
Features of The Course of Cholecystocardial Syndrome
Features of The Course of Cholecystocardial Syndrome
You might also like
- Epidemiology of CVD DiseasesDocument19 pagesEpidemiology of CVD DiseaseshafizahhoshniNo ratings yet
- Comprehensive Insights into Acute Arterial Occlusion: Pathways, Prevention, and Holistic CareFrom EverandComprehensive Insights into Acute Arterial Occlusion: Pathways, Prevention, and Holistic CareNo ratings yet
- Cholesterol Crystal Embolism and Chronic Kidney DiDocument12 pagesCholesterol Crystal Embolism and Chronic Kidney DiKhairunnisa NsNo ratings yet
- Colecistul În Sistemul Biliopancreaticoduodenal (Revista Literaturii)Document4 pagesColecistul În Sistemul Biliopancreaticoduodenal (Revista Literaturii)Ion MașcauțanNo ratings yet
- Pharmacokinetics and PharmacodynamicsDocument166 pagesPharmacokinetics and PharmacodynamicsEvgeny BadmaevNo ratings yet
- Advancements in Acute Aortic Syndrome: From Pathophysiology to Personalized TherapeuticsFrom EverandAdvancements in Acute Aortic Syndrome: From Pathophysiology to Personalized TherapeuticsNo ratings yet
- Analytical Journal of Education and Development: Cardiovascular Diseases in Patients With Diabetes MellitusDocument6 pagesAnalytical Journal of Education and Development: Cardiovascular Diseases in Patients With Diabetes MellitusSunny JNo ratings yet
- Cardiac Involvement in Systemic SclerosisDocument7 pagesCardiac Involvement in Systemic SclerosisWisnu MataramNo ratings yet
- JCM 10 03239Document42 pagesJCM 10 03239Pamela MusabelliuNo ratings yet
- Definitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis - Tokyo GuidelinesDocument13 pagesDefinitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis - Tokyo GuidelinesNilamsari KurniasihNo ratings yet
- Embolism From Atherosclerotic Plaque - Atheroembolism (Cholesterol Crystal Embolism) - UpToDateDocument39 pagesEmbolism From Atherosclerotic Plaque - Atheroembolism (Cholesterol Crystal Embolism) - UpToDateDiego RodriguesNo ratings yet
- Acute CholangitisDocument12 pagesAcute CholangitisWira LinNo ratings yet
- Features of The Aggregate State of Blood in Patients With Ischemic Heart Disease Combined With Type 2 Diabetes MellitusDocument6 pagesFeatures of The Aggregate State of Blood in Patients With Ischemic Heart Disease Combined With Type 2 Diabetes MellitusCentral Asian StudiesNo ratings yet
- DocxDocument3 pagesDocxCamille Joy BaliliNo ratings yet
- Swapnil Thesis PaperDocument5 pagesSwapnil Thesis PaperSwapnil SahuNo ratings yet
- ACP Case Study (2) - 1Document24 pagesACP Case Study (2) - 1Hawwa SaifaNo ratings yet
- Pathogenesis of Ischemic Heart Disease: Diploma ThesisDocument24 pagesPathogenesis of Ischemic Heart Disease: Diploma ThesisEcaterina GorganNo ratings yet
- Prevention Measures of Chronic Renal Failure in AdultsDocument3 pagesPrevention Measures of Chronic Renal Failure in AdultsCentral Asian StudiesNo ratings yet
- Renal and Extra-Renal Diseases, Their Etiological and Epidemiological ManifestationsDocument5 pagesRenal and Extra-Renal Diseases, Their Etiological and Epidemiological ManifestationsCentral Asian StudiesNo ratings yet
- Jurnal Penyakit Jantung Koroner: Nama: Besse Saika Nirmalasari KLS: W8 STB: 1412090440Document15 pagesJurnal Penyakit Jantung Koroner: Nama: Besse Saika Nirmalasari KLS: W8 STB: 1412090440Wardiansyah NaimNo ratings yet
- Hiatalherniaasarare 2Document8 pagesHiatalherniaasarare 2Fernando Nagore AnconaNo ratings yet
- Definitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis Tokyo GuidelinesDocument12 pagesDefinitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis Tokyo GuidelinesGuillermo AranedaNo ratings yet
- Coronary Artery Disease: Assistant of Asian International University ORCID ID 0000-0003-4613-0057Document7 pagesCoronary Artery Disease: Assistant of Asian International University ORCID ID 0000-0003-4613-0057Putri WibowoNo ratings yet
- PIIS246802492301536XDocument13 pagesPIIS246802492301536XjosedegibesNo ratings yet
- Budd-Chiary Sindrom AlinDocument10 pagesBudd-Chiary Sindrom AlinLidya Azka FazaNo ratings yet
- Raynauds Disease.1Document14 pagesRaynauds Disease.1Pierre LaPaditeNo ratings yet
- Age-Related Anatomic & Physiological Changes: Cardiovascular SystemDocument4 pagesAge-Related Anatomic & Physiological Changes: Cardiovascular SystemAnonymous AHJFTkI3S5No ratings yet
- 19-22 Aortoenteric Fistula A Possible Cause of Sudden DeathDocument4 pages19-22 Aortoenteric Fistula A Possible Cause of Sudden DeathLoredana MorosanuNo ratings yet
- Choque Septico en CirrosisDocument19 pagesChoque Septico en CirrosisAzael HaggardNo ratings yet
- Peter Martin A. Quiazon Zoology NewspaperDocument2 pagesPeter Martin A. Quiazon Zoology NewspaperBlack Science ManNo ratings yet
- Congestive Hepatopathy: Molecular SciencesDocument23 pagesCongestive Hepatopathy: Molecular SciencesRizky ValriansyahNo ratings yet
- Piis0002962918302209 1 PDFDocument8 pagesPiis0002962918302209 1 PDFNadiarosmaliaNo ratings yet
- Spondilita Ankilozanta Cardio PulmonarDocument6 pagesSpondilita Ankilozanta Cardio PulmonarGiulia LungulescuNo ratings yet
- Stomach and DuodenumDocument84 pagesStomach and DuodenumDhanush PillaiNo ratings yet
- Beyond the Aorta: Exploring the Depths of Abdominal Aortic AneurysmFrom EverandBeyond the Aorta: Exploring the Depths of Abdominal Aortic AneurysmNo ratings yet
- Aging of Cardiovascular System PDFDocument16 pagesAging of Cardiovascular System PDFpitkerenNo ratings yet
- Study On The Contribution of Physical Balnear Therapy On Patients With Pathology Confounding Cerebrovascular and Degenerative RheumaticDocument21 pagesStudy On The Contribution of Physical Balnear Therapy On Patients With Pathology Confounding Cerebrovascular and Degenerative RheumaticElena PopescuNo ratings yet
- Coronary Heart Disease - Pari VermaDocument4 pagesCoronary Heart Disease - Pari Vermaverma.pari1610No ratings yet
- Evaluation of Adults With Ascites - UpToDateDocument25 pagesEvaluation of Adults With Ascites - UpToDateWynnie VoonNo ratings yet
- Benefits of Biotics For Cardiovascular DiseasesDocument18 pagesBenefits of Biotics For Cardiovascular DiseasesDyane VatriciaNo ratings yet
- Ischemic Heart Disease Pathophysiology Paradigms Overview: From Plaque Activation To Microvascular DysfunctionDocument30 pagesIschemic Heart Disease Pathophysiology Paradigms Overview: From Plaque Activation To Microvascular DysfunctionFannyNo ratings yet
- 2021 New Approaches To Management of Pericardial EffusionsDocument9 pages2021 New Approaches To Management of Pericardial Effusionsjlmatos08No ratings yet
- Thromboembolic Complications in Chronic Inflammatory Bowel DiseaseDocument6 pagesThromboembolic Complications in Chronic Inflammatory Bowel DiseaseIJAR JOURNALNo ratings yet
- Approach To Cardiac PatientDocument6 pagesApproach To Cardiac PatientDemuel Dee L. BertoNo ratings yet
- Heart Kidney InteractionDocument11 pagesHeart Kidney InteractionMichael HostiadiNo ratings yet
- Cirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDocument21 pagesCirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDan ChicinasNo ratings yet
- Circulatory System's Diseases in The ElderlyDocument5 pagesCirculatory System's Diseases in The ElderlySabrina JonesNo ratings yet
- Ascitis ImportanteDocument17 pagesAscitis Importantedanyescalerapumas24No ratings yet
- Acute Myocardial InfarctionDocument17 pagesAcute Myocardial InfarctionRuqowiyah TanjungNo ratings yet
- Corrected QT Interval in Systemic Sclerosis Patients: Archives of Rheumatology & Arthritis ResearchDocument4 pagesCorrected QT Interval in Systemic Sclerosis Patients: Archives of Rheumatology & Arthritis ResearchAlexandruFlaviaNo ratings yet
- Article in Press Page 1 Full Text First ArticleDocument15 pagesArticle in Press Page 1 Full Text First Articlenavyakasturi92No ratings yet
- Acute Cholecystitis From Biliary LithiasisDocument17 pagesAcute Cholecystitis From Biliary Lithiasisdhimas satriaNo ratings yet
- Views On "Postcholecystectomy Syndrome"Document7 pagesViews On "Postcholecystectomy Syndrome"Central Asian StudiesNo ratings yet
- Hipertensi 2Document23 pagesHipertensi 2ayunimrsNo ratings yet
- 27264Document19 pages27264eenNo ratings yet
- Preprints202307 1050 v1Document12 pagesPreprints202307 1050 v1Mihai PopescuNo ratings yet
- Biology Internal AssessmentDocument16 pagesBiology Internal Assessmenthello helloNo ratings yet
- BR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationDocument16 pagesBR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationSergio Alberto Sulub NavarreteNo ratings yet
- Chapter 2 YUMDocument8 pagesChapter 2 YUMGlenelyn Grace InfanteNo ratings yet
- Review of Standard and Advanced Surgical Treatments For Invasive Bladder CancerDocument11 pagesReview of Standard and Advanced Surgical Treatments For Invasive Bladder CancerCentral Asian StudiesNo ratings yet
- Morphological Changes in The Adrenal Glands in Rheumatoid ArthritisDocument6 pagesMorphological Changes in The Adrenal Glands in Rheumatoid ArthritisCentral Asian StudiesNo ratings yet
- A Comprehensive Approach To The Treatment of Facial Neuropathy in ChildrenDocument6 pagesA Comprehensive Approach To The Treatment of Facial Neuropathy in ChildrenCentral Asian StudiesNo ratings yet
- Immunological Effectiveness of Immuno - and Biocorrective Treatment of Dental Diseases in Pregnant WomenDocument4 pagesImmunological Effectiveness of Immuno - and Biocorrective Treatment of Dental Diseases in Pregnant WomenCentral Asian StudiesNo ratings yet
- Effectiveness of The Drug L-Montus (Montelukast) in The Treatment of Bronchial AsthmaDocument4 pagesEffectiveness of The Drug L-Montus (Montelukast) in The Treatment of Bronchial AsthmaCentral Asian StudiesNo ratings yet
- Risk Factors For Arterial Hypertension in Young AgesDocument6 pagesRisk Factors For Arterial Hypertension in Young AgesCentral Asian StudiesNo ratings yet
- The Role of Endothelial Dysfunction Genes in The Development of Postpartum HemorrhageDocument6 pagesThe Role of Endothelial Dysfunction Genes in The Development of Postpartum HemorrhageCentral Asian StudiesNo ratings yet
- Prevention of Dental DiseasesDocument4 pagesPrevention of Dental DiseasesCentral Asian StudiesNo ratings yet
- Evaluation The Role of Hepcidin in Lymphoma PatientsDocument11 pagesEvaluation The Role of Hepcidin in Lymphoma PatientsCentral Asian StudiesNo ratings yet
- Volume: 05 Issue: 01 - Jan-Feb 2024Document7 pagesVolume: 05 Issue: 01 - Jan-Feb 2024Central Asian StudiesNo ratings yet
- The Importance of Magnetic Resonance Imaging in The Diagnosis and Treatment of Diabetic Foot SyndromeDocument7 pagesThe Importance of Magnetic Resonance Imaging in The Diagnosis and Treatment of Diabetic Foot SyndromeCentral Asian StudiesNo ratings yet
- Spectroscopy, Thermal Analysis, Bioavailability and Anticancer Activity of Copper (Ii) Complex With Heterocyclic Azo Dye LigandDocument13 pagesSpectroscopy, Thermal Analysis, Bioavailability and Anticancer Activity of Copper (Ii) Complex With Heterocyclic Azo Dye LigandCentral Asian StudiesNo ratings yet
- Volume: 05 Issue: 01 - Jan-Feb 2024Document8 pagesVolume: 05 Issue: 01 - Jan-Feb 2024Central Asian StudiesNo ratings yet
- Effect of The Concept Mapping Strategy On Teaching and Retaining Some Basic Football Skills To Fifth-Grade Middle School StudentsDocument10 pagesEffect of The Concept Mapping Strategy On Teaching and Retaining Some Basic Football Skills To Fifth-Grade Middle School StudentsCentral Asian StudiesNo ratings yet
- Volume: 05 Issue: 01 - Jan-Feb 2024Document4 pagesVolume: 05 Issue: 01 - Jan-Feb 2024Central Asian StudiesNo ratings yet
- Volume: 05 Issue: 01 - Jan-Feb 2024: Central Asian Journal of Medical and Natural SciencesDocument14 pagesVolume: 05 Issue: 01 - Jan-Feb 2024: Central Asian Journal of Medical and Natural SciencesCentral Asian StudiesNo ratings yet
- Comparative Evaluation of The Effectiveness of Ultrasound and X-Ray Imaging in The Diagnosis of Hip Dysplasia in Children Under 6 Months of AgeDocument8 pagesComparative Evaluation of The Effectiveness of Ultrasound and X-Ray Imaging in The Diagnosis of Hip Dysplasia in Children Under 6 Months of AgeCentral Asian StudiesNo ratings yet
- Analysis of Somatic and Reproductive History of Women With Inflammatory Diseases of The Pelvic Organs Due To Hiv InfectionDocument9 pagesAnalysis of Somatic and Reproductive History of Women With Inflammatory Diseases of The Pelvic Organs Due To Hiv InfectionCentral Asian StudiesNo ratings yet
- Volume: 04 Issue: 06 - Nov-Dec 2023Document6 pagesVolume: 04 Issue: 06 - Nov-Dec 2023Central Asian StudiesNo ratings yet
- Assessing The Efficiency of Ultrasound For Diagnosing Developmental Dysplasia of The Hip (DDH) in Infants Below 6 MonthsDocument8 pagesAssessing The Efficiency of Ultrasound For Diagnosing Developmental Dysplasia of The Hip (DDH) in Infants Below 6 MonthsCentral Asian StudiesNo ratings yet
- Effectiveness of Instruction Program in Improving Balance Level Among Seniors With OsteoporosisDocument8 pagesEffectiveness of Instruction Program in Improving Balance Level Among Seniors With OsteoporosisCentral Asian StudiesNo ratings yet
- Changes in SEP Indicators in Patients Using RPMS in Muscle Hypotonia SyndromeDocument4 pagesChanges in SEP Indicators in Patients Using RPMS in Muscle Hypotonia SyndromeCentral Asian StudiesNo ratings yet
- Pregnancy and Undifferentiated Connective Tissue DysplasiaDocument5 pagesPregnancy and Undifferentiated Connective Tissue DysplasiaCentral Asian StudiesNo ratings yet
- Cortical Fixing Screws Are The Method of Choice For Conservative Treatment of Mandibular FracturesDocument13 pagesCortical Fixing Screws Are The Method of Choice For Conservative Treatment of Mandibular FracturesCentral Asian StudiesNo ratings yet
- Vitamin D Deficiency For Patients With Depression (Case Control Study)Document15 pagesVitamin D Deficiency For Patients With Depression (Case Control Study)Central Asian StudiesNo ratings yet
- Structural and Functional Changes in Periodontal Tissues During Prosthetics With Metal-Ceramic and Zirconium DenturesDocument11 pagesStructural and Functional Changes in Periodontal Tissues During Prosthetics With Metal-Ceramic and Zirconium DenturesCentral Asian StudiesNo ratings yet
- The Importance of Microelements in The Development of Chronic Kidney DiseaseDocument3 pagesThe Importance of Microelements in The Development of Chronic Kidney DiseaseCentral Asian StudiesNo ratings yet
- Needs For Resort and Health Care and Innovative Approaches To Its MeetingDocument6 pagesNeeds For Resort and Health Care and Innovative Approaches To Its MeetingCentral Asian StudiesNo ratings yet
- Iraqibacter As A New Emerging PathogenDocument6 pagesIraqibacter As A New Emerging PathogenCentral Asian StudiesNo ratings yet
- Hygienic Assessment of The Impact of Harmful Substances Formed During The Production of Mineral Fertiliser On The Immune Health Status of ChildrenDocument6 pagesHygienic Assessment of The Impact of Harmful Substances Formed During The Production of Mineral Fertiliser On The Immune Health Status of ChildrenCentral Asian StudiesNo ratings yet
- Los Angeles Police OrganizationDocument9 pagesLos Angeles Police OrganizationRylie MatienzoNo ratings yet
- Metode PengujianDocument17 pagesMetode Pengujianabraham samadNo ratings yet
- CSRDocument16 pagesCSRAnkit YadavNo ratings yet
- Astm D 4258Document2 pagesAstm D 4258anthonybarnard100% (1)
- FSC International StandardDocument15 pagesFSC International StandardEMINANo ratings yet
- Mochamad Juwildia Prayoga - Motivation Letter MAECIDocument2 pagesMochamad Juwildia Prayoga - Motivation Letter MAECIMochamad JuwildiaNo ratings yet
- Catalog Telecommunication Cable PDFDocument29 pagesCatalog Telecommunication Cable PDFVictor AxelsonNo ratings yet
- Currency Detection For Blind PeopleDocument19 pagesCurrency Detection For Blind Peoplehaffah1245No ratings yet
- Maintenance of PSC GirdersDocument10 pagesMaintenance of PSC GirdersradhakrishnangNo ratings yet
- Action Research ModelDocument5 pagesAction Research ModelGapuz, Michelle C.No ratings yet
- Physics Part 2 Class Xii PDF FreeDocument263 pagesPhysics Part 2 Class Xii PDF FreeibbuarmNo ratings yet
- Which of The Following Is An External Sorting?: Merge Sort Tree Sort Bubble Sort Insertion SortDocument3 pagesWhich of The Following Is An External Sorting?: Merge Sort Tree Sort Bubble Sort Insertion SortAjay BhoopalNo ratings yet
- ChalukyanDocument44 pagesChalukyannimisha jainNo ratings yet
- Caterpillar D6Document3 pagesCaterpillar D6RasoolKhadibi100% (1)
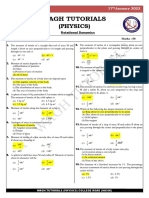
- Mock Test - 98 (17 Jan 2023) Rotational DynamicsDocument1 pageMock Test - 98 (17 Jan 2023) Rotational DynamicsparamNo ratings yet
- Horizon Aviation Academy - HellasDocument2 pagesHorizon Aviation Academy - Hellas1n4r51ssNo ratings yet
- AK Khan Telecom Limited: Orientation ScheduleDocument2 pagesAK Khan Telecom Limited: Orientation Schedulemozammel80No ratings yet
- Aplicacion Corto 3Document5 pagesAplicacion Corto 3Garbel LemusNo ratings yet
- About JK TyreDocument10 pagesAbout JK TyreAshish Adholiya0% (1)
- Resume Goutam AdwantDocument3 pagesResume Goutam AdwantGoutamNo ratings yet
- CH 2 - Guide To Physics PracticalsDocument20 pagesCH 2 - Guide To Physics PracticalsNong Hm100% (2)
- TDS - Emaco R907 PlusDocument2 pagesTDS - Emaco R907 PlusVenkata RaoNo ratings yet
- Project Final Report TemplateDocument14 pagesProject Final Report Templatemonparaashvin0% (1)
- NCERT Solutions For Class 12 Physics Chapter 3 Current ElectricityDocument24 pagesNCERT Solutions For Class 12 Physics Chapter 3 Current ElectricityDileep GNo ratings yet
- Semantic Segmentation Data Labelling: Classes and InstructionsDocument9 pagesSemantic Segmentation Data Labelling: Classes and InstructionsMar FieldsNo ratings yet
- General Biology 1: TEST II. Modified True or False. Indicate Whether The Statement Is True or False. If False, Change TheDocument2 pagesGeneral Biology 1: TEST II. Modified True or False. Indicate Whether The Statement Is True or False. If False, Change TheMA. HAZEL TEOLOGONo ratings yet
- 6yc Multifunction Meter: Operation ManualDocument46 pages6yc Multifunction Meter: Operation ManualHamish JosephNo ratings yet
- Ae tt8 Progress Test 3Document7 pagesAe tt8 Progress Test 3Joana Silva100% (1)
- Solutions To Mathematical Statistics With Applications, Pg. 409, Ex. 39Document5 pagesSolutions To Mathematical Statistics With Applications, Pg. 409, Ex. 39Ivi DownhamNo ratings yet
- Understanding Computer InvestigationsDocument64 pagesUnderstanding Computer InvestigationsLillian KobusingyeNo ratings yet























































































































Download as pdf or txt
You might also like
- Epidemiology of CVD DiseasesDocument19 pagesEpidemiology of CVD DiseaseshafizahhoshniNo ratings yet
- Comprehensive Insights into Acute Arterial Occlusion: Pathways, Prevention, and Holistic CareFrom EverandComprehensive Insights into Acute Arterial Occlusion: Pathways, Prevention, and Holistic CareNo ratings yet
- Cholesterol Crystal Embolism and Chronic Kidney DiDocument12 pagesCholesterol Crystal Embolism and Chronic Kidney DiKhairunnisa NsNo ratings yet
- Colecistul În Sistemul Biliopancreaticoduodenal (Revista Literaturii)Document4 pagesColecistul În Sistemul Biliopancreaticoduodenal (Revista Literaturii)Ion MașcauțanNo ratings yet
- Pharmacokinetics and PharmacodynamicsDocument166 pagesPharmacokinetics and PharmacodynamicsEvgeny BadmaevNo ratings yet
- Advancements in Acute Aortic Syndrome: From Pathophysiology to Personalized TherapeuticsFrom EverandAdvancements in Acute Aortic Syndrome: From Pathophysiology to Personalized TherapeuticsNo ratings yet
- Analytical Journal of Education and Development: Cardiovascular Diseases in Patients With Diabetes MellitusDocument6 pagesAnalytical Journal of Education and Development: Cardiovascular Diseases in Patients With Diabetes MellitusSunny JNo ratings yet
- Cardiac Involvement in Systemic SclerosisDocument7 pagesCardiac Involvement in Systemic SclerosisWisnu MataramNo ratings yet
- JCM 10 03239Document42 pagesJCM 10 03239Pamela MusabelliuNo ratings yet
- Definitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis - Tokyo GuidelinesDocument13 pagesDefinitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis - Tokyo GuidelinesNilamsari KurniasihNo ratings yet
- Embolism From Atherosclerotic Plaque - Atheroembolism (Cholesterol Crystal Embolism) - UpToDateDocument39 pagesEmbolism From Atherosclerotic Plaque - Atheroembolism (Cholesterol Crystal Embolism) - UpToDateDiego RodriguesNo ratings yet
- Acute CholangitisDocument12 pagesAcute CholangitisWira LinNo ratings yet
- Features of The Aggregate State of Blood in Patients With Ischemic Heart Disease Combined With Type 2 Diabetes MellitusDocument6 pagesFeatures of The Aggregate State of Blood in Patients With Ischemic Heart Disease Combined With Type 2 Diabetes MellitusCentral Asian StudiesNo ratings yet
- DocxDocument3 pagesDocxCamille Joy BaliliNo ratings yet
- Swapnil Thesis PaperDocument5 pagesSwapnil Thesis PaperSwapnil SahuNo ratings yet
- ACP Case Study (2) - 1Document24 pagesACP Case Study (2) - 1Hawwa SaifaNo ratings yet
- Pathogenesis of Ischemic Heart Disease: Diploma ThesisDocument24 pagesPathogenesis of Ischemic Heart Disease: Diploma ThesisEcaterina GorganNo ratings yet
- Prevention Measures of Chronic Renal Failure in AdultsDocument3 pagesPrevention Measures of Chronic Renal Failure in AdultsCentral Asian StudiesNo ratings yet
- Renal and Extra-Renal Diseases, Their Etiological and Epidemiological ManifestationsDocument5 pagesRenal and Extra-Renal Diseases, Their Etiological and Epidemiological ManifestationsCentral Asian StudiesNo ratings yet
- Jurnal Penyakit Jantung Koroner: Nama: Besse Saika Nirmalasari KLS: W8 STB: 1412090440Document15 pagesJurnal Penyakit Jantung Koroner: Nama: Besse Saika Nirmalasari KLS: W8 STB: 1412090440Wardiansyah NaimNo ratings yet
- Hiatalherniaasarare 2Document8 pagesHiatalherniaasarare 2Fernando Nagore AnconaNo ratings yet
- Definitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis Tokyo GuidelinesDocument12 pagesDefinitions, Pathophysiology, and Epidemiology of Acute Cholangitis and Cholecystitis Tokyo GuidelinesGuillermo AranedaNo ratings yet
- Coronary Artery Disease: Assistant of Asian International University ORCID ID 0000-0003-4613-0057Document7 pagesCoronary Artery Disease: Assistant of Asian International University ORCID ID 0000-0003-4613-0057Putri WibowoNo ratings yet
- PIIS246802492301536XDocument13 pagesPIIS246802492301536XjosedegibesNo ratings yet
- Budd-Chiary Sindrom AlinDocument10 pagesBudd-Chiary Sindrom AlinLidya Azka FazaNo ratings yet
- Raynauds Disease.1Document14 pagesRaynauds Disease.1Pierre LaPaditeNo ratings yet
- Age-Related Anatomic & Physiological Changes: Cardiovascular SystemDocument4 pagesAge-Related Anatomic & Physiological Changes: Cardiovascular SystemAnonymous AHJFTkI3S5No ratings yet
- 19-22 Aortoenteric Fistula A Possible Cause of Sudden DeathDocument4 pages19-22 Aortoenteric Fistula A Possible Cause of Sudden DeathLoredana MorosanuNo ratings yet
- Choque Septico en CirrosisDocument19 pagesChoque Septico en CirrosisAzael HaggardNo ratings yet
- Peter Martin A. Quiazon Zoology NewspaperDocument2 pagesPeter Martin A. Quiazon Zoology NewspaperBlack Science ManNo ratings yet
- Congestive Hepatopathy: Molecular SciencesDocument23 pagesCongestive Hepatopathy: Molecular SciencesRizky ValriansyahNo ratings yet
- Piis0002962918302209 1 PDFDocument8 pagesPiis0002962918302209 1 PDFNadiarosmaliaNo ratings yet
- Spondilita Ankilozanta Cardio PulmonarDocument6 pagesSpondilita Ankilozanta Cardio PulmonarGiulia LungulescuNo ratings yet
- Stomach and DuodenumDocument84 pagesStomach and DuodenumDhanush PillaiNo ratings yet
- Beyond the Aorta: Exploring the Depths of Abdominal Aortic AneurysmFrom EverandBeyond the Aorta: Exploring the Depths of Abdominal Aortic AneurysmNo ratings yet
- Aging of Cardiovascular System PDFDocument16 pagesAging of Cardiovascular System PDFpitkerenNo ratings yet
- Study On The Contribution of Physical Balnear Therapy On Patients With Pathology Confounding Cerebrovascular and Degenerative RheumaticDocument21 pagesStudy On The Contribution of Physical Balnear Therapy On Patients With Pathology Confounding Cerebrovascular and Degenerative RheumaticElena PopescuNo ratings yet
- Coronary Heart Disease - Pari VermaDocument4 pagesCoronary Heart Disease - Pari Vermaverma.pari1610No ratings yet
- Evaluation of Adults With Ascites - UpToDateDocument25 pagesEvaluation of Adults With Ascites - UpToDateWynnie VoonNo ratings yet
- Benefits of Biotics For Cardiovascular DiseasesDocument18 pagesBenefits of Biotics For Cardiovascular DiseasesDyane VatriciaNo ratings yet
- Ischemic Heart Disease Pathophysiology Paradigms Overview: From Plaque Activation To Microvascular DysfunctionDocument30 pagesIschemic Heart Disease Pathophysiology Paradigms Overview: From Plaque Activation To Microvascular DysfunctionFannyNo ratings yet
- 2021 New Approaches To Management of Pericardial EffusionsDocument9 pages2021 New Approaches To Management of Pericardial Effusionsjlmatos08No ratings yet
- Thromboembolic Complications in Chronic Inflammatory Bowel DiseaseDocument6 pagesThromboembolic Complications in Chronic Inflammatory Bowel DiseaseIJAR JOURNALNo ratings yet
- Approach To Cardiac PatientDocument6 pagesApproach To Cardiac PatientDemuel Dee L. BertoNo ratings yet
- Heart Kidney InteractionDocument11 pagesHeart Kidney InteractionMichael HostiadiNo ratings yet
- Cirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDocument21 pagesCirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDan ChicinasNo ratings yet
- Circulatory System's Diseases in The ElderlyDocument5 pagesCirculatory System's Diseases in The ElderlySabrina JonesNo ratings yet
- Ascitis ImportanteDocument17 pagesAscitis Importantedanyescalerapumas24No ratings yet
- Acute Myocardial InfarctionDocument17 pagesAcute Myocardial InfarctionRuqowiyah TanjungNo ratings yet
- Corrected QT Interval in Systemic Sclerosis Patients: Archives of Rheumatology & Arthritis ResearchDocument4 pagesCorrected QT Interval in Systemic Sclerosis Patients: Archives of Rheumatology & Arthritis ResearchAlexandruFlaviaNo ratings yet
- Article in Press Page 1 Full Text First ArticleDocument15 pagesArticle in Press Page 1 Full Text First Articlenavyakasturi92No ratings yet
- Acute Cholecystitis From Biliary LithiasisDocument17 pagesAcute Cholecystitis From Biliary Lithiasisdhimas satriaNo ratings yet
- Views On "Postcholecystectomy Syndrome"Document7 pagesViews On "Postcholecystectomy Syndrome"Central Asian StudiesNo ratings yet
- Hipertensi 2Document23 pagesHipertensi 2ayunimrsNo ratings yet
- 27264Document19 pages27264eenNo ratings yet
- Preprints202307 1050 v1Document12 pagesPreprints202307 1050 v1Mihai PopescuNo ratings yet
- Biology Internal AssessmentDocument16 pagesBiology Internal Assessmenthello helloNo ratings yet
- BR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationDocument16 pagesBR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationSergio Alberto Sulub NavarreteNo ratings yet
- Chapter 2 YUMDocument8 pagesChapter 2 YUMGlenelyn Grace InfanteNo ratings yet
- Review of Standard and Advanced Surgical Treatments For Invasive Bladder CancerDocument11 pagesReview of Standard and Advanced Surgical Treatments For Invasive Bladder CancerCentral Asian StudiesNo ratings yet
- Morphological Changes in The Adrenal Glands in Rheumatoid ArthritisDocument6 pagesMorphological Changes in The Adrenal Glands in Rheumatoid ArthritisCentral Asian StudiesNo ratings yet
- A Comprehensive Approach To The Treatment of Facial Neuropathy in ChildrenDocument6 pagesA Comprehensive Approach To The Treatment of Facial Neuropathy in ChildrenCentral Asian StudiesNo ratings yet
- Immunological Effectiveness of Immuno - and Biocorrective Treatment of Dental Diseases in Pregnant WomenDocument4 pagesImmunological Effectiveness of Immuno - and Biocorrective Treatment of Dental Diseases in Pregnant WomenCentral Asian StudiesNo ratings yet
- Effectiveness of The Drug L-Montus (Montelukast) in The Treatment of Bronchial AsthmaDocument4 pagesEffectiveness of The Drug L-Montus (Montelukast) in The Treatment of Bronchial AsthmaCentral Asian StudiesNo ratings yet
- Risk Factors For Arterial Hypertension in Young AgesDocument6 pagesRisk Factors For Arterial Hypertension in Young AgesCentral Asian StudiesNo ratings yet
- The Role of Endothelial Dysfunction Genes in The Development of Postpartum HemorrhageDocument6 pagesThe Role of Endothelial Dysfunction Genes in The Development of Postpartum HemorrhageCentral Asian StudiesNo ratings yet
- Prevention of Dental DiseasesDocument4 pagesPrevention of Dental DiseasesCentral Asian StudiesNo ratings yet
- Evaluation The Role of Hepcidin in Lymphoma PatientsDocument11 pagesEvaluation The Role of Hepcidin in Lymphoma PatientsCentral Asian StudiesNo ratings yet
- Volume: 05 Issue: 01 - Jan-Feb 2024Document7 pagesVolume: 05 Issue: 01 - Jan-Feb 2024Central Asian StudiesNo ratings yet
- The Importance of Magnetic Resonance Imaging in The Diagnosis and Treatment of Diabetic Foot SyndromeDocument7 pagesThe Importance of Magnetic Resonance Imaging in The Diagnosis and Treatment of Diabetic Foot SyndromeCentral Asian StudiesNo ratings yet
- Spectroscopy, Thermal Analysis, Bioavailability and Anticancer Activity of Copper (Ii) Complex With Heterocyclic Azo Dye LigandDocument13 pagesSpectroscopy, Thermal Analysis, Bioavailability and Anticancer Activity of Copper (Ii) Complex With Heterocyclic Azo Dye LigandCentral Asian StudiesNo ratings yet
- Volume: 05 Issue: 01 - Jan-Feb 2024Document8 pagesVolume: 05 Issue: 01 - Jan-Feb 2024Central Asian StudiesNo ratings yet
- Effect of The Concept Mapping Strategy On Teaching and Retaining Some Basic Football Skills To Fifth-Grade Middle School StudentsDocument10 pagesEffect of The Concept Mapping Strategy On Teaching and Retaining Some Basic Football Skills To Fifth-Grade Middle School StudentsCentral Asian StudiesNo ratings yet
- Volume: 05 Issue: 01 - Jan-Feb 2024Document4 pagesVolume: 05 Issue: 01 - Jan-Feb 2024Central Asian StudiesNo ratings yet
- Volume: 05 Issue: 01 - Jan-Feb 2024: Central Asian Journal of Medical and Natural SciencesDocument14 pagesVolume: 05 Issue: 01 - Jan-Feb 2024: Central Asian Journal of Medical and Natural SciencesCentral Asian StudiesNo ratings yet
- Comparative Evaluation of The Effectiveness of Ultrasound and X-Ray Imaging in The Diagnosis of Hip Dysplasia in Children Under 6 Months of AgeDocument8 pagesComparative Evaluation of The Effectiveness of Ultrasound and X-Ray Imaging in The Diagnosis of Hip Dysplasia in Children Under 6 Months of AgeCentral Asian StudiesNo ratings yet
- Analysis of Somatic and Reproductive History of Women With Inflammatory Diseases of The Pelvic Organs Due To Hiv InfectionDocument9 pagesAnalysis of Somatic and Reproductive History of Women With Inflammatory Diseases of The Pelvic Organs Due To Hiv InfectionCentral Asian StudiesNo ratings yet
- Volume: 04 Issue: 06 - Nov-Dec 2023Document6 pagesVolume: 04 Issue: 06 - Nov-Dec 2023Central Asian StudiesNo ratings yet
- Assessing The Efficiency of Ultrasound For Diagnosing Developmental Dysplasia of The Hip (DDH) in Infants Below 6 MonthsDocument8 pagesAssessing The Efficiency of Ultrasound For Diagnosing Developmental Dysplasia of The Hip (DDH) in Infants Below 6 MonthsCentral Asian StudiesNo ratings yet
- Effectiveness of Instruction Program in Improving Balance Level Among Seniors With OsteoporosisDocument8 pagesEffectiveness of Instruction Program in Improving Balance Level Among Seniors With OsteoporosisCentral Asian StudiesNo ratings yet
- Changes in SEP Indicators in Patients Using RPMS in Muscle Hypotonia SyndromeDocument4 pagesChanges in SEP Indicators in Patients Using RPMS in Muscle Hypotonia SyndromeCentral Asian StudiesNo ratings yet
- Pregnancy and Undifferentiated Connective Tissue DysplasiaDocument5 pagesPregnancy and Undifferentiated Connective Tissue DysplasiaCentral Asian StudiesNo ratings yet
- Cortical Fixing Screws Are The Method of Choice For Conservative Treatment of Mandibular FracturesDocument13 pagesCortical Fixing Screws Are The Method of Choice For Conservative Treatment of Mandibular FracturesCentral Asian StudiesNo ratings yet
- Vitamin D Deficiency For Patients With Depression (Case Control Study)Document15 pagesVitamin D Deficiency For Patients With Depression (Case Control Study)Central Asian StudiesNo ratings yet
- Structural and Functional Changes in Periodontal Tissues During Prosthetics With Metal-Ceramic and Zirconium DenturesDocument11 pagesStructural and Functional Changes in Periodontal Tissues During Prosthetics With Metal-Ceramic and Zirconium DenturesCentral Asian StudiesNo ratings yet
- The Importance of Microelements in The Development of Chronic Kidney DiseaseDocument3 pagesThe Importance of Microelements in The Development of Chronic Kidney DiseaseCentral Asian StudiesNo ratings yet
- Needs For Resort and Health Care and Innovative Approaches To Its MeetingDocument6 pagesNeeds For Resort and Health Care and Innovative Approaches To Its MeetingCentral Asian StudiesNo ratings yet
- Iraqibacter As A New Emerging PathogenDocument6 pagesIraqibacter As A New Emerging PathogenCentral Asian StudiesNo ratings yet
- Hygienic Assessment of The Impact of Harmful Substances Formed During The Production of Mineral Fertiliser On The Immune Health Status of ChildrenDocument6 pagesHygienic Assessment of The Impact of Harmful Substances Formed During The Production of Mineral Fertiliser On The Immune Health Status of ChildrenCentral Asian StudiesNo ratings yet
- Los Angeles Police OrganizationDocument9 pagesLos Angeles Police OrganizationRylie MatienzoNo ratings yet
- Metode PengujianDocument17 pagesMetode Pengujianabraham samadNo ratings yet
- CSRDocument16 pagesCSRAnkit YadavNo ratings yet
- Astm D 4258Document2 pagesAstm D 4258anthonybarnard100% (1)
- FSC International StandardDocument15 pagesFSC International StandardEMINANo ratings yet
- Mochamad Juwildia Prayoga - Motivation Letter MAECIDocument2 pagesMochamad Juwildia Prayoga - Motivation Letter MAECIMochamad JuwildiaNo ratings yet
- Catalog Telecommunication Cable PDFDocument29 pagesCatalog Telecommunication Cable PDFVictor AxelsonNo ratings yet
- Currency Detection For Blind PeopleDocument19 pagesCurrency Detection For Blind Peoplehaffah1245No ratings yet
- Maintenance of PSC GirdersDocument10 pagesMaintenance of PSC GirdersradhakrishnangNo ratings yet
- Action Research ModelDocument5 pagesAction Research ModelGapuz, Michelle C.No ratings yet
- Physics Part 2 Class Xii PDF FreeDocument263 pagesPhysics Part 2 Class Xii PDF FreeibbuarmNo ratings yet
- Which of The Following Is An External Sorting?: Merge Sort Tree Sort Bubble Sort Insertion SortDocument3 pagesWhich of The Following Is An External Sorting?: Merge Sort Tree Sort Bubble Sort Insertion SortAjay BhoopalNo ratings yet
- ChalukyanDocument44 pagesChalukyannimisha jainNo ratings yet
- Caterpillar D6Document3 pagesCaterpillar D6RasoolKhadibi100% (1)
- Mock Test - 98 (17 Jan 2023) Rotational DynamicsDocument1 pageMock Test - 98 (17 Jan 2023) Rotational DynamicsparamNo ratings yet
- Horizon Aviation Academy - HellasDocument2 pagesHorizon Aviation Academy - Hellas1n4r51ssNo ratings yet
- AK Khan Telecom Limited: Orientation ScheduleDocument2 pagesAK Khan Telecom Limited: Orientation Schedulemozammel80No ratings yet
- Aplicacion Corto 3Document5 pagesAplicacion Corto 3Garbel LemusNo ratings yet
- About JK TyreDocument10 pagesAbout JK TyreAshish Adholiya0% (1)
- Resume Goutam AdwantDocument3 pagesResume Goutam AdwantGoutamNo ratings yet
- CH 2 - Guide To Physics PracticalsDocument20 pagesCH 2 - Guide To Physics PracticalsNong Hm100% (2)
- TDS - Emaco R907 PlusDocument2 pagesTDS - Emaco R907 PlusVenkata RaoNo ratings yet
- Project Final Report TemplateDocument14 pagesProject Final Report Templatemonparaashvin0% (1)
- NCERT Solutions For Class 12 Physics Chapter 3 Current ElectricityDocument24 pagesNCERT Solutions For Class 12 Physics Chapter 3 Current ElectricityDileep GNo ratings yet
- Semantic Segmentation Data Labelling: Classes and InstructionsDocument9 pagesSemantic Segmentation Data Labelling: Classes and InstructionsMar FieldsNo ratings yet
- General Biology 1: TEST II. Modified True or False. Indicate Whether The Statement Is True or False. If False, Change TheDocument2 pagesGeneral Biology 1: TEST II. Modified True or False. Indicate Whether The Statement Is True or False. If False, Change TheMA. HAZEL TEOLOGONo ratings yet
- 6yc Multifunction Meter: Operation ManualDocument46 pages6yc Multifunction Meter: Operation ManualHamish JosephNo ratings yet
- Ae tt8 Progress Test 3Document7 pagesAe tt8 Progress Test 3Joana Silva100% (1)
- Solutions To Mathematical Statistics With Applications, Pg. 409, Ex. 39Document5 pagesSolutions To Mathematical Statistics With Applications, Pg. 409, Ex. 39Ivi DownhamNo ratings yet
- Understanding Computer InvestigationsDocument64 pagesUnderstanding Computer InvestigationsLillian KobusingyeNo ratings yet