Download as pdf or txt
You might also like
- Health Insurance PolicyDocument8 pagesHealth Insurance Policyashwani kumar rai71% (7)
- Tata AIG Health Insurance PDFDocument4 pagesTata AIG Health Insurance PDFSrijan Tiwari80% (5)
- Nursing Care Plan (Acute Pain For Ceasarean Birth) HYPOTHETICALDocument2 pagesNursing Care Plan (Acute Pain For Ceasarean Birth) HYPOTHETICALmarife84% (19)
- Exam Saq Revision QuestionsDocument5 pagesExam Saq Revision QuestionsFarhana Azmira AsmadiNo ratings yet
- Utilizing Okra (Abelmoschus Esculentus) and Citrus Fruits As Hand SanitizerDocument27 pagesUtilizing Okra (Abelmoschus Esculentus) and Citrus Fruits As Hand SanitizerPaula Marie Llido80% (5)
- Star Health and Allied Insurance Company LTDDocument3 pagesStar Health and Allied Insurance Company LTDKishan NandamuriNo ratings yet
- Proposal 231211 141032Document4 pagesProposal 231211 141032endapallikartheeNo ratings yet
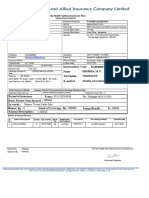
- Star Health and Allied Insurance Company LTD Family Health Optima Insurance PlanDocument4 pagesStar Health and Allied Insurance Company LTD Family Health Optima Insurance PlanRavi Shankar KolluruNo ratings yet
- Star Health and Allied Insurance Company LTD Star Comprehensive Insurance PolicyDocument4 pagesStar Health and Allied Insurance Company LTD Star Comprehensive Insurance PolicyBalamurugan ArumugamNo ratings yet
- Doc1Document3 pagesDoc1kushalNo ratings yet
- OS06691234 - Vinnarasi Juliette PDFDocument4 pagesOS06691234 - Vinnarasi Juliette PDFlayaNo ratings yet
- PRP 23 7000179227PRP 23 7000179227Document7 pagesPRP 23 7000179227PRP 23 7000179227Arvind KumarNo ratings yet
- LVGI Policy ProposalDocument2 pagesLVGI Policy Proposals KollaNo ratings yet
- Star Health and Allied Insurance Company LTDDocument4 pagesStar Health and Allied Insurance Company LTDSagar ADNo ratings yet
- Navi Gi PolicyDocumentSA01DZKIDocument27 pagesNavi Gi PolicyDocumentSA01DZKIabhinav soniNo ratings yet
- Proposal Form ScheduleDocument3 pagesProposal Form ScheduleIndra MishraNo ratings yet
- JB503916 Bab2c NB 00 20201209164847 1Document10 pagesJB503916 Bab2c NB 00 20201209164847 1SatishSubramanianNo ratings yet
- Abhay KumarDocument5 pagesAbhay KumarSunil SahNo ratings yet
- Group Mediprime Certificate of Insurance: 380-Bsa-Dn188271Document4 pagesGroup Mediprime Certificate of Insurance: 380-Bsa-Dn188271Sangwan ParveshNo ratings yet
- PRPFRM 612409754889 V1.0Document8 pagesPRPFRM 612409754889 V1.0anurag singhNo ratings yet
- 80 D Religare Health Insurace Premium Receipt Rs.21347Document7 pages80 D Religare Health Insurace Premium Receipt Rs.21347Shree Sai Enterprise100% (1)
- Navi Health Insurance PolicyDocument20 pagesNavi Health Insurance PolicyAbhishek GadeNo ratings yet
- CR ViewerDocument2 pagesCR ViewerJehan ZebNo ratings yet
- HDFC 3Document37 pagesHDFC 3System SinghNo ratings yet
- PDF 16932270 1584486557515 PDFDocument7 pagesPDF 16932270 1584486557515 PDFLucky TraderNo ratings yet
- Shubham Kalbhor HealthDocument5 pagesShubham Kalbhor Healthpj14061986No ratings yet
- Navi Gi PolicyDocumentG RA01JH1SDocument18 pagesNavi Gi PolicyDocumentG RA01JH1SSameer shaikNo ratings yet
- Anita ShindeDocument1 pageAnita ShindeDeshmukh ViratNo ratings yet
- Navi Health Insurance PolicyDocument21 pagesNavi Health Insurance Policysrinivas kNo ratings yet
- Welcome To Bajaj Allianz Family: Jasleen KaurDocument8 pagesWelcome To Bajaj Allianz Family: Jasleen Kaurbawa sagguNo ratings yet
- Navi Gi PolicyDocumentRA000N9Y 1Document21 pagesNavi Gi PolicyDocumentRA000N9Y 1harishNo ratings yet
- Navi Gi PolicyDocumentRA00101Q 1Document23 pagesNavi Gi PolicyDocumentRA00101Q 1Syed RuksarNo ratings yet
- Policy 85769629 27062024Document4 pagesPolicy 85769629 27062024faisalshaikh91422No ratings yet
- Iob Health Care Plus Policy Proposal FormDocument2 pagesIob Health Care Plus Policy Proposal FormPritamjit RoutNo ratings yet
- Document (1)Document20 pagesDocument (1)MILAN BEHERANo ratings yet
- You Have Made A Wise Choice: Here's Your Arogya Sanjeevani CertificateDocument7 pagesYou Have Made A Wise Choice: Here's Your Arogya Sanjeevani CertificateVishw KaduNo ratings yet
- Policy DocDocument4 pagesPolicy DocSudipta DhaliNo ratings yet
- Policy DocDocument7 pagesPolicy DocAdwaitDeshpandeNo ratings yet
- PolicyDocument8 pagesPolicyjoshiaruna539No ratings yet
- GurbaniDocument4 pagesGurbanimeetu2102No ratings yet
- Instructions For Filling The FormDocument2 pagesInstructions For Filling The Formyash kavitaNo ratings yet
- Declaration of Good Health Cum Membership Form: Life InsuranceDocument2 pagesDeclaration of Good Health Cum Membership Form: Life InsuranceAkshay JagdaleNo ratings yet
- GEMI Application Form - Two Wheeler LoansDocument5 pagesGEMI Application Form - Two Wheeler LoansLuckyNo ratings yet
- Navi Health Insurance PolicyDocument21 pagesNavi Health Insurance PolicySamani PlyNo ratings yet
- Policy DocDocument2 pagesPolicy DocAnusha GholeNo ratings yet
- Health Ins ReceiptDocument3 pagesHealth Ins ReceiptAayush KaulNo ratings yet
- PN2889050000702952Document5 pagesPN2889050000702952singhbhanuprakash28No ratings yet
- Policy 70576558 29082023Document8 pagesPolicy 70576558 29082023anantkantgNo ratings yet
- PDF 17017375 1584486767998 PDFDocument6 pagesPDF 17017375 1584486767998 PDFLucky TraderNo ratings yet
- Health InsuranceDocument7 pagesHealth InsuranceRadhika Rampal100% (1)
- BharatDocument3 pagesBharatravi kumarNo ratings yet
- 42404461Document5 pages42404461tyagishahroof786No ratings yet
- Saral Suraksha Bima, Plan - Preposal Form - v1Document3 pagesSaral Suraksha Bima, Plan - Preposal Form - v1rajeshNo ratings yet
- HEALTHDocument4 pagesHEALTHpj14061986No ratings yet
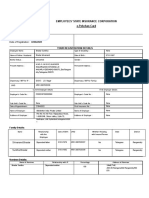
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 pagesEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of Registrationsupport officeNo ratings yet
- I Pru SPC - Member Consent Form - ICICI Bank COVID-19Document2 pagesI Pru SPC - Member Consent Form - ICICI Bank COVID-19Raj ANo ratings yet
- 10789103Document7 pages10789103Sachit MalikNo ratings yet
- Wa0012Document8 pagesWa0012freshmail.conNo ratings yet
- Policy 75532363 02122023Document8 pagesPolicy 75532363 02122023kpandya21No ratings yet
- GAL PreauthQueryLetter NON GMC CLMG 2023 231214 1278945 1672231896488Document2 pagesGAL PreauthQueryLetter NON GMC CLMG 2023 231214 1278945 1672231896488vikashNo ratings yet
- PDF 17145960 1585132385521 PDFDocument7 pagesPDF 17145960 1585132385521 PDFLucky TraderNo ratings yet
- How to Make Your Credit Card Rights Work for You: Save MoneyFrom EverandHow to Make Your Credit Card Rights Work for You: Save MoneyNo ratings yet
- It’s All About Money and Politics: Winning the Healthcare War: Your Guide to Healthcare ReformFrom EverandIt’s All About Money and Politics: Winning the Healthcare War: Your Guide to Healthcare ReformNo ratings yet
- Policy ClauseDocument14 pagesPolicy ClauseYogy YNo ratings yet
- VageeswariDocument6 pagesVageeswariYogy YNo ratings yet
- Maths Iia (Em)Document4 pagesMaths Iia (Em)Yogy YNo ratings yet
- CamScanner 05-04-2021 15.12.45Document3 pagesCamScanner 05-04-2021 15.12.45Yogy YNo ratings yet
- ICSE Class 9 Chemistry Chapter 01 Matter and Its CompositionDocument12 pagesICSE Class 9 Chemistry Chapter 01 Matter and Its CompositionYogy YNo ratings yet
- 2 - Structure of Atom Work SheetDocument4 pages2 - Structure of Atom Work SheetYogy YNo ratings yet
- 07 07 2022 FT Xvi TD Jeem Key - SolDocument18 pages07 07 2022 FT Xvi TD Jeem Key - SolYogy YNo ratings yet
- Final Jee-Main Examination - July, 2022: Chemistry Test Paper With SolutionDocument6 pagesFinal Jee-Main Examination - July, 2022: Chemistry Test Paper With SolutionYogy YNo ratings yet
- Final Jee-Main Examination - July, 2022: Physics Test Paper With SolutionDocument9 pagesFinal Jee-Main Examination - July, 2022: Physics Test Paper With SolutionYogy YNo ratings yet
- Krishna Reddy'S Sri Chaitanya: Week End - 3Document6 pagesKrishna Reddy'S Sri Chaitanya: Week End - 3Yogy YNo ratings yet
- Krishna Reddy'S Sri Chaitanya: Week End - 1Document5 pagesKrishna Reddy'S Sri Chaitanya: Week End - 1Yogy YNo ratings yet
- Krishna Reddy'S Sri Chaitanya: Week End - 2Document6 pagesKrishna Reddy'S Sri Chaitanya: Week End - 2Yogy YNo ratings yet
- Krishna Reddy'S Sri Chaitanya: Week End - 5Document6 pagesKrishna Reddy'S Sri Chaitanya: Week End - 5Yogy YNo ratings yet
- 7.nuclear Chemistry and Environmental Chemistry ExerciseDocument38 pages7.nuclear Chemistry and Environmental Chemistry ExerciseYogy YNo ratings yet
- Krishna Reddy'S Sri Chaitanya: Week End - 4Document6 pagesKrishna Reddy'S Sri Chaitanya: Week End - 4Yogy YNo ratings yet
- IX Circular MotionDocument2 pagesIX Circular MotionYogy YNo ratings yet
- గోరంత దీపాలు (ప్రక్రియ, ప్రశ్నలు)Document6 pagesగోరంత దీపాలు (ప్రక్రియ, ప్రశ్నలు)Yogy YNo ratings yet
- Motion in A Straight LineDocument14 pagesMotion in A Straight LineYogy YNo ratings yet
- 1.current ElectricityDocument147 pages1.current ElectricityYogy YNo ratings yet
- X - Biology Work Sheet - 1Document2 pagesX - Biology Work Sheet - 1Yogy YNo ratings yet
- UNIT - 10 Redox Reactions: Multiple Choice QuestionsDocument9 pagesUNIT - 10 Redox Reactions: Multiple Choice QuestionsYogy YNo ratings yet
- English Work Sheet - 1Document4 pagesEnglish Work Sheet - 1Yogy YNo ratings yet
- SR - Iit - Incomming-Cosaprk&Spark, Ic Ncert - Jee Main Model: Physics MAX - MARKS: 100Document8 pagesSR - Iit - Incomming-Cosaprk&Spark, Ic Ncert - Jee Main Model: Physics MAX - MARKS: 100Yogy YNo ratings yet
- Revised SR Inter (Bco, LX, ZX) Ipe SchedulesDocument5 pagesRevised SR Inter (Bco, LX, ZX) Ipe SchedulesYogy YNo ratings yet
- Psychoanalytic Infant ObservationDocument4 pagesPsychoanalytic Infant ObservationSergiuNo ratings yet
- CVS Case - OSDocument11 pagesCVS Case - OSUjjwal Bhardwaj100% (1)
- Domestic Hydrogen QRA ARUPDocument144 pagesDomestic Hydrogen QRA ARUPkzlpNo ratings yet
- Nursing Responsibilities For METRONIDAZOLEDocument1 pageNursing Responsibilities For METRONIDAZOLEIsrael Soria Espero63% (8)
- Multi-Unit Implant Impression Accuracy: A Review of The LiteratureDocument13 pagesMulti-Unit Implant Impression Accuracy: A Review of The LiteratureRafaela VillamaguaNo ratings yet
- Five Feet Apart (2019) 파이브피트-5p SampleDocument5 pagesFive Feet Apart (2019) 파이브피트-5p SampleAhmad ZakhiNo ratings yet
- Panic Stations - 02 - More About PanicDocument8 pagesPanic Stations - 02 - More About PanicGillian Tan IlaganNo ratings yet
- AOA ConjunctivitisDocument33 pagesAOA ConjunctivitiseloooyiyNo ratings yet
- Using The PartographDocument26 pagesUsing The PartographJulie May SuganobNo ratings yet
- Nurs FPX 4900 Assessment 5 Intervention Presentation and Capstone Video ReflectionDocument5 pagesNurs FPX 4900 Assessment 5 Intervention Presentation and Capstone Video Reflectionfarwaamjad771No ratings yet
- Breech Presentation - PPT (Read-Only)Document5 pagesBreech Presentation - PPT (Read-Only)Nestor SantiagoNo ratings yet
- Condo Central November 2008 IssueDocument100 pagesCondo Central November 2008 Issuecondocentral100% (5)
- Ross 308 PS PO 2011Document12 pagesRoss 308 PS PO 2011Anonymous jZGG7PpNo ratings yet
- Surgical Hip Dislocation Is More Powerful Than Arthro - 2019 - Orthopaedics - TRDocument6 pagesSurgical Hip Dislocation Is More Powerful Than Arthro - 2019 - Orthopaedics - TRIuliana MoiseNo ratings yet
- Sun PDFDocument17 pagesSun PDFAmanda MillerNo ratings yet
- Safety Alert - Grinder WheelDocument3 pagesSafety Alert - Grinder WheelsarojNo ratings yet
- Q Stock Obat Awaln NDCDocument8 pagesQ Stock Obat Awaln NDCiriantiNo ratings yet
- The Science Behind Actigin®: Associated Effects On The Human Body Based On Research FindingsDocument3 pagesThe Science Behind Actigin®: Associated Effects On The Human Body Based On Research FindingsLuis Castro XtrmNo ratings yet
- Clinical HypnosisDocument6 pagesClinical Hypnosisyazhini sasiNo ratings yet
- Kriya Sarira MCQ EnglishDocument10 pagesKriya Sarira MCQ EnglishSruthi Kunaparaju100% (2)
- Lesson Plan in Health IV JonaDocument8 pagesLesson Plan in Health IV JonaJenelyn Limen100% (1)
- Presented by - R Hemamalini 2010CYZ8795 Group G1Document29 pagesPresented by - R Hemamalini 2010CYZ8795 Group G1h_rajagopalan100% (1)
- Case Press Ob WardDocument9 pagesCase Press Ob Wardjohn castroNo ratings yet
- The Pathophysiology of Pneumonia: Therese Jane F. Timbalopez Bachelor of Science in Nursing 2ADocument17 pagesThe Pathophysiology of Pneumonia: Therese Jane F. Timbalopez Bachelor of Science in Nursing 2Ajoyrena ochondraNo ratings yet
- Revision Test 4 - Class 12D1 2021-2022Document7 pagesRevision Test 4 - Class 12D1 2021-2022Tenebrae LuxNo ratings yet
- Orientation To HospitalsDocument97 pagesOrientation To HospitalsSwati KhandelwalNo ratings yet
- 0610 s19 QP 43 PDFDocument20 pages0610 s19 QP 43 PDFrachitNo ratings yet