Download as pdf or txt
You might also like
- All Knowmedge Internal Medicine FlashcardDocument22 pagesAll Knowmedge Internal Medicine Flashcardrub100% (4)
- 2013 0667 TK Geo 13 ENG.123Document112 pages2013 0667 TK Geo 13 ENG.123SURYANo ratings yet
- Addisons DiseaseDocument12 pagesAddisons DiseaseChinju CyrilNo ratings yet
- Addison Disease: Diagnosis and Initial ManagementDocument4 pagesAddison Disease: Diagnosis and Initial ManagementTeguh RahNo ratings yet
- Contribuciones de Leontief A La EconomíaDocument24 pagesContribuciones de Leontief A La EconomíaMargarita SepulvedaNo ratings yet
- 30 Manuscript Addison's DiseaseDocument10 pages30 Manuscript Addison's Diseasekint manlangitNo ratings yet
- Addison SlidesDocument59 pagesAddison Slidesmarianatilla2016No ratings yet
- Adrenal Insufficiency & Addison'S Disease: April 13, 2016Document6 pagesAdrenal Insufficiency & Addison'S Disease: April 13, 2016Chino Paolo SamsonNo ratings yet
- Ijss May Cr01Document4 pagesIjss May Cr01DinaNo ratings yet
- Cushings, Addisons and Acromegaly: DR J Storrow FY2Document38 pagesCushings, Addisons and Acromegaly: DR J Storrow FY2abdalkhalidNo ratings yet
- REPORTDocument13 pagesREPORTEarlou MagbanuaNo ratings yet
- Addison' S Disease: Case PresentationDocument34 pagesAddison' S Disease: Case PresentationShane Olanosa PillonarNo ratings yet
- Addison's Disease: Endocrine GlandsDocument4 pagesAddison's Disease: Endocrine GlandsfynneroNo ratings yet
- Involuntary Weight Loss (GSH)Document39 pagesInvoluntary Weight Loss (GSH)AchmadRizaNo ratings yet
- Addison DiseaseDocument23 pagesAddison DiseaseKompari EvansNo ratings yet
- 6 year Topic 6 Methodical recommendations. Аdrenal insufficiencyDocument10 pages6 year Topic 6 Methodical recommendations. Аdrenal insufficiencyAmrut LovesmusicNo ratings yet
- Clinical Biochimesrt ReportDocument5 pagesClinical Biochimesrt ReportTaha JasimNo ratings yet
- Pituitary Gland Diseases: HypopituitarismDocument9 pagesPituitary Gland Diseases: HypopituitarismAsh AshNo ratings yet
- Addison's DiseaseDocument17 pagesAddison's DiseaseDan AliNo ratings yet
- Progressive Muscle Weakness: More There Than Meets The Eye: Im Board ReviewDocument7 pagesProgressive Muscle Weakness: More There Than Meets The Eye: Im Board Reviewbdalcin5512No ratings yet
- Endocrinology Teaching CasesDocument47 pagesEndocrinology Teaching CasesBinta BaptisteNo ratings yet
- Adrenal Insufficiency and AddisonDocument10 pagesAdrenal Insufficiency and AddisonFarooq Bin MahfoozNo ratings yet
- Endocrinology-II Past Papers 3rd Year-1Document11 pagesEndocrinology-II Past Papers 3rd Year-1Syed Muhammad HameemNo ratings yet
- Involuntary Weight Loss (GSH)Document30 pagesInvoluntary Weight Loss (GSH)Febriliana Mao-maoNo ratings yet
- ActivityDocument21 pagesActivityAbdullah ElgeddawyNo ratings yet
- Cushing's Syndrome, Addison's Disease and Hyperparathyroidism.Document29 pagesCushing's Syndrome, Addison's Disease and Hyperparathyroidism.pranjl100% (1)
- Ug NotesDocument538 pagesUg NotesSteven IStudy SmithNo ratings yet
- Addison's DiseaseDocument22 pagesAddison's DiseaseKarl Jose75% (4)
- Anovulatory InfertilityDocument57 pagesAnovulatory InfertilityUsha AnengaNo ratings yet
- Adrenocortical DisordersDocument73 pagesAdrenocortical DisordersReunita ConstantiaNo ratings yet
- Systemic Lupus ErythematosusDocument27 pagesSystemic Lupus ErythematosusMega AnandaNo ratings yet
- Addison S DiseaseDocument12 pagesAddison S DiseaseChristian MartinezNo ratings yet
- EndokrinDocument27 pagesEndokrinSarah Putri AbellysaNo ratings yet
- Book: Mayo Clinic Family Health Book, 5th EditionDocument11 pagesBook: Mayo Clinic Family Health Book, 5th Editionnimra ansarNo ratings yet
- Endocrinology Best RDocument27 pagesEndocrinology Best RfrabziNo ratings yet
- Endocrinology Course Content: Semester (5) Clinical Pharmacy CourseDocument91 pagesEndocrinology Course Content: Semester (5) Clinical Pharmacy CourseSadigMukhNo ratings yet
- EN8 - HypercortisolismDocument11 pagesEN8 - Hypercortisolismsbobine.imsNo ratings yet
- Addison's Disease 1Document6 pagesAddison's Disease 1Yang YangNo ratings yet
- Addison Disease, Penyakit AddisonDocument11 pagesAddison Disease, Penyakit AddisonKertiasihwayanNo ratings yet
- Addison's DiseaseDocument57 pagesAddison's DiseaseVie Delvia100% (4)
- Final Final Male Hypogonadism-1Document102 pagesFinal Final Male Hypogonadism-1Hassan TahseenNo ratings yet
- Activity 2 MetabsDocument10 pagesActivity 2 MetabsCalvin Keith YadaoNo ratings yet
- 632 Ijar-5063Document6 pages632 Ijar-5063Putri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- Case Presentation On CKD/AKIDocument29 pagesCase Presentation On CKD/AKIsalma.nasr003No ratings yet
- Case Hipertensi SekunderDocument8 pagesCase Hipertensi Sekunderkintan utariNo ratings yet
- Research Paper On Addisons DiseaseDocument8 pagesResearch Paper On Addisons Diseasetug0l0byh1g2100% (1)
- Addison’s Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandAddison’s Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Adrenal Insufficiency and Addison's DiseaseDocument8 pagesAdrenal Insufficiency and Addison's DiseaseFredy RizkiNo ratings yet
- Adrenal Crisis: Risk FactorsDocument25 pagesAdrenal Crisis: Risk Factorspwinzizitah063No ratings yet
- Addison's DiseaseDocument9 pagesAddison's Diseaseash ashNo ratings yet
- Addison's DiseaseDocument17 pagesAddison's DiseaseMah Jezthy100% (1)
- Endocrine DiseaseDocument61 pagesEndocrine DiseasedivyaNo ratings yet
- Adrenal CrisisDocument4 pagesAdrenal CrisisRichie Marie BajaNo ratings yet
- The Patient With Rhabdomyolysis: Have You Considered Quail Poisoning?Document2 pagesThe Patient With Rhabdomyolysis: Have You Considered Quail Poisoning?andriopaNo ratings yet
- Adrenal InsufficiencyDocument11 pagesAdrenal InsufficiencyAustine OsaweNo ratings yet
- Addisions Disease Alternative Names: Return To TopDocument9 pagesAddisions Disease Alternative Names: Return To TopSuhas IngaleNo ratings yet
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocument46 pagesAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupNo ratings yet
- IDA HOMEWORK (2016510024-Putri Nurhisiyah Madya Jamil)Document9 pagesIDA HOMEWORK (2016510024-Putri Nurhisiyah Madya Jamil)Shanon LimNo ratings yet
- Adrenal Cortex and Medulla - The Clinical ContextDocument10 pagesAdrenal Cortex and Medulla - The Clinical ContextbluesaltNo ratings yet
- Adrenal Gland PathologyDocument62 pagesAdrenal Gland Pathologytatti999No ratings yet
- Adrenal Insufficiency and Addison's DiseaseDocument8 pagesAdrenal Insufficiency and Addison's DiseaseyancefinceNo ratings yet
- 3 2packetDocument6 pages3 2packetapi-327561261No ratings yet
- Narrative Text by Marco Class A Morning Lectuer: Hamid Asman, S.PDDocument12 pagesNarrative Text by Marco Class A Morning Lectuer: Hamid Asman, S.PDMardiana DhyanNo ratings yet
- Chemical Technicians 10-2021Document30 pagesChemical Technicians 10-2021PRC Baguio0% (1)
- Zupcasti Par B-F B 35Document4 pagesZupcasti Par B-F B 35Stefan MilojevicNo ratings yet
- Hydraulic Fracturing DesignDocument14 pagesHydraulic Fracturing DesignRichard ChanNo ratings yet
- NFRCS Therm 5.2-July 06versionDocument302 pagesNFRCS Therm 5.2-July 06versionBojan Bjelajac100% (1)
- Film Boiling Condensation ManualDocument3 pagesFilm Boiling Condensation ManualSyafIq AimanNo ratings yet
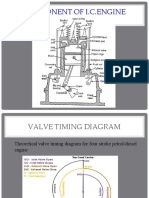
- Valve Timing DiagramDocument43 pagesValve Timing Diagramѕυdeѕн ĸNo ratings yet
- Mass SongsDocument20 pagesMass SongsJason LayaNo ratings yet
- Inspection and Test Plan - Steel AssemblyDocument1 pageInspection and Test Plan - Steel AssemblyAvinash LalNo ratings yet
- Science Mentor Guide of HOTS 2022Document34 pagesScience Mentor Guide of HOTS 2022Ike LeeNo ratings yet
- Sub Zero Service Manual - IW-30CIDocument65 pagesSub Zero Service Manual - IW-30CIMarco ThrushNo ratings yet
- Form 2 - Industrial Training Visitation ReportDocument2 pagesForm 2 - Industrial Training Visitation ReportWong Mun HoeNo ratings yet
- RCCDocument10 pagesRCCGautam KhadkaNo ratings yet
- Indian Maritime University: Section-A (12x 1 12 Marks) (Answer All Questions) Choose The Correct AnswerDocument4 pagesIndian Maritime University: Section-A (12x 1 12 Marks) (Answer All Questions) Choose The Correct AnswerAmitrajeet kumarNo ratings yet
- Quarter 3 - Module 1-W3: Computer Systems Servicing (CSS)Document3 pagesQuarter 3 - Module 1-W3: Computer Systems Servicing (CSS)AC BalioNo ratings yet
- MPCA Response 5.29.20Document2 pagesMPCA Response 5.29.20Duluth News TribuneNo ratings yet
- Bone Marrow and Stem Cell TranspplantDocument28 pagesBone Marrow and Stem Cell TranspplantVILLEJO JHOVIALENNo ratings yet
- A B C - S of Hoodoo - Tina HarrisDocument152 pagesA B C - S of Hoodoo - Tina HarrisDarío Ol100% (11)
- Opmanager Plus Product Information Sheet 1Document49 pagesOpmanager Plus Product Information Sheet 1Nghiêm Sỹ Tâm PhươngNo ratings yet
- Midwifery: Kelly Ackerson, PHD, RN, WHNP-BC, Ruth Zielinski, PHD, CNM, FacnmDocument26 pagesMidwifery: Kelly Ackerson, PHD, RN, WHNP-BC, Ruth Zielinski, PHD, CNM, FacnmMILANo ratings yet
- Datasheet - Trimble SX12 - English US - ScreenDocument4 pagesDatasheet - Trimble SX12 - English US - ScreenJeline AmanteNo ratings yet
- M2 Imalis Schedule 2021-2022-: July 21StDocument1 pageM2 Imalis Schedule 2021-2022-: July 21StMohammed Abdul Rahman KhanNo ratings yet
- Borchers Rheological Additives: For Waterborne Coating SystemsDocument6 pagesBorchers Rheological Additives: For Waterborne Coating Systemsrogerkid17No ratings yet
- 40 Day Language PracticeDocument29 pages40 Day Language PracticeAJ AndersonNo ratings yet
- Writing HWDocument5 pagesWriting HWMinh LêNo ratings yet
- Buku SDKIDocument246 pagesBuku SDKIAdi Pramono100% (1)