
51 - Absorption of Toxicants
51 - Absorption of Toxicants
You might also like
- The Skincare Bible PDFDocument156 pagesThe Skincare Bible PDFLacramioara Valentina100% (12)
- Anatomy One Pager G&aDocument2 pagesAnatomy One Pager G&aJennaNo ratings yet
- Integumentary System ReviewerDocument12 pagesIntegumentary System ReviewerLly Isidoro100% (2)
- Chapter 07 IntegumentaryDocument4 pagesChapter 07 IntegumentaryBernard Paul Guinto50% (2)
- Microblading ManualDocument6 pagesMicroblading ManualPaulina Pineda100% (1)
- Combination of Microneedling and Glycolic Acid Peels For TheDocument7 pagesCombination of Microneedling and Glycolic Acid Peels For Thealejandrogonzalez89No ratings yet
- Absorption and Extraction of ToxinDocument22 pagesAbsorption and Extraction of Toxinabhishekranjan090202No ratings yet
- Pharmacokinetics ProcessDocument11 pagesPharmacokinetics ProcesstitusNo ratings yet
- Absorption and Distribution of Toxicants - L4Document3 pagesAbsorption and Distribution of Toxicants - L4prasad sanjayaNo ratings yet
- Pharmacokinetics Webquest: Kimberly Koon, Pharm. D. Bw733 October 1, 2013Document27 pagesPharmacokinetics Webquest: Kimberly Koon, Pharm. D. Bw733 October 1, 2013كسلان اكتب اسميNo ratings yet
- Topic 5ADocument54 pagesTopic 5AMohd RafiqNo ratings yet
- 2024-EnChem CHAP 5Document30 pages2024-EnChem CHAP 5vuthidieuthaot67No ratings yet
- Transdermal DDSDocument20 pagesTransdermal DDSPC BUGNo ratings yet
- Phardose - Transdermal Drug Delivery SystemDocument25 pagesPhardose - Transdermal Drug Delivery SystemEdrick RamoranNo ratings yet
- Pharmacokinetic, Absorption and Ionisation of DrugsDocument31 pagesPharmacokinetic, Absorption and Ionisation of DrugsAli ElmehdawiNo ratings yet
- 7 Transdermal Drug Delivery SystemDocument59 pages7 Transdermal Drug Delivery Systemwikako9357No ratings yet
- 03.transdermal Drug Delivery SystemsDocument56 pages03.transdermal Drug Delivery SystemsMoganaa LakshmiNo ratings yet
- Trans Dermal Drug DeliveryDocument47 pagesTrans Dermal Drug Deliverysouvik maitiNo ratings yet
- 295 PDFDocument6 pages295 PDFHaola andaniNo ratings yet
- Unit 1Document13 pagesUnit 1parmarkeval1610No ratings yet
- Drug Delevery SystemDocument47 pagesDrug Delevery SystempravincrNo ratings yet
- Organophosphate PoisoningDocument24 pagesOrganophosphate PoisoningScribdTranslationsNo ratings yet
- AbsorptionDocument61 pagesAbsorptionGreenNo ratings yet
- Ico Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanDocument34 pagesIco Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanMelkamu AyeNo ratings yet
- Transdermal Drug Delivery System: Shirode Rahul ADocument37 pagesTransdermal Drug Delivery System: Shirode Rahul AFrancisco MarcanoNo ratings yet
- Semester Test 1 NotesDocument23 pagesSemester Test 1 NotesElla BoyceNo ratings yet
- Semisolids Ointment Updated Final-1Document21 pagesSemisolids Ointment Updated Final-1Sunjida Ali RiyaNo ratings yet
- Polymer Membranes in Biomedical FieldDocument35 pagesPolymer Membranes in Biomedical FieldAbufathima CheruvadiNo ratings yet
- Prokaryotic & Eukaryotic Cells - 3Document47 pagesProkaryotic & Eukaryotic Cells - 3AnaNo ratings yet
- Integrated Vector Control Approach: Dr. Kulrajat BhasinDocument37 pagesIntegrated Vector Control Approach: Dr. Kulrajat BhasinPallabi DasguptaNo ratings yet
- Biopharmaceutics Lecture 2 UquDocument36 pagesBiopharmaceutics Lecture 2 Uquرنا الشريفNo ratings yet
- Transdermal Drug Delivery SystemDocument40 pagesTransdermal Drug Delivery SystemDewang PatilNo ratings yet
- Week 2 - Drugs and The BodyDocument18 pagesWeek 2 - Drugs and The BodyDino MicaNo ratings yet
- Transdermaldrugdeliverysystem FinalDocument84 pagesTransdermaldrugdeliverysystem Finalsowjanya kNo ratings yet
- TDDSDocument82 pagesTDDSVouge ModeNo ratings yet
- Annotated-CHIU, CHERYL S. - exeRCISE 2 - Transport ProcessesDocument4 pagesAnnotated-CHIU, CHERYL S. - exeRCISE 2 - Transport ProcessesCheryl ChiuNo ratings yet
- Chapter 11 Transdermal Drug Delivery SystemDocument3 pagesChapter 11 Transdermal Drug Delivery SystemluisynonNo ratings yet
- Wound Management and Aftercare: Oral & Maxillofacial SurgeryDocument33 pagesWound Management and Aftercare: Oral & Maxillofacial Surgerymehul7patel-10No ratings yet
- Phase I: Chemical Modifications That Introduce or Uncover Functional Groups On A XenobioticDocument5 pagesPhase I: Chemical Modifications That Introduce or Uncover Functional Groups On A XenobioticBlue SaphyrNo ratings yet
- Introduction To Bio PharmaceuticsDocument88 pagesIntroduction To Bio PharmaceuticsSohan PrasathNo ratings yet
- Good Morning Class: - DR MehnazDocument42 pagesGood Morning Class: - DR MehnazUzair KhanNo ratings yet
- Gram Positive Rod of Medical Imortance IIDocument36 pagesGram Positive Rod of Medical Imortance IIJoeyNo ratings yet
- Unit.1 Absorption-Mechanisms of Drug Absorption Through GIT.Document25 pagesUnit.1 Absorption-Mechanisms of Drug Absorption Through GIT.deepshah6068No ratings yet
- Routes of Drug AdministrationDocument6 pagesRoutes of Drug AdministrationKena SamuelNo ratings yet
- BP604T Lecturer's Slides - CompressedDocument119 pagesBP604T Lecturer's Slides - CompressedGyampoh SolomonNo ratings yet
- Neeraj Assignment PDFDocument68 pagesNeeraj Assignment PDFNeeraj GautamNo ratings yet
- IntroductionDocument18 pagesIntroductionsai projectNo ratings yet
- Principles of Toxicology and Basic Treatment: PWM Olly Indrajani 2014Document22 pagesPrinciples of Toxicology and Basic Treatment: PWM Olly Indrajani 2014Princes Mentari Dwi NurainiNo ratings yet
- Paralec M1Document8 pagesParalec M1VE NI CENo ratings yet
- Transdermal Drug Delivery SystemDocument47 pagesTransdermal Drug Delivery SystemMridul AroraNo ratings yet
- Pharmacokinetics: Sun Yi Department of PharmacologyDocument53 pagesPharmacokinetics: Sun Yi Department of PharmacologyMOHAMMAD NAZMUL ISLAMNo ratings yet
- UNIT 2 - Week (4-5) : Mechanisms of Toxicity & Toxicokinetics Intended Learning Outcomes (ILO)Document8 pagesUNIT 2 - Week (4-5) : Mechanisms of Toxicity & Toxicokinetics Intended Learning Outcomes (ILO)Hannah Jean Lapenid LemorenasNo ratings yet
- Bio136 186Unit3P2Document89 pagesBio136 186Unit3P2jhon pauloNo ratings yet
- Endocrine GlandsDocument13 pagesEndocrine GlandsAyesha Jalal KhanNo ratings yet
- Chapter 2Document9 pagesChapter 2jjumlaboratoryNo ratings yet
- Biomedical Nanotechnology: Lecture 18: Cellular Uptake Mechanisms of NanomaterialsDocument43 pagesBiomedical Nanotechnology: Lecture 18: Cellular Uptake Mechanisms of NanomaterialsDURGA DEVI T 037 BME100% (1)
- Micro Microbial Mechanisms of Pathogenicity NOTESDocument6 pagesMicro Microbial Mechanisms of Pathogenicity NOTESAriane NobleNo ratings yet
- Unit 4 Transdermal Drug Delivary System (1)Document42 pagesUnit 4 Transdermal Drug Delivary System (1)Randa OmdaNo ratings yet
- Chapter 5 - Transes PDFDocument3 pagesChapter 5 - Transes PDFMervi SarsonasNo ratings yet
- Free-Living Amoebas & Ciliates (Lab)Document10 pagesFree-Living Amoebas & Ciliates (Lab)Xie LianNo ratings yet
- MYCOLOGYDocument5 pagesMYCOLOGYRusselNo ratings yet
- Transport MembranDocument40 pagesTransport MembranFitri Nurussani AuliaNo ratings yet
- Cell Structures. Dacawe 2017 PDFDocument6 pagesCell Structures. Dacawe 2017 PDFdanicaNo ratings yet
- Biological Surveillance of Aquatic ToxicantsDocument27 pagesBiological Surveillance of Aquatic ToxicantsGC Photo StateNo ratings yet
- Principles and Practice of Skin ToxicologyFrom EverandPrinciples and Practice of Skin ToxicologyRobert ChilcottNo ratings yet
- Macrophage, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandMacrophage, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Esports - Historical Review Current State and Future ChallengesDocument25 pagesEsports - Historical Review Current State and Future Challengeskassim AliNo ratings yet
- Analytical Methods Used For The Detection andDocument11 pagesAnalytical Methods Used For The Detection andkassim AliNo ratings yet
- Destroying of Islamic UnityDocument8 pagesDestroying of Islamic Unitykassim AliNo ratings yet
- Comparison of LC-MS-MS and GC-MS Analysis of Benzodiazepine Compounds Included in The Drug Demand Reduction Analysis ProgramDocument7 pagesComparison of LC-MS-MS and GC-MS Analysis of Benzodiazepine Compounds Included in The Drug Demand Reduction Analysis Programkassim AliNo ratings yet
- The Virtues of Fasting - Fasting Is A Protection From Lusts and Atonement of Sins - Topics On Fasting - Islamic ShariahDocument8 pagesThe Virtues of Fasting - Fasting Is A Protection From Lusts and Atonement of Sins - Topics On Fasting - Islamic Shariahkassim AliNo ratings yet
- The Crucifixion of JesusDocument6 pagesThe Crucifixion of Jesuskassim AliNo ratings yet
- Propaganda TechniquesDocument12 pagesPropaganda Techniqueskassim AliNo ratings yet
- Analysis of Polar Agents by LC/MSDocument16 pagesAnalysis of Polar Agents by LC/MSkassim AliNo ratings yet
- Multidimention Why Need More ResearchDocument14 pagesMultidimention Why Need More Researchkassim AliNo ratings yet
- PrvaslbchklstDocument4 pagesPrvaslbchklstkassim AliNo ratings yet
- Safety Services Brochure Single PageDocument12 pagesSafety Services Brochure Single Pagekassim AliNo ratings yet
- Drug Detection in Exhaled BreathDocument25 pagesDrug Detection in Exhaled Breathkassim AliNo ratings yet
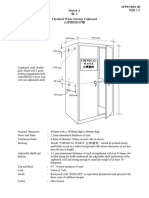
- Chemical Waste Storage CupboardDocument5 pagesChemical Waste Storage Cupboardkassim AliNo ratings yet
- Content Sheet 4-1: Purchasing and Inventory Overview: Role in Quality Management SystemsDocument11 pagesContent Sheet 4-1: Purchasing and Inventory Overview: Role in Quality Management Systemskassim AliNo ratings yet
- Chemical Waste Handling Procedures For Secondary School Science LaboratoriesDocument15 pagesChemical Waste Handling Procedures For Secondary School Science Laboratorieskassim AliNo ratings yet
- Proposal Form: 2013 Student Technology Fee (STF)Document10 pagesProposal Form: 2013 Student Technology Fee (STF)kassim AliNo ratings yet
- Barbosa 2020Document9 pagesBarbosa 2020kassim AliNo ratings yet
- Implementation of QA: 520 Days?Document5 pagesImplementation of QA: 520 Days?kassim AliNo ratings yet
- Charges For Technology: A ProposalDocument7 pagesCharges For Technology: A Proposalkassim AliNo ratings yet
- ChromatographyDocument35 pagesChromatographykassim AliNo ratings yet
- Anatomy and Human Physiology: Module 1: Introduction To The Human Body & Organization and General Plan of The BodyDocument10 pagesAnatomy and Human Physiology: Module 1: Introduction To The Human Body & Organization and General Plan of The BodyLloyd Yap AloNo ratings yet
- Stanley L. Erlandsen Jean E. Magney-Human Histology A Microfiche Atlas Volume 1 Cells and Tissues-University of Minnesota Press (1985)Document92 pagesStanley L. Erlandsen Jean E. Magney-Human Histology A Microfiche Atlas Volume 1 Cells and Tissues-University of Minnesota Press (1985)Rashed HassounNo ratings yet
- Hole's Essentials of Human Anatomy & Physiology: David Shier Jackie Butler Ricki LewisDocument24 pagesHole's Essentials of Human Anatomy & Physiology: David Shier Jackie Butler Ricki LewisChristopher FrigoNo ratings yet
- Skin Lesions SummaryDocument6 pagesSkin Lesions Summarypattydump11No ratings yet
- Double Staining MethodDocument23 pagesDouble Staining Methodarifinuntan100% (1)
- ANAPHY Lec Session #4 - SAS (Agdana, Nicole Ken)Document10 pagesANAPHY Lec Session #4 - SAS (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- Skin and Body MembranesDocument44 pagesSkin and Body MembranesDaniel Redd Rele�asNo ratings yet
- وسام عوض Benign Skin Tumor-5 (Muhadharaty)Document6 pagesوسام عوض Benign Skin Tumor-5 (Muhadharaty)Alaa AhmedNo ratings yet
- BiologyDocument20 pagesBiologypubg. comNo ratings yet
- Case Study Open FractureDocument56 pagesCase Study Open FractureEimereen Montebon Pileo100% (1)
- Integumentary System Terminology WorksheetDocument2 pagesIntegumentary System Terminology WorksheetfernandaNo ratings yet
- Pathology Outlines - PsoriasisDocument1 pagePathology Outlines - PsoriasisCaryl DagamiNo ratings yet
- English Modul Grade Ix SMP St. Bellarminus BekasiDocument20 pagesEnglish Modul Grade Ix SMP St. Bellarminus BekasiPadmaa WatiiNo ratings yet
- Topical Corticosteroids BinderDocument108 pagesTopical Corticosteroids BinderElena DragomirNo ratings yet
- NIH Public Access: Author ManuscriptDocument24 pagesNIH Public Access: Author ManuscriptAnonymous hTivgzixVNNo ratings yet
- BioStine Hydroxide-GSA Powerpoint (En)Document26 pagesBioStine Hydroxide-GSA Powerpoint (En)masumi.rndNo ratings yet
- Anatomy Physiology and Disease For The Health Professions 3rd Edition Booth Solutions Manual Full Chapter PDFDocument34 pagesAnatomy Physiology and Disease For The Health Professions 3rd Edition Booth Solutions Manual Full Chapter PDFrelatermotifef4oq100% (15)
- Anatomi, Eflouresensi KulitDocument67 pagesAnatomi, Eflouresensi KulitWhydia Wedha SutedjaNo ratings yet
- Anatomy and Physiology Transes ReviewerDocument14 pagesAnatomy and Physiology Transes ReviewerYsa Mae Lomibao VillanuevaNo ratings yet
- WHO Monographs On Selected Medicinal Plants Vol 3Document390 pagesWHO Monographs On Selected Medicinal Plants Vol 3Andrew Nugroho100% (1)
- Requisites in Dearmatology - Dermatopathology (PDF) (Tahir99) VRG (Dragged) 12 PDFDocument1 pageRequisites in Dearmatology - Dermatopathology (PDF) (Tahir99) VRG (Dragged) 12 PDFJUSASBNo ratings yet
- Complications and Posttreatment Care Following Invasive Laser Skin Resurfacing 2017Document12 pagesComplications and Posttreatment Care Following Invasive Laser Skin Resurfacing 2017Thảo NguyễnNo ratings yet
- Skin Hydration-A Review On Its Molecular MechanismsDocument8 pagesSkin Hydration-A Review On Its Molecular MechanismsVinicius MelloNo ratings yet
- Nursing Care Plan of Integument SystemDocument27 pagesNursing Care Plan of Integument SystemAlfianGafar67% (3)












































































































Download as pdf or txt
You might also like
- The Skincare Bible PDFDocument156 pagesThe Skincare Bible PDFLacramioara Valentina100% (12)
- Anatomy One Pager G&aDocument2 pagesAnatomy One Pager G&aJennaNo ratings yet
- Integumentary System ReviewerDocument12 pagesIntegumentary System ReviewerLly Isidoro100% (2)
- Chapter 07 IntegumentaryDocument4 pagesChapter 07 IntegumentaryBernard Paul Guinto50% (2)
- Microblading ManualDocument6 pagesMicroblading ManualPaulina Pineda100% (1)
- Combination of Microneedling and Glycolic Acid Peels For TheDocument7 pagesCombination of Microneedling and Glycolic Acid Peels For Thealejandrogonzalez89No ratings yet
- Absorption and Extraction of ToxinDocument22 pagesAbsorption and Extraction of Toxinabhishekranjan090202No ratings yet
- Pharmacokinetics ProcessDocument11 pagesPharmacokinetics ProcesstitusNo ratings yet
- Absorption and Distribution of Toxicants - L4Document3 pagesAbsorption and Distribution of Toxicants - L4prasad sanjayaNo ratings yet
- Pharmacokinetics Webquest: Kimberly Koon, Pharm. D. Bw733 October 1, 2013Document27 pagesPharmacokinetics Webquest: Kimberly Koon, Pharm. D. Bw733 October 1, 2013كسلان اكتب اسميNo ratings yet
- Topic 5ADocument54 pagesTopic 5AMohd RafiqNo ratings yet
- 2024-EnChem CHAP 5Document30 pages2024-EnChem CHAP 5vuthidieuthaot67No ratings yet
- Transdermal DDSDocument20 pagesTransdermal DDSPC BUGNo ratings yet
- Phardose - Transdermal Drug Delivery SystemDocument25 pagesPhardose - Transdermal Drug Delivery SystemEdrick RamoranNo ratings yet
- Pharmacokinetic, Absorption and Ionisation of DrugsDocument31 pagesPharmacokinetic, Absorption and Ionisation of DrugsAli ElmehdawiNo ratings yet
- 7 Transdermal Drug Delivery SystemDocument59 pages7 Transdermal Drug Delivery Systemwikako9357No ratings yet
- 03.transdermal Drug Delivery SystemsDocument56 pages03.transdermal Drug Delivery SystemsMoganaa LakshmiNo ratings yet
- Trans Dermal Drug DeliveryDocument47 pagesTrans Dermal Drug Deliverysouvik maitiNo ratings yet
- 295 PDFDocument6 pages295 PDFHaola andaniNo ratings yet
- Unit 1Document13 pagesUnit 1parmarkeval1610No ratings yet
- Drug Delevery SystemDocument47 pagesDrug Delevery SystempravincrNo ratings yet
- Organophosphate PoisoningDocument24 pagesOrganophosphate PoisoningScribdTranslationsNo ratings yet
- AbsorptionDocument61 pagesAbsorptionGreenNo ratings yet
- Ico Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanDocument34 pagesIco Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanMelkamu AyeNo ratings yet
- Transdermal Drug Delivery System: Shirode Rahul ADocument37 pagesTransdermal Drug Delivery System: Shirode Rahul AFrancisco MarcanoNo ratings yet
- Semester Test 1 NotesDocument23 pagesSemester Test 1 NotesElla BoyceNo ratings yet
- Semisolids Ointment Updated Final-1Document21 pagesSemisolids Ointment Updated Final-1Sunjida Ali RiyaNo ratings yet
- Polymer Membranes in Biomedical FieldDocument35 pagesPolymer Membranes in Biomedical FieldAbufathima CheruvadiNo ratings yet
- Prokaryotic & Eukaryotic Cells - 3Document47 pagesProkaryotic & Eukaryotic Cells - 3AnaNo ratings yet
- Integrated Vector Control Approach: Dr. Kulrajat BhasinDocument37 pagesIntegrated Vector Control Approach: Dr. Kulrajat BhasinPallabi DasguptaNo ratings yet
- Biopharmaceutics Lecture 2 UquDocument36 pagesBiopharmaceutics Lecture 2 Uquرنا الشريفNo ratings yet
- Transdermal Drug Delivery SystemDocument40 pagesTransdermal Drug Delivery SystemDewang PatilNo ratings yet
- Week 2 - Drugs and The BodyDocument18 pagesWeek 2 - Drugs and The BodyDino MicaNo ratings yet
- Transdermaldrugdeliverysystem FinalDocument84 pagesTransdermaldrugdeliverysystem Finalsowjanya kNo ratings yet
- TDDSDocument82 pagesTDDSVouge ModeNo ratings yet
- Annotated-CHIU, CHERYL S. - exeRCISE 2 - Transport ProcessesDocument4 pagesAnnotated-CHIU, CHERYL S. - exeRCISE 2 - Transport ProcessesCheryl ChiuNo ratings yet
- Chapter 11 Transdermal Drug Delivery SystemDocument3 pagesChapter 11 Transdermal Drug Delivery SystemluisynonNo ratings yet
- Wound Management and Aftercare: Oral & Maxillofacial SurgeryDocument33 pagesWound Management and Aftercare: Oral & Maxillofacial Surgerymehul7patel-10No ratings yet
- Phase I: Chemical Modifications That Introduce or Uncover Functional Groups On A XenobioticDocument5 pagesPhase I: Chemical Modifications That Introduce or Uncover Functional Groups On A XenobioticBlue SaphyrNo ratings yet
- Introduction To Bio PharmaceuticsDocument88 pagesIntroduction To Bio PharmaceuticsSohan PrasathNo ratings yet
- Good Morning Class: - DR MehnazDocument42 pagesGood Morning Class: - DR MehnazUzair KhanNo ratings yet
- Gram Positive Rod of Medical Imortance IIDocument36 pagesGram Positive Rod of Medical Imortance IIJoeyNo ratings yet
- Unit.1 Absorption-Mechanisms of Drug Absorption Through GIT.Document25 pagesUnit.1 Absorption-Mechanisms of Drug Absorption Through GIT.deepshah6068No ratings yet
- Routes of Drug AdministrationDocument6 pagesRoutes of Drug AdministrationKena SamuelNo ratings yet
- BP604T Lecturer's Slides - CompressedDocument119 pagesBP604T Lecturer's Slides - CompressedGyampoh SolomonNo ratings yet
- Neeraj Assignment PDFDocument68 pagesNeeraj Assignment PDFNeeraj GautamNo ratings yet
- IntroductionDocument18 pagesIntroductionsai projectNo ratings yet
- Principles of Toxicology and Basic Treatment: PWM Olly Indrajani 2014Document22 pagesPrinciples of Toxicology and Basic Treatment: PWM Olly Indrajani 2014Princes Mentari Dwi NurainiNo ratings yet
- Paralec M1Document8 pagesParalec M1VE NI CENo ratings yet
- Transdermal Drug Delivery SystemDocument47 pagesTransdermal Drug Delivery SystemMridul AroraNo ratings yet
- Pharmacokinetics: Sun Yi Department of PharmacologyDocument53 pagesPharmacokinetics: Sun Yi Department of PharmacologyMOHAMMAD NAZMUL ISLAMNo ratings yet
- UNIT 2 - Week (4-5) : Mechanisms of Toxicity & Toxicokinetics Intended Learning Outcomes (ILO)Document8 pagesUNIT 2 - Week (4-5) : Mechanisms of Toxicity & Toxicokinetics Intended Learning Outcomes (ILO)Hannah Jean Lapenid LemorenasNo ratings yet
- Bio136 186Unit3P2Document89 pagesBio136 186Unit3P2jhon pauloNo ratings yet
- Endocrine GlandsDocument13 pagesEndocrine GlandsAyesha Jalal KhanNo ratings yet
- Chapter 2Document9 pagesChapter 2jjumlaboratoryNo ratings yet
- Biomedical Nanotechnology: Lecture 18: Cellular Uptake Mechanisms of NanomaterialsDocument43 pagesBiomedical Nanotechnology: Lecture 18: Cellular Uptake Mechanisms of NanomaterialsDURGA DEVI T 037 BME100% (1)
- Micro Microbial Mechanisms of Pathogenicity NOTESDocument6 pagesMicro Microbial Mechanisms of Pathogenicity NOTESAriane NobleNo ratings yet
- Unit 4 Transdermal Drug Delivary System (1)Document42 pagesUnit 4 Transdermal Drug Delivary System (1)Randa OmdaNo ratings yet
- Chapter 5 - Transes PDFDocument3 pagesChapter 5 - Transes PDFMervi SarsonasNo ratings yet
- Free-Living Amoebas & Ciliates (Lab)Document10 pagesFree-Living Amoebas & Ciliates (Lab)Xie LianNo ratings yet
- MYCOLOGYDocument5 pagesMYCOLOGYRusselNo ratings yet
- Transport MembranDocument40 pagesTransport MembranFitri Nurussani AuliaNo ratings yet
- Cell Structures. Dacawe 2017 PDFDocument6 pagesCell Structures. Dacawe 2017 PDFdanicaNo ratings yet
- Biological Surveillance of Aquatic ToxicantsDocument27 pagesBiological Surveillance of Aquatic ToxicantsGC Photo StateNo ratings yet
- Principles and Practice of Skin ToxicologyFrom EverandPrinciples and Practice of Skin ToxicologyRobert ChilcottNo ratings yet
- Macrophage, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandMacrophage, Functions, Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Esports - Historical Review Current State and Future ChallengesDocument25 pagesEsports - Historical Review Current State and Future Challengeskassim AliNo ratings yet
- Analytical Methods Used For The Detection andDocument11 pagesAnalytical Methods Used For The Detection andkassim AliNo ratings yet
- Destroying of Islamic UnityDocument8 pagesDestroying of Islamic Unitykassim AliNo ratings yet
- Comparison of LC-MS-MS and GC-MS Analysis of Benzodiazepine Compounds Included in The Drug Demand Reduction Analysis ProgramDocument7 pagesComparison of LC-MS-MS and GC-MS Analysis of Benzodiazepine Compounds Included in The Drug Demand Reduction Analysis Programkassim AliNo ratings yet
- The Virtues of Fasting - Fasting Is A Protection From Lusts and Atonement of Sins - Topics On Fasting - Islamic ShariahDocument8 pagesThe Virtues of Fasting - Fasting Is A Protection From Lusts and Atonement of Sins - Topics On Fasting - Islamic Shariahkassim AliNo ratings yet
- The Crucifixion of JesusDocument6 pagesThe Crucifixion of Jesuskassim AliNo ratings yet
- Propaganda TechniquesDocument12 pagesPropaganda Techniqueskassim AliNo ratings yet
- Analysis of Polar Agents by LC/MSDocument16 pagesAnalysis of Polar Agents by LC/MSkassim AliNo ratings yet
- Multidimention Why Need More ResearchDocument14 pagesMultidimention Why Need More Researchkassim AliNo ratings yet
- PrvaslbchklstDocument4 pagesPrvaslbchklstkassim AliNo ratings yet
- Safety Services Brochure Single PageDocument12 pagesSafety Services Brochure Single Pagekassim AliNo ratings yet
- Drug Detection in Exhaled BreathDocument25 pagesDrug Detection in Exhaled Breathkassim AliNo ratings yet
- Chemical Waste Storage CupboardDocument5 pagesChemical Waste Storage Cupboardkassim AliNo ratings yet
- Content Sheet 4-1: Purchasing and Inventory Overview: Role in Quality Management SystemsDocument11 pagesContent Sheet 4-1: Purchasing and Inventory Overview: Role in Quality Management Systemskassim AliNo ratings yet
- Chemical Waste Handling Procedures For Secondary School Science LaboratoriesDocument15 pagesChemical Waste Handling Procedures For Secondary School Science Laboratorieskassim AliNo ratings yet
- Proposal Form: 2013 Student Technology Fee (STF)Document10 pagesProposal Form: 2013 Student Technology Fee (STF)kassim AliNo ratings yet
- Barbosa 2020Document9 pagesBarbosa 2020kassim AliNo ratings yet
- Implementation of QA: 520 Days?Document5 pagesImplementation of QA: 520 Days?kassim AliNo ratings yet
- Charges For Technology: A ProposalDocument7 pagesCharges For Technology: A Proposalkassim AliNo ratings yet
- ChromatographyDocument35 pagesChromatographykassim AliNo ratings yet
- Anatomy and Human Physiology: Module 1: Introduction To The Human Body & Organization and General Plan of The BodyDocument10 pagesAnatomy and Human Physiology: Module 1: Introduction To The Human Body & Organization and General Plan of The BodyLloyd Yap AloNo ratings yet
- Stanley L. Erlandsen Jean E. Magney-Human Histology A Microfiche Atlas Volume 1 Cells and Tissues-University of Minnesota Press (1985)Document92 pagesStanley L. Erlandsen Jean E. Magney-Human Histology A Microfiche Atlas Volume 1 Cells and Tissues-University of Minnesota Press (1985)Rashed HassounNo ratings yet
- Hole's Essentials of Human Anatomy & Physiology: David Shier Jackie Butler Ricki LewisDocument24 pagesHole's Essentials of Human Anatomy & Physiology: David Shier Jackie Butler Ricki LewisChristopher FrigoNo ratings yet
- Skin Lesions SummaryDocument6 pagesSkin Lesions Summarypattydump11No ratings yet
- Double Staining MethodDocument23 pagesDouble Staining Methodarifinuntan100% (1)
- ANAPHY Lec Session #4 - SAS (Agdana, Nicole Ken)Document10 pagesANAPHY Lec Session #4 - SAS (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- Skin and Body MembranesDocument44 pagesSkin and Body MembranesDaniel Redd Rele�asNo ratings yet
- وسام عوض Benign Skin Tumor-5 (Muhadharaty)Document6 pagesوسام عوض Benign Skin Tumor-5 (Muhadharaty)Alaa AhmedNo ratings yet
- BiologyDocument20 pagesBiologypubg. comNo ratings yet
- Case Study Open FractureDocument56 pagesCase Study Open FractureEimereen Montebon Pileo100% (1)
- Integumentary System Terminology WorksheetDocument2 pagesIntegumentary System Terminology WorksheetfernandaNo ratings yet
- Pathology Outlines - PsoriasisDocument1 pagePathology Outlines - PsoriasisCaryl DagamiNo ratings yet
- English Modul Grade Ix SMP St. Bellarminus BekasiDocument20 pagesEnglish Modul Grade Ix SMP St. Bellarminus BekasiPadmaa WatiiNo ratings yet
- Topical Corticosteroids BinderDocument108 pagesTopical Corticosteroids BinderElena DragomirNo ratings yet
- NIH Public Access: Author ManuscriptDocument24 pagesNIH Public Access: Author ManuscriptAnonymous hTivgzixVNNo ratings yet
- BioStine Hydroxide-GSA Powerpoint (En)Document26 pagesBioStine Hydroxide-GSA Powerpoint (En)masumi.rndNo ratings yet
- Anatomy Physiology and Disease For The Health Professions 3rd Edition Booth Solutions Manual Full Chapter PDFDocument34 pagesAnatomy Physiology and Disease For The Health Professions 3rd Edition Booth Solutions Manual Full Chapter PDFrelatermotifef4oq100% (15)
- Anatomi, Eflouresensi KulitDocument67 pagesAnatomi, Eflouresensi KulitWhydia Wedha SutedjaNo ratings yet
- Anatomy and Physiology Transes ReviewerDocument14 pagesAnatomy and Physiology Transes ReviewerYsa Mae Lomibao VillanuevaNo ratings yet
- WHO Monographs On Selected Medicinal Plants Vol 3Document390 pagesWHO Monographs On Selected Medicinal Plants Vol 3Andrew Nugroho100% (1)
- Requisites in Dearmatology - Dermatopathology (PDF) (Tahir99) VRG (Dragged) 12 PDFDocument1 pageRequisites in Dearmatology - Dermatopathology (PDF) (Tahir99) VRG (Dragged) 12 PDFJUSASBNo ratings yet
- Complications and Posttreatment Care Following Invasive Laser Skin Resurfacing 2017Document12 pagesComplications and Posttreatment Care Following Invasive Laser Skin Resurfacing 2017Thảo NguyễnNo ratings yet
- Skin Hydration-A Review On Its Molecular MechanismsDocument8 pagesSkin Hydration-A Review On Its Molecular MechanismsVinicius MelloNo ratings yet
- Nursing Care Plan of Integument SystemDocument27 pagesNursing Care Plan of Integument SystemAlfianGafar67% (3)