratings yet
- Anti HypretensivesDocument18 pagesAnti HypretensivesLeena AlateeqNo ratings yet
- Anti HypretensivesDocument18 pagesAnti HypretensivesLeena AlateeqNo ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- Hypertension TejaDocument64 pagesHypertension TejaAnushka MaheshwariNo ratings yet
- CVD and HTNDocument60 pagesCVD and HTNZsazsa100% (1)
- M. Gabriel Khan - Cardiac Drug Therapy, Calcium Channel BlockersDocument21 pagesM. Gabriel Khan - Cardiac Drug Therapy, Calcium Channel BlockersluongcongthucNo ratings yet
- AntihypertensiveDocument94 pagesAntihypertensiveadityarupusrikantaNo ratings yet
- HipertensiDocument37 pagesHipertensiIrna Purwanti RahayuNo ratings yet
- Antihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityDocument71 pagesAntihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityMoonAIRNo ratings yet
- PRB VasodilatorsDocument20 pagesPRB VasodilatorsHUZAIFA YAMAANNo ratings yet
- Anti Hypertensive DrugsDocument46 pagesAnti Hypertensive DrugsShabaka KashataNo ratings yet
- ObjectivesDocument39 pagesObjectiveskiranstNo ratings yet
- Antihypertensive Drugs: HypertensionDocument8 pagesAntihypertensive Drugs: Hypertensionalmastar officeNo ratings yet
- Antihypertensive AgentsDocument52 pagesAntihypertensive Agentssameena ramzanNo ratings yet
- CVS & Hypolipidemic Drugs-NursingDocument71 pagesCVS & Hypolipidemic Drugs-NursingManikanta Guptha100% (1)
- Study Guide For Final Pharmacology HypertensionDocument39 pagesStudy Guide For Final Pharmacology HypertensionAlejandro Daniel Landa MoralesNo ratings yet
- Antihypertensive DrugsDocument7 pagesAntihypertensive Drugshamadadodo7No ratings yet
- HYPERTENSIONDocument5 pagesHYPERTENSIONRajesh RamanNo ratings yet
- Antihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarDocument52 pagesAntihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarASHUTOSH KHADANGANo ratings yet
- ACE InhibitorsDocument25 pagesACE InhibitorsShihab AlmoliukiNo ratings yet
- HypertensionDocument85 pagesHypertensionmelkamu AssefaNo ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- Cardiovascular PharmacologyDocument61 pagesCardiovascular PharmacologyTeeOne920% (1)
- AntiHypertensives (Autosaved)Document64 pagesAntiHypertensives (Autosaved)UsamaNo ratings yet
- Antihypertensive Agents Saitoti SDocument50 pagesAntihypertensive Agents Saitoti SMusa yohanaNo ratings yet
- Cholinergic System: e CarbamatesDocument26 pagesCholinergic System: e CarbamatesAcai BoncaiNo ratings yet
- Drugs Used To Treat Cardiovascular Diseases: HypertensionDocument35 pagesDrugs Used To Treat Cardiovascular Diseases: HypertensionAyro Business CenterNo ratings yet
- SYMPATHOLOGICSDocument14 pagesSYMPATHOLOGICSLuiza Mae CastroNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- Mudra VigyanDocument13 pagesMudra VigyanYeathy Raj K NaiduNo ratings yet
- Chronic Disease BurdenDocument2 pagesChronic Disease BurdenjcfloreshNo ratings yet
- Lippincott's PEDIATRIC3 ANSWERSDocument8 pagesLippincott's PEDIATRIC3 ANSWERSNursyNurseNo ratings yet
- Stem Cells Notes - BIO SUmmDocument3 pagesStem Cells Notes - BIO SUmmMuffaddal MustafaNo ratings yet
- Filarial NematodeDocument18 pagesFilarial NematodeHawre NajmaddinNo ratings yet
- 1 SMDocument6 pages1 SMedi_wsNo ratings yet
- Comparative Anatomy of Circulation in Annelid, Arthopoda and MolluscsDocument4 pagesComparative Anatomy of Circulation in Annelid, Arthopoda and MolluscsNarasimha MurthyNo ratings yet
- Epidemiology of Premenstrual Syndrome (PMS) - A Systematic Review and Meta-Analysis StudyDocument4 pagesEpidemiology of Premenstrual Syndrome (PMS) - A Systematic Review and Meta-Analysis StudyPhong Triệu LêNo ratings yet
- WHO International Bibliography of KMCDocument84 pagesWHO International Bibliography of KMCSapna thakurNo ratings yet
- Urine Collection: Collecting A Clean Catch UrineDocument5 pagesUrine Collection: Collecting A Clean Catch UrineAngelene CalivaNo ratings yet
- Leishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal MedicineDocument20 pagesLeishmaniasis: Dr. Kazi Shihab Uddin Mbbs MRCP (Uk) Associate Professor & HOD Department of Internal MedicineSHIHAB UDDIN KAZINo ratings yet
- MPPC Health Indeminity FormDocument2 pagesMPPC Health Indeminity FormmichaelforkcsNo ratings yet
- Manual, Blood CultureDocument41 pagesManual, Blood CultureFilipus HendiantoNo ratings yet
- Med SurgDocument5 pagesMed SurgSherilNo ratings yet
- Jurnal Penatalaksanaan EdemaDocument7 pagesJurnal Penatalaksanaan EdemaMariska Nada Debora100% (1)
- Mapeh 2Document11 pagesMapeh 2Aira Khay MapoteNo ratings yet
- 5 6212862165817229365Document116 pages5 6212862165817229365badhra100% (1)
- Pengantar HemostasisDocument12 pagesPengantar HemostasisPretty AngeliaNo ratings yet
- Blaylock RSM 2002Document359 pagesBlaylock RSM 2002marvel007No ratings yet
- Post TaskDocument2 pagesPost Taskbing bongNo ratings yet
- Iv PrimingDocument16 pagesIv PrimingZahra jane A.No ratings yet
- SYPHILIS (103 To 108) PPT - PPTX - 20230906 - 161225 - 0000Document15 pagesSYPHILIS (103 To 108) PPT - PPTX - 20230906 - 161225 - 0000Aaditya GadhviNo ratings yet
- OXYTOCINDocument1 pageOXYTOCINBernardNo ratings yet
- Notes of 2020Document90 pagesNotes of 2020eolhc rezarf100% (1)
- Final Results Report: Curative Labs Inc. 3330 New York Ave NE Washington, DC 20002Document1 pageFinal Results Report: Curative Labs Inc. 3330 New York Ave NE Washington, DC 20002Aidan NicholsNo ratings yet
- Presentation On: Kgmu College of NursingDocument42 pagesPresentation On: Kgmu College of NursingSweety YadavNo ratings yet