Download as pdf or txt
You might also like
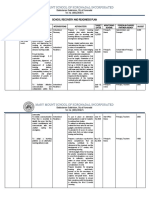
- School Recovery and Readiness PlanDocument6 pagesSchool Recovery and Readiness PlanTeàcher Peach95% (42)
- Lect 3 Trauma CounsellingDocument28 pagesLect 3 Trauma Counsellingumibrahim78% (9)
- DR SolomonDocument23 pagesDR SolomonAnocas PereiraNo ratings yet
- Crisis & Its InterventionDocument13 pagesCrisis & Its InterventionAncy Varkey100% (1)
- Printable Conference Programme, Paris July 2012Document15 pagesPrintable Conference Programme, Paris July 2012tprugNo ratings yet
- Social Work Theory and Methods Comparison TableDocument9 pagesSocial Work Theory and Methods Comparison Tablesanju100% (2)
- Topic 15 The Experience of Loss and Grief, GW 2023-2024, ZU NursingDocument22 pagesTopic 15 The Experience of Loss and Grief, GW 2023-2024, ZU Nursingamosae909No ratings yet
- Psychotherapeutic Modalities (Crisis) : Psychopathology 1 SHRMNDocument39 pagesPsychotherapeutic Modalities (Crisis) : Psychopathology 1 SHRMNPinkRose BrownSpiceNo ratings yet
- Crisis Theory and Phases of DevelopmentDocument6 pagesCrisis Theory and Phases of DevelopmentNic Korapat100% (1)
- Crisis 7Document24 pagesCrisis 7عبدالله سعيدNo ratings yet
- 1.crisis InterventionDocument48 pages1.crisis Interventionsivagiri.p100% (1)
- Grief TherapyDocument15 pagesGrief Therapygauri pillaiNo ratings yet
- Crisis Theory ReportDocument26 pagesCrisis Theory ReportJohan VelicariaNo ratings yet
- Review 2 Final Sp2011 PDFDocument60 pagesReview 2 Final Sp2011 PDFSeiko Matsuura HirataNo ratings yet
- Series 1.9 Prevention and Intervention For At-Risk IndividualsDocument47 pagesSeries 1.9 Prevention and Intervention For At-Risk IndividualsMydearina MaidilNo ratings yet
- Trauma and Coping StrategiesDocument12 pagesTrauma and Coping StrategiesProf. Lakshman Madurasinghe100% (24)
- Masterclass On Grief and LossDocument27 pagesMasterclass On Grief and LosspsychaidconsultsNo ratings yet
- MRC Psychology of DisasterDocument37 pagesMRC Psychology of DisasterL Duane Brand100% (1)
- Crisis Intervention AmaDocument19 pagesCrisis Intervention AmaHoque Mohammed Newaz ShorifulNo ratings yet
- Lect 18 The Trauma of RapeDocument23 pagesLect 18 The Trauma of RapeumibrahimNo ratings yet
- Understanding The Psychosocial Impact of Disasters With LectureDocument25 pagesUnderstanding The Psychosocial Impact of Disasters With LectureArvie ReyesNo ratings yet
- Traumaattachmentdsm 0717Document88 pagesTraumaattachmentdsm 0717Shadi AbualkibashNo ratings yet
- Bab I1Document20 pagesBab I1Mey RahmawatiNo ratings yet
- Adjustment To Disability - AmputationDocument29 pagesAdjustment To Disability - AmputationptannenbaumNo ratings yet
- Grief Crisis 1Document10 pagesGrief Crisis 1Sampreeta KaurNo ratings yet
- Kuliah 6 HELPING SKILLS FOR CRISIS-180209 - 023225-220911 - 085239Document26 pagesKuliah 6 HELPING SKILLS FOR CRISIS-180209 - 023225-220911 - 085239Mejar Jeneral WafiyNo ratings yet
- Patient Safety in Psychiatric WardDocument38 pagesPatient Safety in Psychiatric WardajishNo ratings yet
- Bereavement and DepressionDocument11 pagesBereavement and DepressionAdrian Levi MagbojosNo ratings yet
- NTIMATE PARTNER ViolenceDocument34 pagesNTIMATE PARTNER Violencesanfranciscojulie22No ratings yet
- NCM 117M Trauma and Stressor Related Disorder DSM5Document58 pagesNCM 117M Trauma and Stressor Related Disorder DSM5Amirrah LaurenteNo ratings yet
- Psyche Prefinal CrisisDocument5 pagesPsyche Prefinal CrisisAziil LiizaNo ratings yet
- Chapter-29: Care of Terminally Ill PatientDocument92 pagesChapter-29: Care of Terminally Ill PatientMuhammad MuhammadNo ratings yet
- Death & GriefDocument20 pagesDeath & GriefEleanorNo ratings yet
- Social Psychology in The ClinicDocument18 pagesSocial Psychology in The ClinicRonald GaboNo ratings yet
- Grief Resolution TherapyDocument51 pagesGrief Resolution TherapySandesh HegdeNo ratings yet
- 5 - Illness BehaviorDocument19 pages5 - Illness BehaviorZackNo ratings yet
- Loss, Grief and Grieving ProcessDocument28 pagesLoss, Grief and Grieving ProcessSuper .K. music lyricsNo ratings yet
- Helping Others Cope With TraumaDocument8 pagesHelping Others Cope With TraumaDan TNo ratings yet
- Grief and TraumaDocument34 pagesGrief and TraumaMaheen ShahidNo ratings yet
- Human Behavior 2 2Document42 pagesHuman Behavior 2 2Lindy TamposNo ratings yet
- APP3015 Session 6 Presentation - Person-Centred TherapiesDocument44 pagesAPP3015 Session 6 Presentation - Person-Centred Therapiesjames.hoppeNo ratings yet
- Emotional CrisisDocument12 pagesEmotional CrisisMa Elaine TrinidadNo ratings yet
- Introductory Module:: Stress and Humanitarian WorkDocument104 pagesIntroductory Module:: Stress and Humanitarian WorkThe Vimokkha Online JournalNo ratings yet
- Crisis TheoryDocument26 pagesCrisis TheoryAndraNo ratings yet
- End of Life IssuesDocument35 pagesEnd of Life IssuesJeffrey RamosNo ratings yet
- Trauma 13Document2 pagesTrauma 13DAUPDRAMNo ratings yet
- Module 2 Session 1 Trauma OSAECDocument22 pagesModule 2 Session 1 Trauma OSAECbrian venNo ratings yet
- Psychological First AidDocument60 pagesPsychological First Aidbishakha stylesNo ratings yet
- Death Loss and GriefDocument16 pagesDeath Loss and GriefIshaBrijeshSharmaNo ratings yet
- 98 Unit 11 Stress and HealthDocument32 pages98 Unit 11 Stress and HealthsherrayNo ratings yet
- Grief and LossDocument38 pagesGrief and LossMuarine Faye LaconsNo ratings yet
- Violence, Abuse and NeglectDocument4 pagesViolence, Abuse and NeglectDinarkram Rabreca EculNo ratings yet
- Psychosocial Aspects of Health and DiseaseDocument41 pagesPsychosocial Aspects of Health and Disease70. Iqraa ZamanNo ratings yet
- Session 2Document21 pagesSession 2umibrahimNo ratings yet
- Criticalincidentstress July2017Document4 pagesCriticalincidentstress July2017renato.rdfNo ratings yet
- STEMS IntroductionMaterialandSafetyPlans PDFDocument10 pagesSTEMS IntroductionMaterialandSafetyPlans PDFSera ChunNo ratings yet
- Inculsiveess Chapter - 3?!Document65 pagesInculsiveess Chapter - 3?!Eliyas BeniyamNo ratings yet
- Stress, Conflict and Change Management in EducationDocument13 pagesStress, Conflict and Change Management in EducationHonourable Lloyd ChandaNo ratings yet
- Grief & Grieving ProcessDocument39 pagesGrief & Grieving Processelmerconde100% (4)
- Psychosocial Care and Support in Disaster ManagementDocument14 pagesPsychosocial Care and Support in Disaster ManagementrohitpangreNo ratings yet
- Suicide and Self Harm: DR Nemache Mawere Psychiatrist MBBS IV - Feb 2020Document36 pagesSuicide and Self Harm: DR Nemache Mawere Psychiatrist MBBS IV - Feb 2020AnoobisNo ratings yet
- Passages … Through Grief: Healing Life’s Losses Participant’s ManualFrom EverandPassages … Through Grief: Healing Life’s Losses Participant’s ManualNo ratings yet
- Recordings DatabaseDocument15 pagesRecordings DatabaseChelsi KukretyNo ratings yet
- Pi Nclex Module ReviewDocument192 pagesPi Nclex Module ReviewDan kibet TumboNo ratings yet
- Philosophy - Environment CrisisDocument12 pagesPhilosophy - Environment CrisisMarian Banayo LunaNo ratings yet
- A Comparative Study of Two Global CrisesDocument18 pagesA Comparative Study of Two Global CrisessdfNo ratings yet
- Positive Behavioural Support 4204EDN: Intervention PlanningDocument41 pagesPositive Behavioural Support 4204EDN: Intervention PlanningjacquelineNo ratings yet
- Crisis ManagementDocument16 pagesCrisis Managementnikiniki9100% (1)
- Crisis Management1Document59 pagesCrisis Management1Infrastructure Development ServiceNo ratings yet
- Ebffiledoc - 306download PDF Crisis Intervention A Practical Guide 1St Edition Alan A Cavaiola Ebook Full ChapterDocument53 pagesEbffiledoc - 306download PDF Crisis Intervention A Practical Guide 1St Edition Alan A Cavaiola Ebook Full Chapterpeter.tubb838100% (3)
- Ethiopian Pressure StudyDocument308 pagesEthiopian Pressure StudyAfif Ahmed BellikunhiNo ratings yet
- Final Coaching CASEWORK 1Document290 pagesFinal Coaching CASEWORK 1hayaton408No ratings yet
- Mass Communication Course - Delhi School of Communication PR and Crisis Thesis ReportDocument92 pagesMass Communication Course - Delhi School of Communication PR and Crisis Thesis ReportDelhi School of CommunicationNo ratings yet
- Risk Assessment in The Maritime Industry PDFDocument5 pagesRisk Assessment in The Maritime Industry PDFgksahaNo ratings yet
- Concept Note Locally-Led Response 151215Document7 pagesConcept Note Locally-Led Response 151215lululifeNo ratings yet
- Crisis InterventionDocument14 pagesCrisis InterventionCheasca AbellarNo ratings yet
- Project Report Mobile BankingDocument49 pagesProject Report Mobile Bankingtanugutpta100% (7)
- Lesson 7 FamilyDocument33 pagesLesson 7 FamilyMV FadsNo ratings yet
- The AIESEC Crisis Comms Manual PDFDocument2 pagesThe AIESEC Crisis Comms Manual PDFSharma Gokhool100% (2)
- Social Case Work Practice or Working With Individuals UNIT IIDocument78 pagesSocial Case Work Practice or Working With Individuals UNIT IIJai Santhosh100% (1)
- Effect of US Government Policies On The Financial Markets and The World EconomyDocument179 pagesEffect of US Government Policies On The Financial Markets and The World EconomyAfrican ViewsNo ratings yet
- Growing American Youth CMP FINALDocument43 pagesGrowing American Youth CMP FINALLaur MarchapNo ratings yet
- Agriculture: Agritourism in The Era of The Coronavirus (COVID-19) : A Rapid Assessment From PolandDocument19 pagesAgriculture: Agritourism in The Era of The Coronavirus (COVID-19) : A Rapid Assessment From Polandapril_jingcoNo ratings yet
- MGMT2002 - Notes From Week 7-13 SEM 1 2017Document8 pagesMGMT2002 - Notes From Week 7-13 SEM 1 2017SolNo ratings yet
- Now Is The Time For UnityDocument2 pagesNow Is The Time For UnityBilliemontelfish EilishNo ratings yet
- CP Earthquake April 2023Document29 pagesCP Earthquake April 2023Marlon Villena100% (1)
- Crisis Communication of ToyotaDocument76 pagesCrisis Communication of Toyotajammy9100% (1)
- Family StressDocument36 pagesFamily StressRaymonde Uy100% (1)