Download as pdf or txt
You might also like
- DIY HRT Harm Reduction Guide PDFDocument11 pagesDIY HRT Harm Reduction Guide PDFKentucky Trans Health JusticeNo ratings yet
- Pedia Nicu NotesDocument32 pagesPedia Nicu NotesChristian Noel Fernandez100% (3)
- Ayurveda A Quick Reference Handbook Illustrated 0940676958 9780940676954Document99 pagesAyurveda A Quick Reference Handbook Illustrated 0940676958 9780940676954Jawahar Lal NehruNo ratings yet
- 07-Cell Cycle Virtual Lab Handout SolutionsDocument4 pages07-Cell Cycle Virtual Lab Handout Solutionschuckly100% (2)
- Prediabetes 1Document21 pagesPrediabetes 1Nirmaa100% (2)
- HRT Timeline and Effects Hormone Replacement Therapy InfoDocument1 pageHRT Timeline and Effects Hormone Replacement Therapy Infoz5st795cd7No ratings yet
- CB7 All SheetsDocument38 pagesCB7 All SheetsAryan AdhikariNo ratings yet
- NCM 118 PrelimDocument10 pagesNCM 118 PrelimJodilyn Layo MatunogNo ratings yet
- 1501Document569 pages1501Ina Revenco33% (3)
- Pediatrics Revision E6.5 @TheBoggusdocDocument55 pagesPediatrics Revision E6.5 @TheBoggusdocsushmaNo ratings yet
- Disability Duration Guidelines and Expected Healing TimesDocument64 pagesDisability Duration Guidelines and Expected Healing TimesMarco Antonio Borges das NevesNo ratings yet
- J ANIM SCI-1986-Cochran-1469-75Document8 pagesJ ANIM SCI-1986-Cochran-1469-75Alberto ChambelaNo ratings yet
- To Study The Effect of The Mineral - Compound As Hair Removal. (Romashatan)Document8 pagesTo Study The Effect of The Mineral - Compound As Hair Removal. (Romashatan)ShyamNo ratings yet
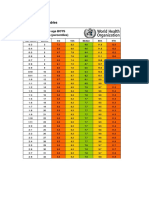
- TABLE Boys 3mo To 5yr TRICEPSage PercentileDocument2 pagesTABLE Boys 3mo To 5yr TRICEPSage Percentilel10n_assNo ratings yet
- Niruha BastiDocument20 pagesNiruha BastiGAURAV100% (5)
- Useful Statistics KZN AnimalsDocument5 pagesUseful Statistics KZN AnimalsCornelVermaakNo ratings yet
- Intermediate 1Document41 pagesIntermediate 1Rip J1No ratings yet
- Medical Students' Committee F or International AffairsDocument2 pagesMedical Students' Committee F or International AffairsveehananiNo ratings yet
- Hotpantz: Herbal GynecologyDocument28 pagesHotpantz: Herbal GynecologyMandy M.100% (20)
- Lecture 4 - Symptoms of EstrusDocument4 pagesLecture 4 - Symptoms of Estruskushal NeupaneNo ratings yet
- SchedDocument5 pagesSchedJohn CenasNo ratings yet
- A Body Image Scale For Evaluating Transsexuals J: Thomas W. Lindgren, M.D., 2 and Ira B. Pauly, M.D. 3Document18 pagesA Body Image Scale For Evaluating Transsexuals J: Thomas W. Lindgren, M.D., 2 and Ira B. Pauly, M.D. 3José Ignacio PérezNo ratings yet
- Obgy NumbersDocument4 pagesObgy NumbersdhavaldankhraeduNo ratings yet
- Newborn Assessment Period: ST THDocument3 pagesNewborn Assessment Period: ST THYoussef AliNo ratings yet
- Equine Vaccination Schedule: Vaccine Foals/Weanlings Yearlings Performance Pleasure/Ranch Broodmares 3-Way (TetanusDocument4 pagesEquine Vaccination Schedule: Vaccine Foals/Weanlings Yearlings Performance Pleasure/Ranch Broodmares 3-Way (TetanusSadam IrshadNo ratings yet
- Minggu 3 Minggu 4 Minggu 5: ISN SEL RAB KHA JUM ISN SEL RABDocument1 pageMinggu 3 Minggu 4 Minggu 5: ISN SEL RAB KHA JUM ISN SEL RABHEMA A/P K.RAMU MoeNo ratings yet
- Testosterone: Given by Subcutaneous (Under The Skin) InjectionsDocument8 pagesTestosterone: Given by Subcutaneous (Under The Skin) Injectionsalice jacksonNo ratings yet
- (14717899 - Reproduction) VARIATIONS IN SERUM FSH, LH AND TESTOSTERONE LEVELS IN MALE RATS FROM BIRTH TO SEXUAL MATURITY PDFDocument6 pages(14717899 - Reproduction) VARIATIONS IN SERUM FSH, LH AND TESTOSTERONE LEVELS IN MALE RATS FROM BIRTH TO SEXUAL MATURITY PDFAminudin AlfatNo ratings yet
- An Autopsy Study To Evaluate Time Since Death From Organs Weight and Physical ParametersDocument5 pagesAn Autopsy Study To Evaluate Time Since Death From Organs Weight and Physical ParametersYunanda RizkiNo ratings yet
- Frozen Embryo Transfer Booklet: Saint Mary's HospitalDocument12 pagesFrozen Embryo Transfer Booklet: Saint Mary's HospitalKirubakaranNo ratings yet
- The Pubescent Period 1MDocument19 pagesThe Pubescent Period 1M1B - Zafra, RamoneNo ratings yet
- Highlights of The Exposure Factors For Activity FactorsDocument6 pagesHighlights of The Exposure Factors For Activity FactorsWong KinsonNo ratings yet
- AAA - Nelsons 20th Summary Part 1Document79 pagesAAA - Nelsons 20th Summary Part 1Jessica MarianoNo ratings yet
- PediatricsDocument58 pagesPediatricsWorld MedclickzNo ratings yet
- Estrous Cycle Different Stages in Domestic Animals PDFDocument3 pagesEstrous Cycle Different Stages in Domestic Animals PDFYounas marri100% (1)
- Hsslive Xii QB by Vhse ZoologyDocument37 pagesHsslive Xii QB by Vhse Zoology16739No ratings yet
- Gonadotropinas - Tiempo PrepubertadDocument10 pagesGonadotropinas - Tiempo PrepubertadVioleta v cNo ratings yet
- 2.0 Trigger-Point Guide: Start HereDocument9 pages2.0 Trigger-Point Guide: Start HereBStrong Do No WrongNo ratings yet
- Sat KriyaDocument2 pagesSat KriyacaterinaNo ratings yet
- Pediatric Reference RangesDocument9 pagesPediatric Reference RangesmmmmmmNo ratings yet
- AdolescenceDocument6 pagesAdolescencekomalangel.aroraNo ratings yet
- Lec05 Breeding - Importance of Cross Breeding. Signs of Estrous Cycle-ArtificialDocument6 pagesLec05 Breeding - Importance of Cross Breeding. Signs of Estrous Cycle-ArtificialarunNo ratings yet
- Pedia CardsDocument40 pagesPedia CardsKristine Marie Santos100% (1)
- Normal Growth: and DevelopmentDocument21 pagesNormal Growth: and DevelopmentsumitNo ratings yet
- Natural Selection Lab Report E-Portfolio Assignment Revised Anthropology Human OriginsDocument7 pagesNatural Selection Lab Report E-Portfolio Assignment Revised Anthropology Human Originsapi-306763831No ratings yet
- Growth Guinea-Pig: Biphasic CycleDocument4 pagesGrowth Guinea-Pig: Biphasic CycleEveAriNo ratings yet
- Send A Message..Document1 pageSend A Message..5drkjg2p8pNo ratings yet
- Numerology and Weight Gain TendencyDocument3 pagesNumerology and Weight Gain TendencyAleksandar MihajlovićNo ratings yet
- Normal ValuesDocument4 pagesNormal ValuesBryan Neil GarmaNo ratings yet
- Planaria Lab ReportDocument5 pagesPlanaria Lab Reportapi-194762577No ratings yet
- Normal ValuesDocument12 pagesNormal ValuessweetyjonasNo ratings yet
- Care Plan ON PEM: Maa Tripura College of Nursing, Jhabua (M.P.)Document7 pagesCare Plan ON PEM: Maa Tripura College of Nursing, Jhabua (M.P.)amit100% (1)
- TissuetrainingDocument29 pagesTissuetrainingEsther Vargas LozadaNo ratings yet
- Growth, Puberty, Sexual Maturity in Relation To ReproductionDocument2 pagesGrowth, Puberty, Sexual Maturity in Relation To Reproductionkushal NeupaneNo ratings yet
- Vedic Astrology HindiDocument46 pagesVedic Astrology HindiBelinda LeeNo ratings yet
- Biology of Reproduction, Suckling Regimes, Growth and DevelopmentDocument60 pagesBiology of Reproduction, Suckling Regimes, Growth and DevelopmentGradinaru ValiNo ratings yet
- Midterm TopicDocument19 pagesMidterm TopicGlyza EbradaNo ratings yet
- TekleDocument8 pagesTeklebirukNo ratings yet
- Endocrine SystemDocument93 pagesEndocrine SystemMa. Jamila JandusayNo ratings yet
- How Planets Affect Our Lives: An observational study that can be read by anyone including those who have no knowledge of astrology.From EverandHow Planets Affect Our Lives: An observational study that can be read by anyone including those who have no knowledge of astrology.No ratings yet
- Insulinoma in Dogs: A Review: Normal Glucose HomeostasisDocument13 pagesInsulinoma in Dogs: A Review: Normal Glucose HomeostasisBrisbany AlcibarNo ratings yet
- Definition and ClassificationDocument36 pagesDefinition and Classificationplogiojayr8340No ratings yet
- Vaginal AgenesisDocument3 pagesVaginal Agenesissanks06No ratings yet
- Female Pregnancy: Slide by MikokitDocument17 pagesFemale Pregnancy: Slide by MikokitGwreyneth Kate MiroNo ratings yet
- Estrous Synchronization in Sheep and GoatDocument56 pagesEstrous Synchronization in Sheep and GoatDrTara Chand Jangir80% (5)
- Anaphy Lecture Activity 10 Endocrine SystemDocument5 pagesAnaphy Lecture Activity 10 Endocrine SystemJohnNo ratings yet
- Kartagener SyndromeDocument4 pagesKartagener Syndromemilkah mwauraNo ratings yet
- Thyroid CrisisDocument20 pagesThyroid CrisisJeffrey DyerNo ratings yet
- JainamDocument20 pagesJainamSpandan KadamNo ratings yet
- Ata Hyperthyroidism BrochureDocument3 pagesAta Hyperthyroidism BrochureKumalaAudiKusumaNo ratings yet
- Lecture I Anatomy of The Gi Tract Lecture Notes Lectures 1 20 PDFDocument322 pagesLecture I Anatomy of The Gi Tract Lecture Notes Lectures 1 20 PDFLilyNo ratings yet
- A&P - 4. Insulin, Glucagon & Regulation of Metabolism (6p) PDFDocument6 pagesA&P - 4. Insulin, Glucagon & Regulation of Metabolism (6p) PDFSreejith Jagal KishoreNo ratings yet
- Nama Barang Cream Malam: Harga Reseller HK Beautycare Harga Jual Harga Resseler Harga Jual Keuntungan ResellerDocument3 pagesNama Barang Cream Malam: Harga Reseller HK Beautycare Harga Jual Harga Resseler Harga Jual Keuntungan ResellerAsep NurzamanNo ratings yet
- Jurnal - Comparative Study of Male and Female Sebum Production 2017Document6 pagesJurnal - Comparative Study of Male and Female Sebum Production 2017Melvy RozaNo ratings yet
- FRM Patient View All ReportDocument3 pagesFRM Patient View All ReportRajeev KumarNo ratings yet
- 1543-Article Text-5316-1-10-20200407Document7 pages1543-Article Text-5316-1-10-20200407Deadly BladeNo ratings yet
- Partial Mole or Complete Mole: Pathophysiology of Molar PregnancyDocument1 pagePartial Mole or Complete Mole: Pathophysiology of Molar PregnancyKristian Karl Bautista Kiw-isNo ratings yet
- Breast Development and Morphology - UpToDateDocument43 pagesBreast Development and Morphology - UpToDateAndrea Díaz Rodríguez0% (1)
- Corticosteroids WordDocument10 pagesCorticosteroids WordMahnoor ArshadNo ratings yet
- Cretinism The Past Present and Future of Diagnosis and Cure 2003Document2 pagesCretinism The Past Present and Future of Diagnosis and Cure 2003Family Medicine FK UnsyiahNo ratings yet
- SyllabusDocument44 pagesSyllabusom vermaNo ratings yet
- Thyroid SwellingDocument4 pagesThyroid SwellingShafiq ZahariNo ratings yet
- Midterms Reviewer Ana 2Document8 pagesMidterms Reviewer Ana 2Ais WallensteinNo ratings yet
- Endocrine Physiology Case Study - BathshebaDocument6 pagesEndocrine Physiology Case Study - BathshebaMc Lindssey PascualNo ratings yet
- Diabetes and You: Your Guide To Better Living With DiabetesDocument51 pagesDiabetes and You: Your Guide To Better Living With DiabetesdrjperumalNo ratings yet
- Linear MeasurementDocument57 pagesLinear MeasurementbkangusNo ratings yet
- Androgenic Supplementation in Men - Effects of Age Herbal ExtractDocument154 pagesAndrogenic Supplementation in Men - Effects of Age Herbal ExtractMaria PopaNo ratings yet
- Harga Normal LaboratDocument14 pagesHarga Normal LaboratMistrionoNo ratings yet
- Water Deprivation TestDocument5 pagesWater Deprivation TestGhada ElhassanNo ratings yet