Download as pdf or txt
You might also like
- Respiratory CaseDocument5 pagesRespiratory CaseChristina Listha0% (2)
- NCP 1 N 2Document5 pagesNCP 1 N 2Cuttie Anne GalangNo ratings yet
- Case PresentationDocument5 pagesCase PresentationJARIETTA OCHOANo ratings yet
- NCP For Impaired Gas ExchangeDocument2 pagesNCP For Impaired Gas ExchangeSweetie Star94% (16)
- Chest Fisioterapy in BronchiektasisDocument11 pagesChest Fisioterapy in BronchiektasisKhalila DiantiNo ratings yet
- 4759 PDFDocument9 pages4759 PDFamitjustamitNo ratings yet
- Coding Data Worksheet - Spring 2021 1Document2 pagesCoding Data Worksheet - Spring 2021 1api-548217720No ratings yet
- Icu 2Document9 pagesIcu 2GemilleDaphneAndradaNo ratings yet
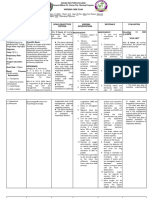
- Assessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: IndependentDocument4 pagesAssessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: IndependentAlyssa Marie SantosNo ratings yet
- Pulmonary Embol-WPS OfficeDocument49 pagesPulmonary Embol-WPS OfficeBryan BuendiaNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaNo ratings yet
- Bernadas NCPDocument3 pagesBernadas NCPBernadas, Jhon Kristopher C.No ratings yet
- Assessmen 1Document2 pagesAssessmen 1jana manaloNo ratings yet
- NCP Impaired Gas ExchangeDocument2 pagesNCP Impaired Gas ExchangeGabriel Tolentino70% (10)
- Diana Kyla A. Punay Bsn-Dash-6: Subjective Data: Short Term: Short TermDocument3 pagesDiana Kyla A. Punay Bsn-Dash-6: Subjective Data: Short Term: Short TermZoè AshtrönNo ratings yet
- NCP - Or-Rotation 2Document12 pagesNCP - Or-Rotation 2Vian RiveraNo ratings yet
- NCP Difficulties in BreathingDocument4 pagesNCP Difficulties in BreathingKingJayson Pacman06No ratings yet
- Assessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveDocument6 pagesAssessment Nursing Diagnosis Planning Nsg. Intervention Rationale Evaluation SubjectiveIngrid Eunice ConcordiaNo ratings yet
- Nursing Care Plan: Assessement Diagnosis Goals and Desired Outcomes Nursing Intervention Implementation EvaluationDocument1 pageNursing Care Plan: Assessement Diagnosis Goals and Desired Outcomes Nursing Intervention Implementation EvaluationJoshua Selwyn SalazarNo ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument9 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluationclydell joyce masiarNo ratings yet
- Final NCP (Jannel)Document6 pagesFinal NCP (Jannel)Zed P. EstalillaNo ratings yet
- Elena Ocyo (Pedia - NCP)Document3 pagesElena Ocyo (Pedia - NCP)elle leliNo ratings yet
- Name: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaDocument3 pagesName: Mr. M AGE: 62 Years Old SEX: Male CC: Persistent Cough Admitting/Working Diagnosis: PnuemoniaMae Therese B. MAGNONo ratings yet
- CKD Case 2Document16 pagesCKD Case 2Arabylle Maranca AbuelNo ratings yet
- Excess or Deficit in Oxygenation And/or Carbon Dioxide Elimination at The Alveolar-Capillary MembraneDocument6 pagesExcess or Deficit in Oxygenation And/or Carbon Dioxide Elimination at The Alveolar-Capillary MembraneHazel MiraranNo ratings yet
- Vital Signs Taken As FollowsDocument10 pagesVital Signs Taken As FollowsKyle AndrewNo ratings yet
- Cap No GraphyDocument37 pagesCap No GraphyLeypotNo ratings yet
- NURSING CARE PLAN Alvarez - Impaired Gas ExchangeDocument2 pagesNURSING CARE PLAN Alvarez - Impaired Gas ExchangeNader AbdurasadNo ratings yet
- NCP DR WardDocument5 pagesNCP DR WardLyza MateoNo ratings yet
- NCP Acute BrochitisDocument5 pagesNCP Acute BrochitisFrancine kimberlyNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationBianca Mikaela DosdosNo ratings yet
- NCP and Drug StudyDocument7 pagesNCP and Drug StudyKirsty Marie SupranesNo ratings yet
- Hashim Clinical Log 3Document10 pagesHashim Clinical Log 3Hashim AlsammawiNo ratings yet
- Name: Zeph Age: 23 Years Old Sex: Male Room Number: 304 Hospital Number: 100921Document2 pagesName: Zeph Age: 23 Years Old Sex: Male Room Number: 304 Hospital Number: 100921kuro hanabusaNo ratings yet
- Concept MapDocument1 pageConcept Mapapi-636490948No ratings yet
- Nursing Care Plan On Community-Acquired PneumoniaDocument3 pagesNursing Care Plan On Community-Acquired Pneumoniabeatrice angelineNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationJustine Mae A. LoriaNo ratings yet
- Assessment Planning Intervention Rationale Evaluation: Mechanism of ActionDocument2 pagesAssessment Planning Intervention Rationale Evaluation: Mechanism of ActionNicole CalpoturaNo ratings yet
- Ventilatory Assistance Case Study - Case Study Assignment v.2Document3 pagesVentilatory Assistance Case Study - Case Study Assignment v.2j dogNo ratings yet
- Basics of Mechanical Ventilation (SIPHW)Document68 pagesBasics of Mechanical Ventilation (SIPHW)Sudip beraNo ratings yet
- Emphysema NCPDocument5 pagesEmphysema NCPAbegail Bautista DoriaNo ratings yet
- Nursing Care Plan AnemiaDocument3 pagesNursing Care Plan AnemiaNat B. AntipoloNo ratings yet
- Mechanical VentilationDocument13 pagesMechanical VentilationNithiya NadesanNo ratings yet
- NCP BauanDocument2 pagesNCP BauanJoedelynne Diane Endaya GarciaNo ratings yet
- NCP FinalDocument16 pagesNCP FinalEuleen Tria PadrigoNo ratings yet
- Ineffective Airway ClearanceDocument1 pageIneffective Airway ClearanceFreisanChenMandumotanNo ratings yet
- Pulmonary and Critical Care MedicineDocument33 pagesPulmonary and Critical Care MedicineVh TRNo ratings yet
- Case AnalysisDocument11 pagesCase AnalysisCZAR VINCENT WAYNE SEVANDAL BAYLONNo ratings yet
- Name: L.J.A AGE: 20 Years Old SEX: Male CC: Cough and DOB Admitting/Working Diagnosis: AsthmaDocument2 pagesName: L.J.A AGE: 20 Years Old SEX: Male CC: Cough and DOB Admitting/Working Diagnosis: AsthmaMae Therese B. MAGNONo ratings yet
- Respiratory Physiology: Ventilation Perfusion DiffusionDocument6 pagesRespiratory Physiology: Ventilation Perfusion DiffusionShiara Ruth EdrosoloNo ratings yet
- Pulmo ImDocument7 pagesPulmo ImCathy SolivarNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- NCP, KentDocument2 pagesNCP, KentKent JuguilonNo ratings yet
- Braga, Patricia 4B (NCM 118)Document4 pagesBraga, Patricia 4B (NCM 118)Jessica BragaNo ratings yet
- Therapeutic AssignmentDocument4 pagesTherapeutic AssignmentSylvester WasongaNo ratings yet
- Ch20 - PostoperativeDocument18 pagesCh20 - PostoperativeAbel C. Idusma Jr.No ratings yet
- T Thomas Acute Care Practicum 3-28-14Document2 pagesT Thomas Acute Care Practicum 3-28-14api-283689862No ratings yet
- LP Penyakit Dyspnea AmelDocument11 pagesLP Penyakit Dyspnea AmelAmilia Dwi IndrawatiNo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Questions and Answers in Small Animal AnesthesiaFrom EverandQuestions and Answers in Small Animal AnesthesiaLesley J. SmithNo ratings yet
- Astm D 4258Document2 pagesAstm D 4258anthonybarnard100% (1)
- Métodos de Violín y ViolaDocument10 pagesMétodos de Violín y ViolaMaria de los Ángeles50% (2)
- Colors and Effects - PSG Pigment Preparations PolyolefinsDocument24 pagesColors and Effects - PSG Pigment Preparations PolyolefinsBoonyarit LurdgrienggraiyingNo ratings yet
- Mistral: DehumidifierDocument16 pagesMistral: DehumidifierAntreprenor XNo ratings yet
- Weekly Meal Planner TemplateDocument11 pagesWeekly Meal Planner TemplateAshok JagtapNo ratings yet
- Vincent Van GoghDocument6 pagesVincent Van Goghfrancy sharonNo ratings yet
- A Proposal On Reusable Sanitary PADSDocument16 pagesA Proposal On Reusable Sanitary PADSMike AbbeyNo ratings yet
- Viking Johnson Dismantling Joint+BrochureDocument13 pagesViking Johnson Dismantling Joint+BrochureecocadecNo ratings yet
- TDS - Emaco R907 PlusDocument2 pagesTDS - Emaco R907 PlusVenkata RaoNo ratings yet
- Final Report.Document48 pagesFinal Report.Arjun Singh ANo ratings yet
- 2018 Resume NVDocument1 page2018 Resume NVcourtney willsonNo ratings yet
- Cheatsheet Gimp-Letter PDFDocument1 pageCheatsheet Gimp-Letter PDFRox DiazNo ratings yet
- Semantic Segmentation Data Labelling: Classes and InstructionsDocument9 pagesSemantic Segmentation Data Labelling: Classes and InstructionsMar FieldsNo ratings yet
- ACCA P1 Study Guide OpenTuitionDocument4 pagesACCA P1 Study Guide OpenTuitionalauddinaloNo ratings yet
- ChalukyanDocument44 pagesChalukyannimisha jainNo ratings yet
- Big Picture B: Unit 3Document4 pagesBig Picture B: Unit 3vworldpeace yanibNo ratings yet
- Hands On 3.1 ActDocument7 pagesHands On 3.1 Actmarkkyle collantesNo ratings yet
- Al Tronic Ill-Cpu Medium Engines, 2 16 Cylinders Service Instructions FORM Alii-CPU SL 4-91Document8 pagesAl Tronic Ill-Cpu Medium Engines, 2 16 Cylinders Service Instructions FORM Alii-CPU SL 4-91SMcNo ratings yet
- Torque Spiral Wound GSKT TableDocument2 pagesTorque Spiral Wound GSKT TableCarlos Roberto Tamariz100% (1)
- ProposalDocument15 pagesProposalCourage JuwawoNo ratings yet
- QuickRide LogcatDocument179 pagesQuickRide Logcatap131096No ratings yet
- Technicall Specification of 630 KVA, 11-0.415 KV Dry Type Outdoor Transformers.......... Dated. 31.08.2015Document25 pagesTechnicall Specification of 630 KVA, 11-0.415 KV Dry Type Outdoor Transformers.......... Dated. 31.08.2015spidervinoNo ratings yet
- The Classical Theory of Organization and Its Relevance - IRJFE - 41 - 06Document8 pagesThe Classical Theory of Organization and Its Relevance - IRJFE - 41 - 06coxshulerNo ratings yet
- Samsung LN46D550K1FXZA Fast Track Guide (SM)Document4 pagesSamsung LN46D550K1FXZA Fast Track Guide (SM)Carlos OdilonNo ratings yet
- Timothy StainbrookDocument1 pageTimothy Stainbrookapi-548131304No ratings yet
- Asian School Change in Profit Sharing Ratio Sample PaperDocument2 pagesAsian School Change in Profit Sharing Ratio Sample PaperMan your voice is breaking kuttyNo ratings yet
- Correction Level 5Document9 pagesCorrection Level 5nika wikaNo ratings yet
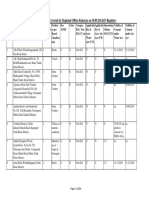
- List of Organisations Covered by Regional Office-Kolar (As On 30.09.2014) (F-Register)Document284 pagesList of Organisations Covered by Regional Office-Kolar (As On 30.09.2014) (F-Register)mutton moonswamiNo ratings yet