
Hemovigilance - 2012 - de Vries - APPENDIX B Proposed Standard Definitions For Surveillance of Non Infectious Adverse
Hemovigilance - 2012 - de Vries - APPENDIX B Proposed Standard Definitions For Surveillance of Non Infectious Adverse
You might also like
- Referat (PPT) - Hiperleukositosis & LeukostasisDocument16 pagesReferat (PPT) - Hiperleukositosis & LeukostasisShapira alNo ratings yet
- Guideline For Hemorrhagic ShockDocument8 pagesGuideline For Hemorrhagic ShockMikaGieJergoLarizaNo ratings yet
- Bloody Easy Coagulation SimplifiedDocument24 pagesBloody Easy Coagulation SimplifiedIlyasHasanNo ratings yet
- Definition of Transfusion ReactionDocument26 pagesDefinition of Transfusion ReactionAlvin A. AldeaNo ratings yet
- Adverse Effects of Blood Transfusion: 6 EditionDocument32 pagesAdverse Effects of Blood Transfusion: 6 EditionKaycee Gretz Loresca100% (1)
- Hemovigilancia ISBT 2011Document12 pagesHemovigilancia ISBT 2011Leonardo Borges dos SantosNo ratings yet
- Transfusion ReactionDocument66 pagesTransfusion ReactionAbhineet SalveNo ratings yet
- Serious Transfusion Incident Report 2015 16 PD PDFDocument57 pagesSerious Transfusion Incident Report 2015 16 PD PDFje zhNo ratings yet
- Paciente Que Sangra - Trastornos Hemorrágicos Adquiridos 2020Document9 pagesPaciente Que Sangra - Trastornos Hemorrágicos Adquiridos 202090STRATOVARIUS90No ratings yet
- TransfusiónDocument5 pagesTransfusiónMayra Alejandra Prada SerranoNo ratings yet
- Reactii PostransfuzionaleDocument11 pagesReactii PostransfuzionaleDenisa BrihanNo ratings yet
- Informed Consent - StatPearls - NCBI BookshelfDocument7 pagesInformed Consent - StatPearls - NCBI BookshelfShashank ShekharNo ratings yet
- Transfusion ReactionsDocument36 pagesTransfusion Reactionsmarky203No ratings yet
- Prevention of Adverse ReactionsDocument15 pagesPrevention of Adverse Reactionscupuwatie cahyaniNo ratings yet
- Hazards of Blood TransfusionDocument9 pagesHazards of Blood TransfusionMaria Leslie FernandezNo ratings yet
- Investigation of FMH by Flow CytometryDocument15 pagesInvestigation of FMH by Flow CytometryMohammed Khair BashirNo ratings yet
- Cancer Guide Oncologic EmergenciesDocument22 pagesCancer Guide Oncologic EmergenciesHerrera MiguelNo ratings yet
- Complications of Blood TransfusionDocument7 pagesComplications of Blood TransfusionChandan SrivastavaNo ratings yet
- 10 1016@j Transci 2020 103015Document4 pages10 1016@j Transci 2020 1030152mf2hgjrj9No ratings yet
- Guidelines On The Use of Intravenous Immune Globulin For Hematologic ConditionsDocument48 pagesGuidelines On The Use of Intravenous Immune Globulin For Hematologic ConditionssarahulfaaNo ratings yet
- Tipe Reaksi TransfusiDocument9 pagesTipe Reaksi TransfusiRangga Raditya RanggaNo ratings yet
- Blood Transfusion Reactions-A Comprehensive Review of The Literature Including A Swiss PerspectiveDocument19 pagesBlood Transfusion Reactions-A Comprehensive Review of The Literature Including A Swiss Perspectivecesarsamp2No ratings yet
- Dic 1Document6 pagesDic 1Sandra Lusi NovitaNo ratings yet
- Acute Transfusion Reactions Nov15Document16 pagesAcute Transfusion Reactions Nov15Toto ZazNo ratings yet
- Understanding Disseminated Intravascular Coagulation (DIC)Document40 pagesUnderstanding Disseminated Intravascular Coagulation (DIC)Denise135No ratings yet
- Blood Transfusion Error Prevention - Nurses RoleDocument5 pagesBlood Transfusion Error Prevention - Nurses RoleLorenn AdarnaNo ratings yet
- Martin 2016Document12 pagesMartin 2016rositha prabandariNo ratings yet
- Affiliate InstitutionsDocument10 pagesAffiliate Institutionspopov357No ratings yet
- HIV MedscapeDocument60 pagesHIV MedscapeInfinitiiiNo ratings yet
- Dengue Fever by Prof M Ali KhanDocument36 pagesDengue Fever by Prof M Ali KhanVina MuspitaNo ratings yet
- Dengue Fever by Prof M Ali KhanDocument36 pagesDengue Fever by Prof M Ali Khanmaha rNo ratings yet
- Hematology NotesDocument32 pagesHematology NotesbrittaNo ratings yet
- Blood Transfusion Reactions Revisited Dr. Edwin RodriguezDocument99 pagesBlood Transfusion Reactions Revisited Dr. Edwin RodriguezBeng AquinoNo ratings yet
- Sepsis Cap 44 Cirugía GeneralDocument14 pagesSepsis Cap 44 Cirugía GeneralKarla Montserrat González MuroNo ratings yet
- JIFCC Lab Tests Interpretation 2018Document8 pagesJIFCC Lab Tests Interpretation 2018Abdul Sattar100% (1)
- Dengue DOHDocument16 pagesDengue DOHGehlatin Tumanan100% (1)
- Probleme La TransfuziiDocument6 pagesProbleme La TransfuziiAdina TîrnoveanuNo ratings yet
- A Ciegas - Josh MalermanDocument6 pagesA Ciegas - Josh MalermanRooyValenciaNo ratings yet
- DR Zalina - Trafusion Reaction and Management PDFDocument77 pagesDR Zalina - Trafusion Reaction and Management PDFvasu_5iveNo ratings yet
- Jurnal Pengambilan Darah Vena PDFDocument10 pagesJurnal Pengambilan Darah Vena PDFfebriyankusumoningrum100% (1)
- Diagnosis FluidDocument14 pagesDiagnosis FluidCristianMP96No ratings yet
- Disseminated Intravascular Coagulation and Implications For Medical-Surgical NursesDocument5 pagesDisseminated Intravascular Coagulation and Implications For Medical-Surgical Nursesancours100% (1)
- Dengue Fever by Prof M Ali KhanDocument36 pagesDengue Fever by Prof M Ali KhanAnonymous uGbcVSJTDgNo ratings yet
- Haemodialysis With On-Line Monitoring EquipmentDocument12 pagesHaemodialysis With On-Line Monitoring EquipmentConnie Alva GutierrezNo ratings yet
- Ascorbic Acid NCPDocument8 pagesAscorbic Acid NCPJohann OrtizNo ratings yet
- JBB2012 151967Document13 pagesJBB2012 151967Prodia Central Java RegionNo ratings yet
- AdsasdadsaDocument252 pagesAdsasdadsaAmitShettyNo ratings yet
- NP40126 SaeDocument9 pagesNP40126 SaeMohd AljawfiNo ratings yet
- Otolaryngol - Head Neck Surg - 2014 - Al Khatib - Severe Vitamin D DeficiencyDocument8 pagesOtolaryngol - Head Neck Surg - 2014 - Al Khatib - Severe Vitamin D Deficiencyrohillak692No ratings yet
- Koate DVIDocument7 pagesKoate DVIagnesroNo ratings yet
- BT ReactionDocument8 pagesBT ReactionMary Elijah Jane PopesNo ratings yet
- IC Guidance For Preventing and Controlling Blood-Borne Virus Infection in Haemo Units Feb 10Document10 pagesIC Guidance For Preventing and Controlling Blood-Borne Virus Infection in Haemo Units Feb 10Slavica Gjurceska-GorjanskaNo ratings yet
- How Should We Use Convalescent Plasma Therapies For The Management of COVID-19?Document9 pagesHow Should We Use Convalescent Plasma Therapies For The Management of COVID-19?Asep tepiyanaNo ratings yet
- Hypovolemic Shock Guidelines PDFDocument8 pagesHypovolemic Shock Guidelines PDFAloysia Catur WidiNo ratings yet
- Emorrhagic Hock: Sogc Clinical Practice GuidelinesDocument8 pagesEmorrhagic Hock: Sogc Clinical Practice GuidelinesraysellaNo ratings yet
- Cpm15th Dengue Fever (Doh)Document18 pagesCpm15th Dengue Fever (Doh)Marko ParungoNo ratings yet
- Lab Technologist 11Document43 pagesLab Technologist 11AHAMED SHIFAANNo ratings yet
- Blood Transfusion ReactionsDocument3 pagesBlood Transfusion ReactionsANDREW MWITINo ratings yet
- Sepsis Diagnosis and Monitoring: Fast Early ReliableDocument24 pagesSepsis Diagnosis and Monitoring: Fast Early ReliableI Nyoman Gede Semarajana100% (1)
- Hemophilia and Hemostasis: A Case-Based Approach to ManagementFrom EverandHemophilia and Hemostasis: A Case-Based Approach to ManagementAlice D. MaNo ratings yet
- Physical Characteristics and VolumeDocument10 pagesPhysical Characteristics and Volumedeepika kushwahNo ratings yet
- 58-File Utama Naskah-62-1-10-20200928Document8 pages58-File Utama Naskah-62-1-10-20200928Alfaera Rahma FarestyNo ratings yet
- Jose, Ruth Domingo 2201022290Document5 pagesJose, Ruth Domingo 2201022290xveniaNo ratings yet
- Status Note On Blood SafetyDocument9 pagesStatus Note On Blood SafetyAlbin Prince John0% (1)
- Hemophilia in ChildrenDocument6 pagesHemophilia in Childrensimina intunericNo ratings yet
- IdmDocument46 pagesIdmht8zwk946sNo ratings yet
- Evoluºia I Tratamentul În Sindromul Hemolitic-Uremic La CopilDocument6 pagesEvoluºia I Tratamentul În Sindromul Hemolitic-Uremic La CopilAntonia GenesNo ratings yet
- 782Document20 pages782Aarathi raoNo ratings yet
- PRP Therapy Kit MainDocument1 pagePRP Therapy Kit Maindrsuryakant9818No ratings yet
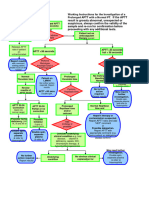
- Working Instructions Investigation of Prolonged APTTDocument1 pageWorking Instructions Investigation of Prolonged APTTtadeariba1No ratings yet
- Iso ImmunizationDocument3 pagesIso ImmunizationHazel Marie EchavezNo ratings yet
- A Study On The Role of in in Haemolytic Disease of The NewbornDocument9 pagesA Study On The Role of in in Haemolytic Disease of The Newbornaymona2000No ratings yet
- Rehman Medical Institute: Test Result Unit Reference ValuesDocument1 pageRehman Medical Institute: Test Result Unit Reference ValuesfahadbasahirNo ratings yet
- 2 Labs Cheat Sheets Nurse NationDocument2 pages2 Labs Cheat Sheets Nurse NationkNo ratings yet
- Strategi Diagnosis AnemiaDocument49 pagesStrategi Diagnosis Anemianiniek yusidaNo ratings yet
- Experiment Number 3 Sample Preparation For Blood Banking ProcedureDocument10 pagesExperiment Number 3 Sample Preparation For Blood Banking ProcedureKriziaNo ratings yet
- Fullpapers IJCPML 12-3-08Document4 pagesFullpapers IJCPML 12-3-08ryanNo ratings yet
- Feline Blood TransfusionDocument4 pagesFeline Blood TransfusionPhilipsNo ratings yet
- ABO Blood Group System NotesDocument45 pagesABO Blood Group System NotesAnne Carmel Verano100% (1)
- Erythrocyte Sedimentation Rate: Hematology 1 ReportDocument18 pagesErythrocyte Sedimentation Rate: Hematology 1 ReportNico LokoNo ratings yet
- Management of Blood Donors and Blood Donations From Individuals Found To Have A Positive Direct Antiglobulin TestDocument11 pagesManagement of Blood Donors and Blood Donations From Individuals Found To Have A Positive Direct Antiglobulin TestLuis Enrique Tinoco JuradoNo ratings yet
- 2021 ISFM Consensus Guidelines On The Collection and Administration of Blood and Blood Products in CatsDocument23 pages2021 ISFM Consensus Guidelines On The Collection and Administration of Blood and Blood Products in CatsNurul Izzatul AnnisaNo ratings yet
- BCM 20 Ultra NewDocument11 pagesBCM 20 Ultra NewWessamNo ratings yet
- Pathway HiperbilirubinDocument1 pagePathway HiperbilirubinHendri Ty100% (1)
- Iron Defisience AnemiaDocument61 pagesIron Defisience AnemiaYeni Jesika SilitongaNo ratings yet
- WarfarinDocument2 pagesWarfarinWAHYU NOFANDARI HERDIYANTINo ratings yet
- Hemophilia in ChildrenDocument16 pagesHemophilia in ChildrenVinay Sahu100% (1)
- Fu Mcu 12102022Document12 pagesFu Mcu 12102022anggaNo ratings yet





















































































Download as pdf or txt
You might also like
- Referat (PPT) - Hiperleukositosis & LeukostasisDocument16 pagesReferat (PPT) - Hiperleukositosis & LeukostasisShapira alNo ratings yet
- Guideline For Hemorrhagic ShockDocument8 pagesGuideline For Hemorrhagic ShockMikaGieJergoLarizaNo ratings yet
- Bloody Easy Coagulation SimplifiedDocument24 pagesBloody Easy Coagulation SimplifiedIlyasHasanNo ratings yet
- Definition of Transfusion ReactionDocument26 pagesDefinition of Transfusion ReactionAlvin A. AldeaNo ratings yet
- Adverse Effects of Blood Transfusion: 6 EditionDocument32 pagesAdverse Effects of Blood Transfusion: 6 EditionKaycee Gretz Loresca100% (1)
- Hemovigilancia ISBT 2011Document12 pagesHemovigilancia ISBT 2011Leonardo Borges dos SantosNo ratings yet
- Transfusion ReactionDocument66 pagesTransfusion ReactionAbhineet SalveNo ratings yet
- Serious Transfusion Incident Report 2015 16 PD PDFDocument57 pagesSerious Transfusion Incident Report 2015 16 PD PDFje zhNo ratings yet
- Paciente Que Sangra - Trastornos Hemorrágicos Adquiridos 2020Document9 pagesPaciente Que Sangra - Trastornos Hemorrágicos Adquiridos 202090STRATOVARIUS90No ratings yet
- TransfusiónDocument5 pagesTransfusiónMayra Alejandra Prada SerranoNo ratings yet
- Reactii PostransfuzionaleDocument11 pagesReactii PostransfuzionaleDenisa BrihanNo ratings yet
- Informed Consent - StatPearls - NCBI BookshelfDocument7 pagesInformed Consent - StatPearls - NCBI BookshelfShashank ShekharNo ratings yet
- Transfusion ReactionsDocument36 pagesTransfusion Reactionsmarky203No ratings yet
- Prevention of Adverse ReactionsDocument15 pagesPrevention of Adverse Reactionscupuwatie cahyaniNo ratings yet
- Hazards of Blood TransfusionDocument9 pagesHazards of Blood TransfusionMaria Leslie FernandezNo ratings yet
- Investigation of FMH by Flow CytometryDocument15 pagesInvestigation of FMH by Flow CytometryMohammed Khair BashirNo ratings yet
- Cancer Guide Oncologic EmergenciesDocument22 pagesCancer Guide Oncologic EmergenciesHerrera MiguelNo ratings yet
- Complications of Blood TransfusionDocument7 pagesComplications of Blood TransfusionChandan SrivastavaNo ratings yet
- 10 1016@j Transci 2020 103015Document4 pages10 1016@j Transci 2020 1030152mf2hgjrj9No ratings yet
- Guidelines On The Use of Intravenous Immune Globulin For Hematologic ConditionsDocument48 pagesGuidelines On The Use of Intravenous Immune Globulin For Hematologic ConditionssarahulfaaNo ratings yet
- Tipe Reaksi TransfusiDocument9 pagesTipe Reaksi TransfusiRangga Raditya RanggaNo ratings yet
- Blood Transfusion Reactions-A Comprehensive Review of The Literature Including A Swiss PerspectiveDocument19 pagesBlood Transfusion Reactions-A Comprehensive Review of The Literature Including A Swiss Perspectivecesarsamp2No ratings yet
- Dic 1Document6 pagesDic 1Sandra Lusi NovitaNo ratings yet
- Acute Transfusion Reactions Nov15Document16 pagesAcute Transfusion Reactions Nov15Toto ZazNo ratings yet
- Understanding Disseminated Intravascular Coagulation (DIC)Document40 pagesUnderstanding Disseminated Intravascular Coagulation (DIC)Denise135No ratings yet
- Blood Transfusion Error Prevention - Nurses RoleDocument5 pagesBlood Transfusion Error Prevention - Nurses RoleLorenn AdarnaNo ratings yet
- Martin 2016Document12 pagesMartin 2016rositha prabandariNo ratings yet
- Affiliate InstitutionsDocument10 pagesAffiliate Institutionspopov357No ratings yet
- HIV MedscapeDocument60 pagesHIV MedscapeInfinitiiiNo ratings yet
- Dengue Fever by Prof M Ali KhanDocument36 pagesDengue Fever by Prof M Ali KhanVina MuspitaNo ratings yet
- Dengue Fever by Prof M Ali KhanDocument36 pagesDengue Fever by Prof M Ali Khanmaha rNo ratings yet
- Hematology NotesDocument32 pagesHematology NotesbrittaNo ratings yet
- Blood Transfusion Reactions Revisited Dr. Edwin RodriguezDocument99 pagesBlood Transfusion Reactions Revisited Dr. Edwin RodriguezBeng AquinoNo ratings yet
- Sepsis Cap 44 Cirugía GeneralDocument14 pagesSepsis Cap 44 Cirugía GeneralKarla Montserrat González MuroNo ratings yet
- JIFCC Lab Tests Interpretation 2018Document8 pagesJIFCC Lab Tests Interpretation 2018Abdul Sattar100% (1)
- Dengue DOHDocument16 pagesDengue DOHGehlatin Tumanan100% (1)
- Probleme La TransfuziiDocument6 pagesProbleme La TransfuziiAdina TîrnoveanuNo ratings yet
- A Ciegas - Josh MalermanDocument6 pagesA Ciegas - Josh MalermanRooyValenciaNo ratings yet
- DR Zalina - Trafusion Reaction and Management PDFDocument77 pagesDR Zalina - Trafusion Reaction and Management PDFvasu_5iveNo ratings yet
- Jurnal Pengambilan Darah Vena PDFDocument10 pagesJurnal Pengambilan Darah Vena PDFfebriyankusumoningrum100% (1)
- Diagnosis FluidDocument14 pagesDiagnosis FluidCristianMP96No ratings yet
- Disseminated Intravascular Coagulation and Implications For Medical-Surgical NursesDocument5 pagesDisseminated Intravascular Coagulation and Implications For Medical-Surgical Nursesancours100% (1)
- Dengue Fever by Prof M Ali KhanDocument36 pagesDengue Fever by Prof M Ali KhanAnonymous uGbcVSJTDgNo ratings yet
- Haemodialysis With On-Line Monitoring EquipmentDocument12 pagesHaemodialysis With On-Line Monitoring EquipmentConnie Alva GutierrezNo ratings yet
- Ascorbic Acid NCPDocument8 pagesAscorbic Acid NCPJohann OrtizNo ratings yet
- JBB2012 151967Document13 pagesJBB2012 151967Prodia Central Java RegionNo ratings yet
- AdsasdadsaDocument252 pagesAdsasdadsaAmitShettyNo ratings yet
- NP40126 SaeDocument9 pagesNP40126 SaeMohd AljawfiNo ratings yet
- Otolaryngol - Head Neck Surg - 2014 - Al Khatib - Severe Vitamin D DeficiencyDocument8 pagesOtolaryngol - Head Neck Surg - 2014 - Al Khatib - Severe Vitamin D Deficiencyrohillak692No ratings yet
- Koate DVIDocument7 pagesKoate DVIagnesroNo ratings yet
- BT ReactionDocument8 pagesBT ReactionMary Elijah Jane PopesNo ratings yet
- IC Guidance For Preventing and Controlling Blood-Borne Virus Infection in Haemo Units Feb 10Document10 pagesIC Guidance For Preventing and Controlling Blood-Borne Virus Infection in Haemo Units Feb 10Slavica Gjurceska-GorjanskaNo ratings yet
- How Should We Use Convalescent Plasma Therapies For The Management of COVID-19?Document9 pagesHow Should We Use Convalescent Plasma Therapies For The Management of COVID-19?Asep tepiyanaNo ratings yet
- Hypovolemic Shock Guidelines PDFDocument8 pagesHypovolemic Shock Guidelines PDFAloysia Catur WidiNo ratings yet
- Emorrhagic Hock: Sogc Clinical Practice GuidelinesDocument8 pagesEmorrhagic Hock: Sogc Clinical Practice GuidelinesraysellaNo ratings yet
- Cpm15th Dengue Fever (Doh)Document18 pagesCpm15th Dengue Fever (Doh)Marko ParungoNo ratings yet
- Lab Technologist 11Document43 pagesLab Technologist 11AHAMED SHIFAANNo ratings yet
- Blood Transfusion ReactionsDocument3 pagesBlood Transfusion ReactionsANDREW MWITINo ratings yet
- Sepsis Diagnosis and Monitoring: Fast Early ReliableDocument24 pagesSepsis Diagnosis and Monitoring: Fast Early ReliableI Nyoman Gede Semarajana100% (1)
- Hemophilia and Hemostasis: A Case-Based Approach to ManagementFrom EverandHemophilia and Hemostasis: A Case-Based Approach to ManagementAlice D. MaNo ratings yet
- Physical Characteristics and VolumeDocument10 pagesPhysical Characteristics and Volumedeepika kushwahNo ratings yet
- 58-File Utama Naskah-62-1-10-20200928Document8 pages58-File Utama Naskah-62-1-10-20200928Alfaera Rahma FarestyNo ratings yet
- Jose, Ruth Domingo 2201022290Document5 pagesJose, Ruth Domingo 2201022290xveniaNo ratings yet
- Status Note On Blood SafetyDocument9 pagesStatus Note On Blood SafetyAlbin Prince John0% (1)
- Hemophilia in ChildrenDocument6 pagesHemophilia in Childrensimina intunericNo ratings yet
- IdmDocument46 pagesIdmht8zwk946sNo ratings yet
- Evoluºia I Tratamentul În Sindromul Hemolitic-Uremic La CopilDocument6 pagesEvoluºia I Tratamentul În Sindromul Hemolitic-Uremic La CopilAntonia GenesNo ratings yet
- 782Document20 pages782Aarathi raoNo ratings yet
- PRP Therapy Kit MainDocument1 pagePRP Therapy Kit Maindrsuryakant9818No ratings yet
- Working Instructions Investigation of Prolonged APTTDocument1 pageWorking Instructions Investigation of Prolonged APTTtadeariba1No ratings yet
- Iso ImmunizationDocument3 pagesIso ImmunizationHazel Marie EchavezNo ratings yet
- A Study On The Role of in in Haemolytic Disease of The NewbornDocument9 pagesA Study On The Role of in in Haemolytic Disease of The Newbornaymona2000No ratings yet
- Rehman Medical Institute: Test Result Unit Reference ValuesDocument1 pageRehman Medical Institute: Test Result Unit Reference ValuesfahadbasahirNo ratings yet
- 2 Labs Cheat Sheets Nurse NationDocument2 pages2 Labs Cheat Sheets Nurse NationkNo ratings yet
- Strategi Diagnosis AnemiaDocument49 pagesStrategi Diagnosis Anemianiniek yusidaNo ratings yet
- Experiment Number 3 Sample Preparation For Blood Banking ProcedureDocument10 pagesExperiment Number 3 Sample Preparation For Blood Banking ProcedureKriziaNo ratings yet
- Fullpapers IJCPML 12-3-08Document4 pagesFullpapers IJCPML 12-3-08ryanNo ratings yet
- Feline Blood TransfusionDocument4 pagesFeline Blood TransfusionPhilipsNo ratings yet
- ABO Blood Group System NotesDocument45 pagesABO Blood Group System NotesAnne Carmel Verano100% (1)
- Erythrocyte Sedimentation Rate: Hematology 1 ReportDocument18 pagesErythrocyte Sedimentation Rate: Hematology 1 ReportNico LokoNo ratings yet
- Management of Blood Donors and Blood Donations From Individuals Found To Have A Positive Direct Antiglobulin TestDocument11 pagesManagement of Blood Donors and Blood Donations From Individuals Found To Have A Positive Direct Antiglobulin TestLuis Enrique Tinoco JuradoNo ratings yet
- 2021 ISFM Consensus Guidelines On The Collection and Administration of Blood and Blood Products in CatsDocument23 pages2021 ISFM Consensus Guidelines On The Collection and Administration of Blood and Blood Products in CatsNurul Izzatul AnnisaNo ratings yet
- BCM 20 Ultra NewDocument11 pagesBCM 20 Ultra NewWessamNo ratings yet
- Pathway HiperbilirubinDocument1 pagePathway HiperbilirubinHendri Ty100% (1)
- Iron Defisience AnemiaDocument61 pagesIron Defisience AnemiaYeni Jesika SilitongaNo ratings yet
- WarfarinDocument2 pagesWarfarinWAHYU NOFANDARI HERDIYANTINo ratings yet
- Hemophilia in ChildrenDocument16 pagesHemophilia in ChildrenVinay Sahu100% (1)
- Fu Mcu 12102022Document12 pagesFu Mcu 12102022anggaNo ratings yet