Download as pdf or txt
You might also like
- Brain Over BodyDocument10 pagesBrain Over BodyJohn LenoNo ratings yet
- Hydro CardiovasDocument39 pagesHydro CardiovasFransiskus Xaverius CungkringNo ratings yet
- Magnetic RefrigerationDocument7 pagesMagnetic RefrigerationhasanNo ratings yet
- Motor and Sensory Nerve ConductionDocument12 pagesMotor and Sensory Nerve ConductionSantiago Mondragon RiosNo ratings yet
- Respuesta Neuro DinamicaDocument6 pagesRespuesta Neuro DinamicaEdwin Trujillo OspinaNo ratings yet
- Effect of Occlusal Splint Treatment On The Temperature of Different Muscles in Patients With TMDDocument5 pagesEffect of Occlusal Splint Treatment On The Temperature of Different Muscles in Patients With TMDMichael KronovNo ratings yet
- Abstracts / Osteoarthritis and Cartilage 27 (2019) S373 Es516 S490Document2 pagesAbstracts / Osteoarthritis and Cartilage 27 (2019) S373 Es516 S490Shella Zulfatima RahmadiniNo ratings yet
- The Anterior Cruciate Ligament: Reconstruction and Basic ScienceDocument6 pagesThe Anterior Cruciate Ligament: Reconstruction and Basic ScienceMourad BennaniNo ratings yet
- Ice Therapy: How Good Is The Evidence?: Orthopedics and Clinical ScienceDocument6 pagesIce Therapy: How Good Is The Evidence?: Orthopedics and Clinical ScienceEva FisioNo ratings yet
- Applsci 11 00097Document15 pagesApplsci 11 00097Nhat TrieuNo ratings yet
- BJSM 2006 031237Document6 pagesBJSM 2006 031237raul carreñoNo ratings yet
- 901 PDFDocument6 pages901 PDFgalihNo ratings yet
- Tenosinovitos de QuerveinDocument8 pagesTenosinovitos de QuerveinEduardo RetamaNo ratings yet
- Delayed Onset Muscle Soreness Neck ShoulderDocument8 pagesDelayed Onset Muscle Soreness Neck ShoulderJorge Campillay GuzmánNo ratings yet
- Artigo Termografia JamacyDocument8 pagesArtigo Termografia Jamacyanon-720083No ratings yet
- 2001 Ice Therapy How Good Is The EvidenceDocument6 pages2001 Ice Therapy How Good Is The EvidenceFrancisco Antonó Castro WeithNo ratings yet
- Investigation of Temperature Effects of A Low-Level Laser Source Within The Muscle PhantomDocument5 pagesInvestigation of Temperature Effects of A Low-Level Laser Source Within The Muscle PhantomInternational Journal of Advances in Applied Sciences (IJAAS)No ratings yet
- The Effects of Kinesio-Taping On Quadriceps Strength During Isokinetic Exercise in Healthy Non Athlete WomenDocument6 pagesThe Effects of Kinesio-Taping On Quadriceps Strength During Isokinetic Exercise in Healthy Non Athlete WomenSurya DiatmikaNo ratings yet
- Jmu 26 194Document6 pagesJmu 26 194Arkar SoeNo ratings yet
- Superficial Thermotherapy CHC, IR, BP.Document12 pagesSuperficial Thermotherapy CHC, IR, BP.ScribdTranslationsNo ratings yet
- The Physiologic Basis and Clinical Applications of CryotherapyDocument6 pagesThe Physiologic Basis and Clinical Applications of CryotherapyomboNo ratings yet
- Thermal Behavior Differs Between Males and Females.18Document12 pagesThermal Behavior Differs Between Males and Females.18GerasimarasNo ratings yet
- Pulsed Shortwave Diathermy and Joint Mobilizations Restore A Twice Fractured Elbow With Metal Implants To Full Range of MotionDocument7 pagesPulsed Shortwave Diathermy and Joint Mobilizations Restore A Twice Fractured Elbow With Metal Implants To Full Range of MotionIndah YulantariNo ratings yet
- Homeostatic Disturbance of Thermoregulatory Functions in Rats With Chronic FatigueDocument6 pagesHomeostatic Disturbance of Thermoregulatory Functions in Rats With Chronic FatigueG ElegansNo ratings yet
- Ankle Cryotherapy Facilitates SoleusDocument6 pagesAnkle Cryotherapy Facilitates SoleusRamiro Avendaño RebolledoNo ratings yet
- Changes in Temperature Following Radiofrequency Thermal Ablation of The Nucleus Pulposus and Annulus Fibrosus: A Cadaveric StudyDocument8 pagesChanges in Temperature Following Radiofrequency Thermal Ablation of The Nucleus Pulposus and Annulus Fibrosus: A Cadaveric StudyMARCOS HUACONo ratings yet
- Fisiological Effects - JosptDocument8 pagesFisiological Effects - Josptcarlla728No ratings yet
- Immune Effects of Cold ExposureDocument12 pagesImmune Effects of Cold ExposurePAPA HURCONo ratings yet
- Warm-Up Reduces Delayed-Onset Muscle Soreness But Cool-Down Does Not: A Randomised Controlled TrialDocument5 pagesWarm-Up Reduces Delayed-Onset Muscle Soreness But Cool-Down Does Not: A Randomised Controlled TrialAgustinus VincentNo ratings yet
- MET Vs ConventionalDocument6 pagesMET Vs ConventionalPoorvin ShahNo ratings yet
- Geurts 2005 CGP2Document8 pagesGeurts 2005 CGP2maggie305No ratings yet
- Effects of Dry Needling On Calf Muscle in Case of Myofascial Trigger Point With Mild Restriction of Knee Joint Movement: A Case StudyDocument4 pagesEffects of Dry Needling On Calf Muscle in Case of Myofascial Trigger Point With Mild Restriction of Knee Joint Movement: A Case StudyIJAR JOURNALNo ratings yet
- Thermal Imaging of An Ice Burn Over The Patella Following Clinically Relevant Cryotherapy Application During A Clinical Research StudyDocument6 pagesThermal Imaging of An Ice Burn Over The Patella Following Clinically Relevant Cryotherapy Application During A Clinical Research StudyhanadilahNo ratings yet
- Agulhamento Seco No Alívio Da Dor Lombalgia Dry Needling BOXEDocument7 pagesAgulhamento Seco No Alívio Da Dor Lombalgia Dry Needling BOXEtaki47685No ratings yet
- Version of Record Doi: 10.1111/EVJ.13278Document21 pagesVersion of Record Doi: 10.1111/EVJ.13278DBZ beatzNo ratings yet
- 7 Parolo & Onesta Tecar in Acute & Chronic Musculo Skeletal Lesions 60 Patient SeriesDocument6 pages7 Parolo & Onesta Tecar in Acute & Chronic Musculo Skeletal Lesions 60 Patient SeriesSilvia PluisNo ratings yet
- Ijpr 2022 156Document5 pagesIjpr 2022 156winda athyaNo ratings yet
- Postinflammatory Hyperpigmentation After Human.2Document4 pagesPostinflammatory Hyperpigmentation After Human.2Anida HasnaNo ratings yet
- Thermography in Dentistry-RevisitedDocument5 pagesThermography in Dentistry-RevisitedkittumdsNo ratings yet
- Preclinical Assessment of Tissue Effects by Gastrointestinal Endoscope Tip TemperatureDocument10 pagesPreclinical Assessment of Tissue Effects by Gastrointestinal Endoscope Tip TemperatureOisin McGleenanNo ratings yet
- The Effect of Thermal Insulation Pads On Heat Flux, Physical Effort and Perceived Exertion During Endurance Exercise in Cool EnvironmentsDocument12 pagesThe Effect of Thermal Insulation Pads On Heat Flux, Physical Effort and Perceived Exertion During Endurance Exercise in Cool EnvironmentstomNo ratings yet
- Physical Agent Modalities in PTDocument16 pagesPhysical Agent Modalities in PTlauris881106No ratings yet
- 12 - Santos Et Al (2014) - TERMOGRAFIA NA FISIOTERAPIA REVIEWDocument8 pages12 - Santos Et Al (2014) - TERMOGRAFIA NA FISIOTERAPIA REVIEWHenrique Martins FilhoNo ratings yet
- Sex Difference in Cold Perception and Shivering Onset Upon Gradual Cold ExposureDocument9 pagesSex Difference in Cold Perception and Shivering Onset Upon Gradual Cold ExposureAzizi AlfyanNo ratings yet
- Yao 2015 - Sensory Cortical Re-Mapping Following Upper-Limb Amputation and Subsequent Targeted Reinnervation A Case ReportDocument8 pagesYao 2015 - Sensory Cortical Re-Mapping Following Upper-Limb Amputation and Subsequent Targeted Reinnervation A Case ReportDaniel BoariNo ratings yet
- The Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersDocument3 pagesThe Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mode of Action of Cupping - Local Metabolism and Pain Thresholds in Neck Pain Patients and Healthy SubjectsDocument14 pagesMode of Action of Cupping - Local Metabolism and Pain Thresholds in Neck Pain Patients and Healthy Subjectsdwi putri ratehNo ratings yet
- Ice Freezes Pain A Review of The Clinical Effectiveness of Analgesic Cold PDFDocument4 pagesIce Freezes Pain A Review of The Clinical Effectiveness of Analgesic Cold PDFMatin Abdillah GogaNo ratings yet
- Detection of Acute Stress by Smooth Muscle Electromyography PDFDocument9 pagesDetection of Acute Stress by Smooth Muscle Electromyography PDFMarco mNo ratings yet
- Does Sex Have An Independant Effect On Thermoeffector Responses During Exercise in The HeatDocument11 pagesDoes Sex Have An Independant Effect On Thermoeffector Responses During Exercise in The HeateposterproductionsNo ratings yet
- Effects of Acute Dehydration On Neuromuscular Responses of Exercised and Nonexercised Muscles After Exercise in The HeatDocument6 pagesEffects of Acute Dehydration On Neuromuscular Responses of Exercised and Nonexercised Muscles After Exercise in The HeatCarlos EmilioNo ratings yet
- Thermal Imaging Bowen TherapyDocument15 pagesThermal Imaging Bowen TherapyMagdallinaNo ratings yet
- Manual Therapy: Original ArticleDocument5 pagesManual Therapy: Original ArticleCleber PimentaNo ratings yet
- Effect of A Hydrotherapy Based Alternate Compress On Osteoarthritis of The Knee Joint: A Randomized Controlled TrialDocument14 pagesEffect of A Hydrotherapy Based Alternate Compress On Osteoarthritis of The Knee Joint: A Randomized Controlled TrialYuni fahllefyNo ratings yet
- Ntrk1 Molecular Genetic Testing.: Ngf-Dependent Neurons and The Role of TrkaDocument3 pagesNtrk1 Molecular Genetic Testing.: Ngf-Dependent Neurons and The Role of TrkaPan DjeroNo ratings yet
- The Context of Noxious StimulusDocument8 pagesThe Context of Noxious StimulusHossam BarghashNo ratings yet
- Efficacy of Cubed-Ice and Wetted-Ice As A Cryotherapeutic Agent in The Malaysian ClimateDocument9 pagesEfficacy of Cubed-Ice and Wetted-Ice As A Cryotherapeutic Agent in The Malaysian ClimateEva FisioNo ratings yet
- Giustini - Siracusa 2016Document23 pagesGiustini - Siracusa 2016sabina vladeanuNo ratings yet
- FascialFitness in DaltonDocument12 pagesFascialFitness in DaltonQuiroprácticaParaTodosNo ratings yet
- Bove 2012 Visc Mobiliz Adhesion RatDocument7 pagesBove 2012 Visc Mobiliz Adhesion RatQuiroprácticaParaTodosNo ratings yet
- Acordes PDFDocument1 pageAcordes PDFQuiroprácticaParaTodosNo ratings yet
- Bove-Chapelle ViscMobilizAdhesionRatDocument7 pagesBove-Chapelle ViscMobilizAdhesionRatQuiroprácticaParaTodosNo ratings yet
- Bordoni 2014 Fascial SystemDocument11 pagesBordoni 2014 Fascial SystemQuiroprácticaParaTodosNo ratings yet
- ChaitowBook ExcerptDocument9 pagesChaitowBook ExcerptQuiroprácticaParaTodosNo ratings yet
- 10 1097@PHM 0000000000001048Document28 pages10 1097@PHM 0000000000001048QuiroprácticaParaTodosNo ratings yet
- Bruggmann2010 IntraabdomadhesionsDocument10 pagesBruggmann2010 IntraabdomadhesionsQuiroprácticaParaTodosNo ratings yet
- MovilizacionDocument6 pagesMovilizacionQuiroprácticaParaTodosNo ratings yet
- Prevalencia Hernias 2022Document9 pagesPrevalencia Hernias 2022QuiroprácticaParaTodosNo ratings yet
- Chiropractic Instrumental Manipulation in The Lower Back: A Systematic ReviewDocument6 pagesChiropractic Instrumental Manipulation in The Lower Back: A Systematic ReviewQuiroprácticaParaTodosNo ratings yet
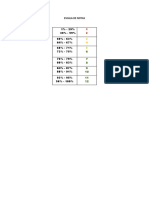
- Escala de NotasDocument1 pageEscala de NotasQuiroprácticaParaTodosNo ratings yet
- Accepted Manuscript: Journal of BiomechanicsDocument42 pagesAccepted Manuscript: Journal of BiomechanicsQuiroprácticaParaTodosNo ratings yet
- Bilg Il I Soy Filiz 2018Document28 pagesBilg Il I Soy Filiz 2018QuiroprácticaParaTodosNo ratings yet
- A Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyDocument8 pagesA Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyQuiroprácticaParaTodosNo ratings yet
- PDF 60574 4818Document13 pagesPDF 60574 4818QuiroprácticaParaTodosNo ratings yet
- Thoracolumbar Rotation During Tai Chi Movements-A Biomechanical Analysis of The Entire Peking Style RoutineDocument7 pagesThoracolumbar Rotation During Tai Chi Movements-A Biomechanical Analysis of The Entire Peking Style RoutineQuiroprácticaParaTodosNo ratings yet
- Journal of Integrative Medicine: ReviewDocument6 pagesJournal of Integrative Medicine: ReviewQuiroprácticaParaTodosNo ratings yet
- Houghton 2013Document11 pagesHoughton 2013QuiroprácticaParaTodosNo ratings yet
- Work-Related Thumb Pain in Physiotherapists Is Associated With Thumb Alignment During Performance of PA PressuresDocument5 pagesWork-Related Thumb Pain in Physiotherapists Is Associated With Thumb Alignment During Performance of PA PressuresQuiroprácticaParaTodosNo ratings yet
- Perspective: Discriminative and Affective Touch: Sensing and FeelingDocument19 pagesPerspective: Discriminative and Affective Touch: Sensing and FeelingQuiroprácticaParaTodosNo ratings yet
- Human Movement Science: Brian C. Nairn, Janessa D.M. DrakeDocument11 pagesHuman Movement Science: Brian C. Nairn, Janessa D.M. DrakeQuiroprácticaParaTodosNo ratings yet
- E041433 FullDocument15 pagesE041433 FullQuiroprácticaParaTodosNo ratings yet
- Parker 2020Document6 pagesParker 2020QuiroprácticaParaTodosNo ratings yet
- Effect of Low Back Pain On The Muscles Controlling The Sitting PostureDocument4 pagesEffect of Low Back Pain On The Muscles Controlling The Sitting PostureQuiroprácticaParaTodosNo ratings yet
- Scapular Dyskinesia, The Forgotten Culprit of Shoulder Pain and How To RehabilitateDocument6 pagesScapular Dyskinesia, The Forgotten Culprit of Shoulder Pain and How To RehabilitateQuiroprácticaParaTodosNo ratings yet
- Does The Addition of Visceral Manipulation Alter Outcomes For Patients With Low Back Pain? A Randomized Placebo Controlled TrialDocument9 pagesDoes The Addition of Visceral Manipulation Alter Outcomes For Patients With Low Back Pain? A Randomized Placebo Controlled TrialQuiroprácticaParaTodosNo ratings yet
- Urinary IncontinenceDocument5 pagesUrinary IncontinencefakrulnersmudaNo ratings yet
- Drugs Used in Pregnancy, Labour and Puerperium: Presented By:-Ms Lisa Chadha F.Y. MSC Nursing Bvcon, PuneDocument87 pagesDrugs Used in Pregnancy, Labour and Puerperium: Presented By:-Ms Lisa Chadha F.Y. MSC Nursing Bvcon, PuneSanjay Kumar SanjuNo ratings yet
- Breast Cancer Atlas of Clinical OncologyDocument300 pagesBreast Cancer Atlas of Clinical OncologyQueenIchma ChualunaeonelophNo ratings yet
- Physiology, Lecture 6, Gas Exchange (Lecture Notes)Document14 pagesPhysiology, Lecture 6, Gas Exchange (Lecture Notes)Ali Al-QudsiNo ratings yet
- Hot Tub Folliculitis: Symptoms and CausesDocument5 pagesHot Tub Folliculitis: Symptoms and CausesDennis NjorogeNo ratings yet
- STS Gene TherapyDocument12 pagesSTS Gene Therapyedgar malupengNo ratings yet
- Arterial Blood PressureDocument46 pagesArterial Blood PressureRupasi KathiravanNo ratings yet
- Week - 7 Rle 312Document5 pagesWeek - 7 Rle 312VAL ASHLIE ACEBARNo ratings yet
- Enf Tiroidea y Embarazo Lancet 2018Document12 pagesEnf Tiroidea y Embarazo Lancet 2018Jair Alexander Quintero PanucoNo ratings yet
- Amoebiasis - and GiardiasisDocument59 pagesAmoebiasis - and GiardiasisSaurabh AgarwalNo ratings yet
- Template 01.03.2021Document9 pagesTemplate 01.03.2021statenvhcp rajasthanNo ratings yet
- Family Relationships and Mental Illness: IssuesDocument19 pagesFamily Relationships and Mental Illness: IssuesneetiprakashNo ratings yet
- Lecture 1-Geriatrics INTRODocument26 pagesLecture 1-Geriatrics INTRORao SahabNo ratings yet
- Etiology: 1. Compare Lobar Pneumonia With Lobular Pneumonia On The ListDocument3 pagesEtiology: 1. Compare Lobar Pneumonia With Lobular Pneumonia On The Listselam kalayuNo ratings yet
- Placenta AcretaDocument5 pagesPlacenta AcretaFrancisca MoennigNo ratings yet
- 83K English Class Examination Questions of Infectious DiseaseDocument23 pages83K English Class Examination Questions of Infectious Diseasetarun956519No ratings yet
- Exam 4Document10 pagesExam 4Hasan A AsFourNo ratings yet
- Final TCS ModuleDocument24 pagesFinal TCS Modulemae cudalNo ratings yet
- Morning Report: Dr. Dikara WS Maulidy, SP - PDDocument24 pagesMorning Report: Dr. Dikara WS Maulidy, SP - PDBethari Abi SafitriNo ratings yet
- Sistem DigestifDocument17 pagesSistem DigestifleilaNo ratings yet
- Protap NTG DripDocument4 pagesProtap NTG DripAinil MardiahNo ratings yet
- Paxil: Generic Name: Paroxetine HydrochlorideDocument3 pagesPaxil: Generic Name: Paroxetine Hydrochloridenasir khanNo ratings yet
- Hubungan Kadar Interleukin 6 Dan Interleukin 10 Serum Pada Pasien Cedera Otak Berat Akibat TraumaDocument9 pagesHubungan Kadar Interleukin 6 Dan Interleukin 10 Serum Pada Pasien Cedera Otak Berat Akibat TraumaanggiNo ratings yet
- 277 2010 Article 908Document11 pages277 2010 Article 908Mochamad HuseinNo ratings yet
- Eye Essentials Cataract Assessment Classification and Management PDFDocument245 pagesEye Essentials Cataract Assessment Classification and Management PDFihsansiregarNo ratings yet
- Pediatrics in Review - February2011Document86 pagesPediatrics in Review - February2011Manuel AlvaradoNo ratings yet
- MCI SyllabusDocument6 pagesMCI SyllabusloocasjNo ratings yet
- Chemotherapeutic Drug Induced Nail Changes A Prospective Observational StudyDocument5 pagesChemotherapeutic Drug Induced Nail Changes A Prospective Observational StudyDr SrigopalNo ratings yet
- Digital Eye Care and Teleophthalmology Practical Guide To Applications - 3031240510Document524 pagesDigital Eye Care and Teleophthalmology Practical Guide To Applications - 3031240510Manci PeterNo ratings yet
- Set 1 1. Please Tell Us A Little About You.: Blood Donation SurveyDocument2 pagesSet 1 1. Please Tell Us A Little About You.: Blood Donation SurveyHisyam AhmadNo ratings yet