
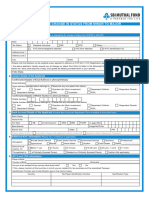
Electronic Fund Transfer (EFT) Authorization: Provider Information
Electronic Fund Transfer (EFT) Authorization: Provider Information
You might also like
- Auto Loan For Individual and Single Proprietorship - Application FormDocument2 pagesAuto Loan For Individual and Single Proprietorship - Application FormEymard Siojo67% (3)
- Ps 3881 XDocument1 pagePs 3881 XcolindownesNo ratings yet
- Edi FormDocument2 pagesEdi Formapi-240084111No ratings yet
- Direct Deposit FormDocument3 pagesDirect Deposit FormRabindra ShakyaNo ratings yet
- EFI Application Form SUPPLEMENTARY PDFDocument1 pageEFI Application Form SUPPLEMENTARY PDFJhoie GeeCeeNo ratings yet
- UTI - Minor To Major FormDocument2 pagesUTI - Minor To Major FormAMIT PANDEY100% (1)
- Broadcom 2011 Product BrochureDocument20 pagesBroadcom 2011 Product BrochureJeremy WatsonNo ratings yet
- Electronic Funds Transfer (Eft) Authorization Agreement: Part I: Reason For SubmissionDocument3 pagesElectronic Funds Transfer (Eft) Authorization Agreement: Part I: Reason For SubmissionAfzal ImamNo ratings yet
- Electronic Funds Transfer (Eft) Authorization Agreement: Page 1 of 3Document3 pagesElectronic Funds Transfer (Eft) Authorization Agreement: Page 1 of 3JayNo ratings yet
- Canada EngDocument3 pagesCanada Engpaolomarabella8No ratings yet
- TIAA Bank - Add Account HolderDocument2 pagesTIAA Bank - Add Account HolderDavid BuchananNo ratings yet
- Fulcrum Direct Deposit EFTAuthorization FormDocument2 pagesFulcrum Direct Deposit EFTAuthorization FormRON THOMTONNo ratings yet
- Direct Deposit Authorization For Electronic Funds Transfer (EFT)Document2 pagesDirect Deposit Authorization For Electronic Funds Transfer (EFT)Marcy MarkNo ratings yet
- Supplier or Payee RequestDocument2 pagesSupplier or Payee RequestAnnmary JojoNo ratings yet
- TN Enrollment Document For 87726 Created 6-12-2023 37731414Document2 pagesTN Enrollment Document For 87726 Created 6-12-2023 37731414kalinalveyNo ratings yet
- 1199 A 1 PDFDocument4 pages1199 A 1 PDFGerry Ruff100% (1)
- Cigna Claim FormDocument2 pagesCigna Claim FormLoganBohannonNo ratings yet
- ACH W9 FillableDocument1 pageACH W9 FillableEAZY CHARNo ratings yet
- P38 - Change To Personal Details FormDocument1 pageP38 - Change To Personal Details FormPancho G ReyesNo ratings yet
- UnitedHealthCare Fillable Reconsideration FormDocument1 pageUnitedHealthCare Fillable Reconsideration FormDavid R. GonzálezNo ratings yet
- Bank Account Updation FormDocument2 pagesBank Account Updation Forms.sabapathyNo ratings yet
- Vendor File Request Form - BlankDocument2 pagesVendor File Request Form - Blanknisa16fitiaNo ratings yet
- Cigna Global Claim FormDocument3 pagesCigna Global Claim Formrsiabs marketingNo ratings yet
- Supplier Direct Deposit Form 2020 7 2Document1 pageSupplier Direct Deposit Form 2020 7 2dannygNo ratings yet
- Mam Form For Change in Status From Minor To MajorDocument2 pagesMam Form For Change in Status From Minor To MajorPratap PratapNo ratings yet
- GEN-GEN-41-G01 - Change of Banking Details - External GuideDocument8 pagesGEN-GEN-41-G01 - Change of Banking Details - External GuideKriben RaoNo ratings yet
- EFT Request FormDocument2 pagesEFT Request Formekuhni2012No ratings yet
- Ohip ApplicationDocument4 pagesOhip Applicationapi-310747685No ratings yet
- Wire Transfer Request Form - 2220745Document3 pagesWire Transfer Request Form - 2220745Michael KimNo ratings yet
- Sf1199a 870601V01Document2 pagesSf1199a 870601V01jefe_e578726No ratings yet
- VoguePay 2Document3 pagesVoguePay 2islamNo ratings yet
- Description: Tags: FP0409Document4 pagesDescription: Tags: FP0409anon-451079No ratings yet
- Add Power of Attorney: 1. Account Holder InformationDocument3 pagesAdd Power of Attorney: 1. Account Holder InformationDavid BuchananNo ratings yet
- TCF-ICEE Credit Application 11 081Document1 pageTCF-ICEE Credit Application 11 081jasonparker80No ratings yet
- Din Form: Provisional Director Identification Number (DIN)Document2 pagesDin Form: Provisional Director Identification Number (DIN)Niraj HarodiaNo ratings yet
- Direct Deposit FormDocument3 pagesDirect Deposit FormSreenivas RaoNo ratings yet
- Zipcash KYC FormDocument2 pagesZipcash KYC FormhemanthbolemNo ratings yet
- Withdrawal Great American Life FormsDocument13 pagesWithdrawal Great American Life FormsMax PowerNo ratings yet
- Ag 501Document2 pagesAg 501Cindy FazzinoNo ratings yet
- Missouri Direct Deposit FormDocument2 pagesMissouri Direct Deposit FormitargetingNo ratings yet
- Direct Deposit Enrollment & Changes: SECTION 1: Annuitant InformationDocument3 pagesDirect Deposit Enrollment & Changes: SECTION 1: Annuitant InformationdesireeNo ratings yet
- Form D - Supplier Information SheetDocument1 pageForm D - Supplier Information SheetvinuNo ratings yet
- E VisaDocument3 pagesE Visazahoorunisa20No ratings yet
- Warehouse Donation Request 090214Document1 pageWarehouse Donation Request 090214butada basuraNo ratings yet
- Psychiatric Rehabilitation FACILITYDocument23 pagesPsychiatric Rehabilitation FACILITYkwonjuNo ratings yet
- Ofs Era Claim FormDocument2 pagesOfs Era Claim Formbanira.luv3000No ratings yet
- YSA Claim Form (NPC) 11.12.2010Document2 pagesYSA Claim Form (NPC) 11.12.2010Joanna ClarkNo ratings yet
- Service Request Form: (9-Digit Number Next To Your Cheque Number) ( 11 Character Code Printed On A Cheque / Passbook)Document2 pagesService Request Form: (9-Digit Number Next To Your Cheque Number) ( 11 Character Code Printed On A Cheque / Passbook)vatsonwizzluvNo ratings yet
- MAMForm forchangeinstatusfromMinortoMajorDocument2 pagesMAMForm forchangeinstatusfromMinortoMajorManish SinhaNo ratings yet
- In-Service Withdrawal FormDocument1 pageIn-Service Withdrawal FormlanzahouseNo ratings yet
- THMP Pic FormDocument2 pagesTHMP Pic FormMia JacksonNo ratings yet
- New Account Request: General InformationDocument6 pagesNew Account Request: General InformationHussein SeetalNo ratings yet
- EFT FormDocument1 pageEFT FormgavinNo ratings yet
- Cardmember Application, Individual Liability: (For Employees of Accenture)Document2 pagesCardmember Application, Individual Liability: (For Employees of Accenture)Ranajit SahuNo ratings yet
- Domestic Vendor Creation / Amendment Form: Supplier DetailsDocument2 pagesDomestic Vendor Creation / Amendment Form: Supplier DetailsLucas GomesNo ratings yet
- ICICI Bank Credit Card Address Change Request FormDocument2 pagesICICI Bank Credit Card Address Change Request FormDhavalNo ratings yet
- State Bank of India: Step 1 - Complete The Identification RequirementDocument8 pagesState Bank of India: Step 1 - Complete The Identification Requirementrafi617No ratings yet
- Saving Account OpeningDocument18 pagesSaving Account OpeningmoregauravNo ratings yet
- How to Make Your Credit Card Rights Work for You: Save MoneyFrom EverandHow to Make Your Credit Card Rights Work for You: Save MoneyNo ratings yet
- Design of Passive-Type Radar ReflectorDocument7 pagesDesign of Passive-Type Radar ReflectorRoman BabaevNo ratings yet
- Davis Echomaster 00152 153 157Document16 pagesDavis Echomaster 00152 153 157Roman BabaevNo ratings yet
- Engels Toolbox Life-Saving Rules - DEFDocument39 pagesEngels Toolbox Life-Saving Rules - DEFRoman BabaevNo ratings yet
- Engels Vouwkaart XS 54x85 ENG Web DEFDocument2 pagesEngels Vouwkaart XS 54x85 ENG Web DEFRoman BabaevNo ratings yet
- B63CDocument3 pagesB63CRoman BabaevNo ratings yet
- Fema Lifelines Card Template 2023Document2 pagesFema Lifelines Card Template 2023Roman BabaevNo ratings yet
- BABT Module B Exp 2022Document3 pagesBABT Module B Exp 2022Roman BabaevNo ratings yet
- Ritchie Helmsman Compass ManualDocument7 pagesRitchie Helmsman Compass ManualRoman BabaevNo ratings yet
- RLS AnnualReport2021 v2 LR SPGDocument80 pagesRLS AnnualReport2021 v2 LR SPGRoman BabaevNo ratings yet
- V-128 Operational and Technical Performance Requirement For VTS EquipmentDocument68 pagesV-128 Operational and Technical Performance Requirement For VTS EquipmentRoman BabaevNo ratings yet
- 89 New - Aton Radar Reflector Type IrrDocument2 pages89 New - Aton Radar Reflector Type IrrRoman BabaevNo ratings yet
- Poster A2 Eng DefDocument1 pagePoster A2 Eng DefRoman BabaevNo ratings yet
- Lyclear Dermal Cream: PermethrinDocument1 pageLyclear Dermal Cream: PermethrinRoman BabaevNo ratings yet
- Imm 5280 eDocument4 pagesImm 5280 eRoman BabaevNo ratings yet
- ElectroRice ENGDocument2 pagesElectroRice ENGRoman BabaevNo ratings yet
- XDocument6 pagesXRoman BabaevNo ratings yet
- Terms of Use enDocument6 pagesTerms of Use enRoman BabaevNo ratings yet
- 5 - Threaded Fasteners PDFDocument41 pages5 - Threaded Fasteners PDFViven Sharma100% (1)
- SQL Select From V$SGADocument16 pagesSQL Select From V$SGAsaravanand1983100% (2)
- Iot Paper Ieee FormatDocument4 pagesIot Paper Ieee FormatKarthikeyan K Palanisamy100% (2)
- Robot Expert Quick Start GuideDocument141 pagesRobot Expert Quick Start GuideSF JM100% (12)
- QUIZ Answer MergedDocument31 pagesQUIZ Answer MergedPiyush GuptaNo ratings yet
- HIstogramDocument38 pagesHIstogramJerritta SNo ratings yet
- STR W6853 DatasheetDocument5 pagesSTR W6853 DatasheetBembenk PutraNo ratings yet
- User Manual - MaxQ 4000 Incubated and Refrigerated Shakers - 7004342 - 057-287-00 Rev. 7Document46 pagesUser Manual - MaxQ 4000 Incubated and Refrigerated Shakers - 7004342 - 057-287-00 Rev. 7Andrew HernandezNo ratings yet
- 2D Rotary EncodersDocument88 pages2D Rotary Encodersddsf2012No ratings yet
- Bridge Project Design 1 FirstDocument9 pagesBridge Project Design 1 FirstAfiq AimanNo ratings yet
- DroneDocument4 pagesDroneheni16belayNo ratings yet
- Unit - Ii: Process PlanningDocument24 pagesUnit - Ii: Process PlanningJackson ..No ratings yet
- PDF2DWG Raster2VectorDocument2 pagesPDF2DWG Raster2VectorNanthawat BabybebNo ratings yet
- Free Download Here: Labview Core 1 PDFDocument2 pagesFree Download Here: Labview Core 1 PDFabrahamNo ratings yet
- USB Controller With External Amplifier and Recording FunctionDocument9 pagesUSB Controller With External Amplifier and Recording FunctioncdpangoNo ratings yet
- Problem SolutionsDocument6 pagesProblem SolutionsMuhammad Talha AtharNo ratings yet
- Sec 3 A Math Mock Exam WA2 2024Document8 pagesSec 3 A Math Mock Exam WA2 2024meredithtanyongenNo ratings yet
- Ladbrokes BettingDocument18 pagesLadbrokes BettingLevel BusinessNo ratings yet
- Juniper Baseline Operation GuideDocument380 pagesJuniper Baseline Operation GuideMushtaq HussainNo ratings yet
- Leakage Current - Part 2: Leakage Current Test App Note Figure # IEC60601-1 Figure #Document6 pagesLeakage Current - Part 2: Leakage Current Test App Note Figure # IEC60601-1 Figure #bigasribeNo ratings yet
- MEGA Solution Footprint V5Document17 pagesMEGA Solution Footprint V5Wissam ShehabNo ratings yet
- 5G Technology: By:-Kaushal, Mantra, Meet, PriyamDocument20 pages5G Technology: By:-Kaushal, Mantra, Meet, PriyamMantra PatelNo ratings yet
- Kenny 230723 Data Structures Interview QuestionsDocument16 pagesKenny 230723 Data Structures Interview QuestionsvanjchaoNo ratings yet
- Lesson 2 - CyberSecurity FundamentalsDocument132 pagesLesson 2 - CyberSecurity FundamentalsZozer Mbula Lwanga100% (2)
- HP Color Laserjet Pro M283Fdw: Extraordinary, Wireless Two-Sided Printing. Professional MFP Productivity, Plus FaxDocument2 pagesHP Color Laserjet Pro M283Fdw: Extraordinary, Wireless Two-Sided Printing. Professional MFP Productivity, Plus Faxthato mathogojaneNo ratings yet
- ON1 Photo Keyword AI User Guide PDFDocument91 pagesON1 Photo Keyword AI User Guide PDFmoneygain4everNo ratings yet
- ESE (Book) PDFDocument486 pagesESE (Book) PDFVir DavinderNo ratings yet
- Sound On Sound USA - May 2022Document172 pagesSound On Sound USA - May 2022gogettagadNo ratings yet
- Intelligent BuildingsDocument23 pagesIntelligent BuildingsMilosav Pusonjic MikiNo ratings yet









































































































Download as pdf or txt
You might also like
- Auto Loan For Individual and Single Proprietorship - Application FormDocument2 pagesAuto Loan For Individual and Single Proprietorship - Application FormEymard Siojo67% (3)
- Ps 3881 XDocument1 pagePs 3881 XcolindownesNo ratings yet
- Edi FormDocument2 pagesEdi Formapi-240084111No ratings yet
- Direct Deposit FormDocument3 pagesDirect Deposit FormRabindra ShakyaNo ratings yet
- EFI Application Form SUPPLEMENTARY PDFDocument1 pageEFI Application Form SUPPLEMENTARY PDFJhoie GeeCeeNo ratings yet
- UTI - Minor To Major FormDocument2 pagesUTI - Minor To Major FormAMIT PANDEY100% (1)
- Broadcom 2011 Product BrochureDocument20 pagesBroadcom 2011 Product BrochureJeremy WatsonNo ratings yet
- Electronic Funds Transfer (Eft) Authorization Agreement: Part I: Reason For SubmissionDocument3 pagesElectronic Funds Transfer (Eft) Authorization Agreement: Part I: Reason For SubmissionAfzal ImamNo ratings yet
- Electronic Funds Transfer (Eft) Authorization Agreement: Page 1 of 3Document3 pagesElectronic Funds Transfer (Eft) Authorization Agreement: Page 1 of 3JayNo ratings yet
- Canada EngDocument3 pagesCanada Engpaolomarabella8No ratings yet
- TIAA Bank - Add Account HolderDocument2 pagesTIAA Bank - Add Account HolderDavid BuchananNo ratings yet
- Fulcrum Direct Deposit EFTAuthorization FormDocument2 pagesFulcrum Direct Deposit EFTAuthorization FormRON THOMTONNo ratings yet
- Direct Deposit Authorization For Electronic Funds Transfer (EFT)Document2 pagesDirect Deposit Authorization For Electronic Funds Transfer (EFT)Marcy MarkNo ratings yet
- Supplier or Payee RequestDocument2 pagesSupplier or Payee RequestAnnmary JojoNo ratings yet
- TN Enrollment Document For 87726 Created 6-12-2023 37731414Document2 pagesTN Enrollment Document For 87726 Created 6-12-2023 37731414kalinalveyNo ratings yet
- 1199 A 1 PDFDocument4 pages1199 A 1 PDFGerry Ruff100% (1)
- Cigna Claim FormDocument2 pagesCigna Claim FormLoganBohannonNo ratings yet
- ACH W9 FillableDocument1 pageACH W9 FillableEAZY CHARNo ratings yet
- P38 - Change To Personal Details FormDocument1 pageP38 - Change To Personal Details FormPancho G ReyesNo ratings yet
- UnitedHealthCare Fillable Reconsideration FormDocument1 pageUnitedHealthCare Fillable Reconsideration FormDavid R. GonzálezNo ratings yet
- Bank Account Updation FormDocument2 pagesBank Account Updation Forms.sabapathyNo ratings yet
- Vendor File Request Form - BlankDocument2 pagesVendor File Request Form - Blanknisa16fitiaNo ratings yet
- Cigna Global Claim FormDocument3 pagesCigna Global Claim Formrsiabs marketingNo ratings yet
- Supplier Direct Deposit Form 2020 7 2Document1 pageSupplier Direct Deposit Form 2020 7 2dannygNo ratings yet
- Mam Form For Change in Status From Minor To MajorDocument2 pagesMam Form For Change in Status From Minor To MajorPratap PratapNo ratings yet
- GEN-GEN-41-G01 - Change of Banking Details - External GuideDocument8 pagesGEN-GEN-41-G01 - Change of Banking Details - External GuideKriben RaoNo ratings yet
- EFT Request FormDocument2 pagesEFT Request Formekuhni2012No ratings yet
- Ohip ApplicationDocument4 pagesOhip Applicationapi-310747685No ratings yet
- Wire Transfer Request Form - 2220745Document3 pagesWire Transfer Request Form - 2220745Michael KimNo ratings yet
- Sf1199a 870601V01Document2 pagesSf1199a 870601V01jefe_e578726No ratings yet
- VoguePay 2Document3 pagesVoguePay 2islamNo ratings yet
- Description: Tags: FP0409Document4 pagesDescription: Tags: FP0409anon-451079No ratings yet
- Add Power of Attorney: 1. Account Holder InformationDocument3 pagesAdd Power of Attorney: 1. Account Holder InformationDavid BuchananNo ratings yet
- TCF-ICEE Credit Application 11 081Document1 pageTCF-ICEE Credit Application 11 081jasonparker80No ratings yet
- Din Form: Provisional Director Identification Number (DIN)Document2 pagesDin Form: Provisional Director Identification Number (DIN)Niraj HarodiaNo ratings yet
- Direct Deposit FormDocument3 pagesDirect Deposit FormSreenivas RaoNo ratings yet
- Zipcash KYC FormDocument2 pagesZipcash KYC FormhemanthbolemNo ratings yet
- Withdrawal Great American Life FormsDocument13 pagesWithdrawal Great American Life FormsMax PowerNo ratings yet
- Ag 501Document2 pagesAg 501Cindy FazzinoNo ratings yet
- Missouri Direct Deposit FormDocument2 pagesMissouri Direct Deposit FormitargetingNo ratings yet
- Direct Deposit Enrollment & Changes: SECTION 1: Annuitant InformationDocument3 pagesDirect Deposit Enrollment & Changes: SECTION 1: Annuitant InformationdesireeNo ratings yet
- Form D - Supplier Information SheetDocument1 pageForm D - Supplier Information SheetvinuNo ratings yet
- E VisaDocument3 pagesE Visazahoorunisa20No ratings yet
- Warehouse Donation Request 090214Document1 pageWarehouse Donation Request 090214butada basuraNo ratings yet
- Psychiatric Rehabilitation FACILITYDocument23 pagesPsychiatric Rehabilitation FACILITYkwonjuNo ratings yet
- Ofs Era Claim FormDocument2 pagesOfs Era Claim Formbanira.luv3000No ratings yet
- YSA Claim Form (NPC) 11.12.2010Document2 pagesYSA Claim Form (NPC) 11.12.2010Joanna ClarkNo ratings yet
- Service Request Form: (9-Digit Number Next To Your Cheque Number) ( 11 Character Code Printed On A Cheque / Passbook)Document2 pagesService Request Form: (9-Digit Number Next To Your Cheque Number) ( 11 Character Code Printed On A Cheque / Passbook)vatsonwizzluvNo ratings yet
- MAMForm forchangeinstatusfromMinortoMajorDocument2 pagesMAMForm forchangeinstatusfromMinortoMajorManish SinhaNo ratings yet
- In-Service Withdrawal FormDocument1 pageIn-Service Withdrawal FormlanzahouseNo ratings yet
- THMP Pic FormDocument2 pagesTHMP Pic FormMia JacksonNo ratings yet
- New Account Request: General InformationDocument6 pagesNew Account Request: General InformationHussein SeetalNo ratings yet
- EFT FormDocument1 pageEFT FormgavinNo ratings yet
- Cardmember Application, Individual Liability: (For Employees of Accenture)Document2 pagesCardmember Application, Individual Liability: (For Employees of Accenture)Ranajit SahuNo ratings yet
- Domestic Vendor Creation / Amendment Form: Supplier DetailsDocument2 pagesDomestic Vendor Creation / Amendment Form: Supplier DetailsLucas GomesNo ratings yet
- ICICI Bank Credit Card Address Change Request FormDocument2 pagesICICI Bank Credit Card Address Change Request FormDhavalNo ratings yet
- State Bank of India: Step 1 - Complete The Identification RequirementDocument8 pagesState Bank of India: Step 1 - Complete The Identification Requirementrafi617No ratings yet
- Saving Account OpeningDocument18 pagesSaving Account OpeningmoregauravNo ratings yet
- How to Make Your Credit Card Rights Work for You: Save MoneyFrom EverandHow to Make Your Credit Card Rights Work for You: Save MoneyNo ratings yet
- Design of Passive-Type Radar ReflectorDocument7 pagesDesign of Passive-Type Radar ReflectorRoman BabaevNo ratings yet
- Davis Echomaster 00152 153 157Document16 pagesDavis Echomaster 00152 153 157Roman BabaevNo ratings yet
- Engels Toolbox Life-Saving Rules - DEFDocument39 pagesEngels Toolbox Life-Saving Rules - DEFRoman BabaevNo ratings yet
- Engels Vouwkaart XS 54x85 ENG Web DEFDocument2 pagesEngels Vouwkaart XS 54x85 ENG Web DEFRoman BabaevNo ratings yet
- B63CDocument3 pagesB63CRoman BabaevNo ratings yet
- Fema Lifelines Card Template 2023Document2 pagesFema Lifelines Card Template 2023Roman BabaevNo ratings yet
- BABT Module B Exp 2022Document3 pagesBABT Module B Exp 2022Roman BabaevNo ratings yet
- Ritchie Helmsman Compass ManualDocument7 pagesRitchie Helmsman Compass ManualRoman BabaevNo ratings yet
- RLS AnnualReport2021 v2 LR SPGDocument80 pagesRLS AnnualReport2021 v2 LR SPGRoman BabaevNo ratings yet
- V-128 Operational and Technical Performance Requirement For VTS EquipmentDocument68 pagesV-128 Operational and Technical Performance Requirement For VTS EquipmentRoman BabaevNo ratings yet
- 89 New - Aton Radar Reflector Type IrrDocument2 pages89 New - Aton Radar Reflector Type IrrRoman BabaevNo ratings yet
- Poster A2 Eng DefDocument1 pagePoster A2 Eng DefRoman BabaevNo ratings yet
- Lyclear Dermal Cream: PermethrinDocument1 pageLyclear Dermal Cream: PermethrinRoman BabaevNo ratings yet
- Imm 5280 eDocument4 pagesImm 5280 eRoman BabaevNo ratings yet
- ElectroRice ENGDocument2 pagesElectroRice ENGRoman BabaevNo ratings yet
- XDocument6 pagesXRoman BabaevNo ratings yet
- Terms of Use enDocument6 pagesTerms of Use enRoman BabaevNo ratings yet
- 5 - Threaded Fasteners PDFDocument41 pages5 - Threaded Fasteners PDFViven Sharma100% (1)
- SQL Select From V$SGADocument16 pagesSQL Select From V$SGAsaravanand1983100% (2)
- Iot Paper Ieee FormatDocument4 pagesIot Paper Ieee FormatKarthikeyan K Palanisamy100% (2)
- Robot Expert Quick Start GuideDocument141 pagesRobot Expert Quick Start GuideSF JM100% (12)
- QUIZ Answer MergedDocument31 pagesQUIZ Answer MergedPiyush GuptaNo ratings yet
- HIstogramDocument38 pagesHIstogramJerritta SNo ratings yet
- STR W6853 DatasheetDocument5 pagesSTR W6853 DatasheetBembenk PutraNo ratings yet
- User Manual - MaxQ 4000 Incubated and Refrigerated Shakers - 7004342 - 057-287-00 Rev. 7Document46 pagesUser Manual - MaxQ 4000 Incubated and Refrigerated Shakers - 7004342 - 057-287-00 Rev. 7Andrew HernandezNo ratings yet
- 2D Rotary EncodersDocument88 pages2D Rotary Encodersddsf2012No ratings yet
- Bridge Project Design 1 FirstDocument9 pagesBridge Project Design 1 FirstAfiq AimanNo ratings yet
- DroneDocument4 pagesDroneheni16belayNo ratings yet
- Unit - Ii: Process PlanningDocument24 pagesUnit - Ii: Process PlanningJackson ..No ratings yet
- PDF2DWG Raster2VectorDocument2 pagesPDF2DWG Raster2VectorNanthawat BabybebNo ratings yet
- Free Download Here: Labview Core 1 PDFDocument2 pagesFree Download Here: Labview Core 1 PDFabrahamNo ratings yet
- USB Controller With External Amplifier and Recording FunctionDocument9 pagesUSB Controller With External Amplifier and Recording FunctioncdpangoNo ratings yet
- Problem SolutionsDocument6 pagesProblem SolutionsMuhammad Talha AtharNo ratings yet
- Sec 3 A Math Mock Exam WA2 2024Document8 pagesSec 3 A Math Mock Exam WA2 2024meredithtanyongenNo ratings yet
- Ladbrokes BettingDocument18 pagesLadbrokes BettingLevel BusinessNo ratings yet
- Juniper Baseline Operation GuideDocument380 pagesJuniper Baseline Operation GuideMushtaq HussainNo ratings yet
- Leakage Current - Part 2: Leakage Current Test App Note Figure # IEC60601-1 Figure #Document6 pagesLeakage Current - Part 2: Leakage Current Test App Note Figure # IEC60601-1 Figure #bigasribeNo ratings yet
- MEGA Solution Footprint V5Document17 pagesMEGA Solution Footprint V5Wissam ShehabNo ratings yet
- 5G Technology: By:-Kaushal, Mantra, Meet, PriyamDocument20 pages5G Technology: By:-Kaushal, Mantra, Meet, PriyamMantra PatelNo ratings yet
- Kenny 230723 Data Structures Interview QuestionsDocument16 pagesKenny 230723 Data Structures Interview QuestionsvanjchaoNo ratings yet
- Lesson 2 - CyberSecurity FundamentalsDocument132 pagesLesson 2 - CyberSecurity FundamentalsZozer Mbula Lwanga100% (2)
- HP Color Laserjet Pro M283Fdw: Extraordinary, Wireless Two-Sided Printing. Professional MFP Productivity, Plus FaxDocument2 pagesHP Color Laserjet Pro M283Fdw: Extraordinary, Wireless Two-Sided Printing. Professional MFP Productivity, Plus Faxthato mathogojaneNo ratings yet
- ON1 Photo Keyword AI User Guide PDFDocument91 pagesON1 Photo Keyword AI User Guide PDFmoneygain4everNo ratings yet
- ESE (Book) PDFDocument486 pagesESE (Book) PDFVir DavinderNo ratings yet
- Sound On Sound USA - May 2022Document172 pagesSound On Sound USA - May 2022gogettagadNo ratings yet
- Intelligent BuildingsDocument23 pagesIntelligent BuildingsMilosav Pusonjic MikiNo ratings yet