Download as pdf or txt
You might also like
- Unit 2 Organizational Structure of PEDocument10 pagesUnit 2 Organizational Structure of PEAngel Marie Cahanap100% (2)
- Assignment Module 2Document15 pagesAssignment Module 2Sania Malik82% (66)
- Practice Examination For HESI ExitDocument76 pagesPractice Examination For HESI ExitGod_is_Good_294486% (43)
- Sensory Diet: Prepared by Christy E. Yee, OTRDocument12 pagesSensory Diet: Prepared by Christy E. Yee, OTRAlexandra StăncescuNo ratings yet
- Case Study Colorectal CancerDocument23 pagesCase Study Colorectal CancerLeogalvez BedanoNo ratings yet
- Neur0 NLE Practice ExamDocument10 pagesNeur0 NLE Practice ExamRI NANo ratings yet
- Physical Education Activity 1 Describe How These Principles Are Essential in Teaching Physical Education inDocument7 pagesPhysical Education Activity 1 Describe How These Principles Are Essential in Teaching Physical Education inCiel EvangelistaNo ratings yet
- Module 02Document17 pagesModule 02Abdul MuqeetNo ratings yet
- Brain Based LearningDocument33 pagesBrain Based LearningJane FowlerNo ratings yet
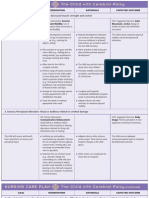
- Home Plan For Hemiplegic CPDocument13 pagesHome Plan For Hemiplegic CPMaira PervezNo ratings yet
- Mapeh: Music - Arts - Physical Education - HealthDocument14 pagesMapeh: Music - Arts - Physical Education - HealthjonieshayneNo ratings yet
- Toaz - Info Grade 7 Pe Module PRDocument16 pagesToaz - Info Grade 7 Pe Module PRVince Ivan S. PacayraNo ratings yet
- Module-2 Exercises of Practical Life (EPL) : Myida Binte Majeed Roll No # DK2306Document11 pagesModule-2 Exercises of Practical Life (EPL) : Myida Binte Majeed Roll No # DK2306myida majeedNo ratings yet
- What Is Brain Gym?: 3. Double DoodleDocument1 pageWhat Is Brain Gym?: 3. Double DoodleFrance BejosaNo ratings yet
- Q1 W1 Mod1 Physical Education 12 HRFDocument9 pagesQ1 W1 Mod1 Physical Education 12 HRFClareen June DagoyNo ratings yet
- Paediatric Neurology:: Management Practices and Evidence Based PracticesDocument41 pagesPaediatric Neurology:: Management Practices and Evidence Based PracticesNikita ChaubeNo ratings yet
- Physical Education & Health Ii: Core SubjectDocument8 pagesPhysical Education & Health Ii: Core SubjectErika Louise LabiosNo ratings yet
- Ped-7facilitating Learner CenteredDocument5 pagesPed-7facilitating Learner CenteredJessica VillanuevaNo ratings yet
- Path FitDocument3 pagesPath FitLester AganonNo ratings yet
- FINAL EDIT Ped001-ModuleDocument50 pagesFINAL EDIT Ped001-ModuleChing DialomaNo ratings yet
- HCPSSensory Integration HandbookDocument20 pagesHCPSSensory Integration HandbookClaudia Ichele DíazNo ratings yet
- Grade 4 Physical Education Lesson PlanDocument9 pagesGrade 4 Physical Education Lesson Plancabasagglenda8No ratings yet
- Grade 7 PE ModuleDocument11 pagesGrade 7 PE ModuleMeann Joy Barrios Mendoza100% (1)
- Prof. Ed. 1 Semifinals ModuleDocument19 pagesProf. Ed. 1 Semifinals ModuleKyla Jelinne CastilloNo ratings yet
- Mindfulness Is Not Only A Popular Topic For Researchers and AcademicsDocument14 pagesMindfulness Is Not Only A Popular Topic For Researchers and AcademicsDumitruRalucaNo ratings yet
- Ot HandbookDocument24 pagesOt Handbooktaraka sravyaNo ratings yet
- What Is Conductive Education?Document6 pagesWhat Is Conductive Education?Amina SawalmehNo ratings yet
- Inclusive EducationDocument6 pagesInclusive Educationchris black MateusNo ratings yet
- Assignment Module 2: Rabia Shazeb ROLL# DK2007 Question # 1Document21 pagesAssignment Module 2: Rabia Shazeb ROLL# DK2007 Question # 1Rabia ShazebNo ratings yet
- CH 20, 21, 30Document9 pagesCH 20, 21, 30DaNelle McPhaddenNo ratings yet
- ASSIGNMENT 831 Zubi.2Document25 pagesASSIGNMENT 831 Zubi.2Faheem Elahi FomeNo ratings yet
- LP How To Care For Our BodiesDocument2 pagesLP How To Care For Our BodiesAin SyahiraNo ratings yet
- Motor Control Motor LearningDocument56 pagesMotor Control Motor LearningJune EpeNo ratings yet
- March 21Document4 pagesMarch 21marita castilloNo ratings yet
- Names: Gulshan Shehzadi Roll# D17090 Topic: Exercise of Practical Life (EPL)Document18 pagesNames: Gulshan Shehzadi Roll# D17090 Topic: Exercise of Practical Life (EPL)Gulshan ShehzadiNo ratings yet
- Learning Process and Acquiring SkillsDocument18 pagesLearning Process and Acquiring SkillsHarris PaulNo ratings yet
- Sociology AssignmentDocument19 pagesSociology AssignmentHarbhajan SinghNo ratings yet
- Physical Impairment and Self Care FOSIEDocument7 pagesPhysical Impairment and Self Care FOSIENorsaidin TungkagNo ratings yet
- The Managing and Caring For The SelfDocument27 pagesThe Managing and Caring For The SelfLouise SantosNo ratings yet
- Chapter-4 XiDocument5 pagesChapter-4 Xirajat jainNo ratings yet
- Learning Theories Thorndike Pavlov Watson Skinner 1Document47 pagesLearning Theories Thorndike Pavlov Watson Skinner 1jonel.race34No ratings yet
- Goal SettingDocument4 pagesGoal SettingSherwin BasanNo ratings yet
- What Is Brain GymDocument4 pagesWhat Is Brain Gymsaiqa batoolNo ratings yet
- Assignment Module 2 (Saba Nauman-DK2502)Document11 pagesAssignment Module 2 (Saba Nauman-DK2502)Saba NaumanNo ratings yet
- Pediatric Evaluation and Plan of CareDocument10 pagesPediatric Evaluation and Plan of CareVeronica MwendeNo ratings yet
- Pe 101 ActivityDocument2 pagesPe 101 ActivityGlazel V GonzagaNo ratings yet
- PMC-Module 2 Assignment 2. PDFDocument10 pagesPMC-Module 2 Assignment 2. PDFsana100% (3)
- Module II Psychological Foundations of CurriculumDocument6 pagesModule II Psychological Foundations of CurriculumCatherine yapeNo ratings yet
- Child - Cerebral PalsyDocument3 pagesChild - Cerebral PalsyJamie Icabandi67% (3)
- Module 2Document12 pagesModule 2kausarktk33No ratings yet
- Emotional Wellbeing Unit of LearningDocument43 pagesEmotional Wellbeing Unit of LearningMushaim AfreenNo ratings yet
- Modular-Hard Learners' ManualDocument14 pagesModular-Hard Learners' ManualWayne James RusselNo ratings yet
- Brain Based EducationDocument7 pagesBrain Based Educationchristine baldonazaNo ratings yet
- PATHFit1 Study GuideDocument4 pagesPATHFit1 Study GuideemmanuelanecesitoNo ratings yet
- Q1-Week 1-5 Business MathDocument17 pagesQ1-Week 1-5 Business Mathemmalou shane fernandezNo ratings yet
- Questions PEDocument9 pagesQuestions PEBinth caderNo ratings yet
- Module 1Document12 pagesModule 1PanJan BalNo ratings yet
- Arthrogryposis Multiplex Congenita (Amc) : Tapan Kumar ParasethDocument24 pagesArthrogryposis Multiplex Congenita (Amc) : Tapan Kumar ParasethTapan Paraseth StudiesNo ratings yet
- PE Grade 10 (2ndQT)Document8 pagesPE Grade 10 (2ndQT)Jeric MatunhayNo ratings yet
- Hope 1: Health Optimizing Physical EducationDocument15 pagesHope 1: Health Optimizing Physical EducationSakusakuNo ratings yet
- HOPE1-Lesson8 FinalDocument9 pagesHOPE1-Lesson8 FinalEian InganNo ratings yet
- Learning TheoriesDocument21 pagesLearning Theorieswinwin86No ratings yet
- Summary of Barbara Neiman's Mindfulness & Yoga Skills For Children and AdolescentsFrom EverandSummary of Barbara Neiman's Mindfulness & Yoga Skills For Children and AdolescentsNo ratings yet
- General Pharmacology - Sources of Drugs and Routes of AdministrationDocument48 pagesGeneral Pharmacology - Sources of Drugs and Routes of AdministrationDhriti Brahma78% (9)
- MPNST Pleiomorphic MRDocument30 pagesMPNST Pleiomorphic MRBian PutriNo ratings yet
- Functional Training Part 1: New Advances: Clinician'Sinformationforself-HelpproceduresDocument7 pagesFunctional Training Part 1: New Advances: Clinician'Sinformationforself-HelpproceduresGust AvoNo ratings yet
- Andrea MillsDocument2 pagesAndrea MillsAndrea MillsNo ratings yet
- AIDS Related Mycoses Updated Progress and FutureDocument4 pagesAIDS Related Mycoses Updated Progress and Futurelwlolo168No ratings yet
- Jospt 2019 0301 PDFDocument85 pagesJospt 2019 0301 PDFyohanNo ratings yet
- Anitbiotic Treatment in Cystic FibrosisDocument76 pagesAnitbiotic Treatment in Cystic FibrosisOxana TurcuNo ratings yet
- OME StudyGuide 2monthDocument5 pagesOME StudyGuide 2monthVarNo ratings yet
- Induction Booklet - Final VersionDocument60 pagesInduction Booklet - Final VersionMuhammad YousufNo ratings yet
- Ampra Depo UgdDocument2 pagesAmpra Depo UgdCitra NingrumNo ratings yet
- ICU - DR Abdullah AlRbiaanDocument224 pagesICU - DR Abdullah AlRbiaanAHMAD ALROWAILYNo ratings yet
- Guidelines For Hospital Regarding Claim Prepration For Payment Clearance - SSPDocument1 pageGuidelines For Hospital Regarding Claim Prepration For Payment Clearance - SSPumayrh@gmail.comNo ratings yet
- Beat CancerDocument114 pagesBeat CancerGeorge Dragoi100% (9)
- Ascento Dental Line Catalog Implanturi Alpha Dent GermaniaDocument82 pagesAscento Dental Line Catalog Implanturi Alpha Dent GermaniaGabriela IconaruNo ratings yet
- PEDIA 20Idiot20Notes 1Document76 pagesPEDIA 20Idiot20Notes 1Aljon S. TemploNo ratings yet
- Costello-Boerrigter Et Al - AJP 2005 - V2 Receptor Antagonism Augments Water Excretion Without Changes in Renal Hemodynamics or Na and K Excretion in Human HFDocument6 pagesCostello-Boerrigter Et Al - AJP 2005 - V2 Receptor Antagonism Augments Water Excretion Without Changes in Renal Hemodynamics or Na and K Excretion in Human HFtankNo ratings yet
- Community Dentistry McqsDocument11 pagesCommunity Dentistry McqsIsaac Nsenga100% (3)
- WCLC2017 Abstract Book WebDocument700 pagesWCLC2017 Abstract Book Webdavid.yb.wangNo ratings yet
- Vulvectomy: Patient Information Patient InformationDocument11 pagesVulvectomy: Patient Information Patient InformationMega FebrianaNo ratings yet
- Pediatric Readiness Guidelines ChecklistDocument4 pagesPediatric Readiness Guidelines ChecklistsabirNo ratings yet
- Current and Emerging Treatment Strategies For Duchenne Muscular DystrophyDocument14 pagesCurrent and Emerging Treatment Strategies For Duchenne Muscular DystrophyANAMIKA ANANDINo ratings yet
- Nursing Care Plan ColostomyDocument5 pagesNursing Care Plan ColostomyCarissa Mae Tapec EstradaNo ratings yet
- Strasburger Et Al-2015-PsyCh JournalDocument8 pagesStrasburger Et Al-2015-PsyCh JournalPedro CardosoNo ratings yet
- Situational Tasks Such As KROK Pharmacology English Sem 6Document17 pagesSituational Tasks Such As KROK Pharmacology English Sem 6Mi PatelNo ratings yet
- Atlas of Laparoscopic Urologic Surgery, 1E (2007) PDFDocument340 pagesAtlas of Laparoscopic Urologic Surgery, 1E (2007) PDFAndreea Q. PopaNo ratings yet
- Using Voice Change As An Indicator of Dysphagia A Systematic ReviewDocument13 pagesUsing Voice Change As An Indicator of Dysphagia A Systematic ReviewSandra Liliana Sosa SabogalNo ratings yet
- Daftar Harga Terbaru 9 September 2021 Dept. Generik: Column1 Column2 Column3 Column4Document2 pagesDaftar Harga Terbaru 9 September 2021 Dept. Generik: Column1 Column2 Column3 Column4Lia Mahdi AgustianiNo ratings yet