
GKNHS Tooth Extraction CONSENT
GKNHS Tooth Extraction CONSENT
You might also like
- Project Proposal WinsDocument3 pagesProject Proposal WinsEllen Mae CruzNo ratings yet
- IDH Citizens' Charter 2016Document22 pagesIDH Citizens' Charter 2016Mary Jean GelitoNo ratings yet
- Parental Influences and Academic Performance Among Nursing Students During COVID-19 Pandemic Transition Point: A Correlational StudyDocument18 pagesParental Influences and Academic Performance Among Nursing Students During COVID-19 Pandemic Transition Point: A Correlational StudyPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Good and Scates Criteria For ValidityDocument2 pagesGood and Scates Criteria For ValidityAile BogartNo ratings yet
- Implementation of School-Based Feeding Program Among The Elementary Schools in The School Division of Quezon Basis For Amendments On The SBFP Operational GuidelinesDocument15 pagesImplementation of School-Based Feeding Program Among The Elementary Schools in The School Division of Quezon Basis For Amendments On The SBFP Operational GuidelinesPsychology and Education: A Multidisciplinary Journal100% (1)
- Teaching A Lesson in Science 6 Through Explicit InstructionDocument1 pageTeaching A Lesson in Science 6 Through Explicit InstructionHazel L Ibarra100% (1)
- Governor Miguel Luis: Villafuerte JRDocument1 pageGovernor Miguel Luis: Villafuerte JRBlezel Mae AlzagaNo ratings yet
- Rcy-Membership FormDocument1 pageRcy-Membership FormJasper Astillero CailingNo ratings yet
- Certificate of AppearanceDocument2 pagesCertificate of AppearanceArthur BenecarioNo ratings yet
- Ages School Canteen Report 2022 2023Document3 pagesAges School Canteen Report 2022 2023Redempcion P QuiambaoNo ratings yet
- Deworming PermitDocument1 pageDeworming PermitAlvin Wilfred Ogot100% (1)
- Kagawaran NG Edukasyon: Integrative Assessment Quarter 2-Grade 6: Week 1-2 For The Teacher GDocument4 pagesKagawaran NG Edukasyon: Integrative Assessment Quarter 2-Grade 6: Week 1-2 For The Teacher GGessle GamirNo ratings yet
- Homeroom Guidance Monitoring Tool Long PortraitDocument3 pagesHomeroom Guidance Monitoring Tool Long PortraitRamil Almoite50% (2)
- Republic of The Philippines Department of Education: Tugbo Integrated SchoolDocument2 pagesRepublic of The Philippines Department of Education: Tugbo Integrated SchoolJemuel Castillo100% (1)
- Accomplishment ReportDocument1 pageAccomplishment ReportChe Valenzuela100% (1)
- School Board Meeting ReflectionDocument3 pagesSchool Board Meeting Reflectionapi-302398531No ratings yet
- Mental Health Action PlanDocument1 pageMental Health Action PlanJudah Ben Ng Ducusin100% (1)
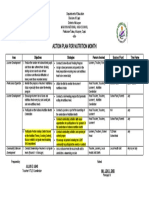
- Action Plan For Nutrition Month: Learner DevelopmentDocument1 pageAction Plan For Nutrition Month: Learner Developmentjulius ubasNo ratings yet
- Letter of IntentDocument1 pageLetter of IntentMartin Capucion50% (2)
- GESP AY 2021-2022 Forms and AgreementDocument21 pagesGESP AY 2021-2022 Forms and AgreementMPDO LGU San AndresNo ratings yet
- CVFDocument18 pagesCVFshurreiNo ratings yet
- 2nd HRPTA - Minutes of The MeetingDocument2 pages2nd HRPTA - Minutes of The MeetingMafey DadivasNo ratings yet
- Memorandum Deped DewormingDocument1 pageMemorandum Deped DewormingKristin Villasenot100% (1)
- Pilot Testing - Letter To BrgyDocument1 pagePilot Testing - Letter To BrgyCara Basnic Lagura100% (1)
- Guidance Program Sy 2022-2023Document2 pagesGuidance Program Sy 2022-2023Lorena RomeroNo ratings yet
- Monitoring Tool For Functional School ClinicDocument5 pagesMonitoring Tool For Functional School ClinicYatts De La Cuesta100% (1)
- Appearance Certificate BlankDocument2 pagesAppearance Certificate Blankalvin_isipNo ratings yet
- Techno Hiv Summit CertificateDocument8 pagesTechno Hiv Summit CertificateVenice RaieNo ratings yet
- D Epartment of E Ducation: R Epublic of The P HilippinesDocument3 pagesD Epartment of E Ducation: R Epublic of The P HilippinesAlmira AguadoNo ratings yet
- Department of Social Welfare and Development 4ps Cvs TemplateDocument1 pageDepartment of Social Welfare and Development 4ps Cvs TemplateSelda Venturayo-Nebril CabusasNo ratings yet
- School Clinic Action Plan-2023-2024Document3 pagesSchool Clinic Action Plan-2023-2024May Cordero PamunagNo ratings yet
- Adopt A Barangay Program EditedDocument6 pagesAdopt A Barangay Program Editedrichele valenciaNo ratings yet
- CIVIL SERVICE FORM 41 Medical CertificateDocument1 pageCIVIL SERVICE FORM 41 Medical CertificateElc Elc ElcNo ratings yet
- Program Proper MañanitaDocument2 pagesProgram Proper MañanitaCogie PeraltaNo ratings yet
- Matias B. Salvador Memorial Elementary School: Republic of The Philippines Department of EducationDocument3 pagesMatias B. Salvador Memorial Elementary School: Republic of The Philippines Department of EducationGuia Marie Diaz BriginoNo ratings yet
- Department of Education: School Dental Health Care Program (SDHCP) Monitoring ToolDocument3 pagesDepartment of Education: School Dental Health Care Program (SDHCP) Monitoring Toollowella formento100% (1)
- Emcee ScriptDocument3 pagesEmcee ScriptAlex Abonales DumandanNo ratings yet
- The Milestones of Polomolok Central Elementary SchoolDocument2 pagesThe Milestones of Polomolok Central Elementary SchoolLee Ziel0% (1)
- Didactic UnitDocument3 pagesDidactic UnittareixaNo ratings yet
- Narrative Report 3rd YearDocument27 pagesNarrative Report 3rd YearKissMarje EsnobeRaNo ratings yet
- Derrick LetterDocument5 pagesDerrick LetterJosette Mae AtanacioNo ratings yet
- Feeding Action ResearchDocument5 pagesFeeding Action ResearchMaria Judelyn Grana TuaresNo ratings yet
- Campaign SpeechDocument1 pageCampaign SpeechYannah MarianoNo ratings yet
- Certification Mam EdnaDocument1 pageCertification Mam EdnaArmi Alcantara BautistaNo ratings yet
- SSG Classroom Officers List and Geographical Location FormDocument3 pagesSSG Classroom Officers List and Geographical Location FormEugene Salem AbulocNo ratings yet
- Accomplishment ReportDocument2 pagesAccomplishment ReportWena Mae CristobalNo ratings yet
- Project E-Localized: A Utilization of Electronic Books and Printed Localized Reading Materials To Enhance The Level of Reading Comprehension in Filipino of Grade ThreeDocument5 pagesProject E-Localized: A Utilization of Electronic Books and Printed Localized Reading Materials To Enhance The Level of Reading Comprehension in Filipino of Grade ThreePsychology and Education: A Multidisciplinary JournalNo ratings yet
- Other Trainings - SPMCDocument1 pageOther Trainings - SPMCRia Tiglao Fortugaliza100% (1)
- School Action Plan Research Sy 2022 2023Document2 pagesSchool Action Plan Research Sy 2022 2023AYESSA ROMUALDONo ratings yet
- Reflection Paper On Lecture Series 2 - Teaching Deaf Students Physical EducationDocument2 pagesReflection Paper On Lecture Series 2 - Teaching Deaf Students Physical EducationCatherine Sagario OliquinoNo ratings yet
- Action Plan Gulayan Sa Paaralan Program (GPP) S.Y. 2019 - 2020Document3 pagesAction Plan Gulayan Sa Paaralan Program (GPP) S.Y. 2019 - 2020Jessah Chris Eve ValleNo ratings yet
- Action Plan and Accomplishment Report (Indonesia)Document4 pagesAction Plan and Accomplishment Report (Indonesia)Ezra Angeli Cariño JoaquinNo ratings yet
- Gen. Santos Avenue, Bicutan, Taguig CityDocument16 pagesGen. Santos Avenue, Bicutan, Taguig CityArianne B. CabañezNo ratings yet
- Department of Education: Republic of The PhilippinesDocument6 pagesDepartment of Education: Republic of The PhilippinesJESSIE JAMES YAPAONo ratings yet
- CS Form No. 212 Attachment - Work Experience Sheet...Document3 pagesCS Form No. 212 Attachment - Work Experience Sheet...Jm uniteNo ratings yet
- Taal SHS 3rd NSED 2Document9 pagesTaal SHS 3rd NSED 2Elizalde Lopez PiolNo ratings yet
- Reading Validation TemplateDocument1 pageReading Validation TemplateAURORA BAUTISTANo ratings yet
- Solid Mixed With LiquidDocument2 pagesSolid Mixed With LiquidRaqueliza Molina Villapa100% (6)
- Catch Up Fridays AttendanceDocument6 pagesCatch Up Fridays AttendanceGladys CarreonNo ratings yet

























































Download as docx, pdf, or txt
You might also like
- Project Proposal WinsDocument3 pagesProject Proposal WinsEllen Mae CruzNo ratings yet
- IDH Citizens' Charter 2016Document22 pagesIDH Citizens' Charter 2016Mary Jean GelitoNo ratings yet
- Parental Influences and Academic Performance Among Nursing Students During COVID-19 Pandemic Transition Point: A Correlational StudyDocument18 pagesParental Influences and Academic Performance Among Nursing Students During COVID-19 Pandemic Transition Point: A Correlational StudyPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Good and Scates Criteria For ValidityDocument2 pagesGood and Scates Criteria For ValidityAile BogartNo ratings yet
- Implementation of School-Based Feeding Program Among The Elementary Schools in The School Division of Quezon Basis For Amendments On The SBFP Operational GuidelinesDocument15 pagesImplementation of School-Based Feeding Program Among The Elementary Schools in The School Division of Quezon Basis For Amendments On The SBFP Operational GuidelinesPsychology and Education: A Multidisciplinary Journal100% (1)
- Teaching A Lesson in Science 6 Through Explicit InstructionDocument1 pageTeaching A Lesson in Science 6 Through Explicit InstructionHazel L Ibarra100% (1)
- Governor Miguel Luis: Villafuerte JRDocument1 pageGovernor Miguel Luis: Villafuerte JRBlezel Mae AlzagaNo ratings yet
- Rcy-Membership FormDocument1 pageRcy-Membership FormJasper Astillero CailingNo ratings yet
- Certificate of AppearanceDocument2 pagesCertificate of AppearanceArthur BenecarioNo ratings yet
- Ages School Canteen Report 2022 2023Document3 pagesAges School Canteen Report 2022 2023Redempcion P QuiambaoNo ratings yet
- Deworming PermitDocument1 pageDeworming PermitAlvin Wilfred Ogot100% (1)
- Kagawaran NG Edukasyon: Integrative Assessment Quarter 2-Grade 6: Week 1-2 For The Teacher GDocument4 pagesKagawaran NG Edukasyon: Integrative Assessment Quarter 2-Grade 6: Week 1-2 For The Teacher GGessle GamirNo ratings yet
- Homeroom Guidance Monitoring Tool Long PortraitDocument3 pagesHomeroom Guidance Monitoring Tool Long PortraitRamil Almoite50% (2)
- Republic of The Philippines Department of Education: Tugbo Integrated SchoolDocument2 pagesRepublic of The Philippines Department of Education: Tugbo Integrated SchoolJemuel Castillo100% (1)
- Accomplishment ReportDocument1 pageAccomplishment ReportChe Valenzuela100% (1)
- School Board Meeting ReflectionDocument3 pagesSchool Board Meeting Reflectionapi-302398531No ratings yet
- Mental Health Action PlanDocument1 pageMental Health Action PlanJudah Ben Ng Ducusin100% (1)
- Action Plan For Nutrition Month: Learner DevelopmentDocument1 pageAction Plan For Nutrition Month: Learner Developmentjulius ubasNo ratings yet
- Letter of IntentDocument1 pageLetter of IntentMartin Capucion50% (2)
- GESP AY 2021-2022 Forms and AgreementDocument21 pagesGESP AY 2021-2022 Forms and AgreementMPDO LGU San AndresNo ratings yet
- CVFDocument18 pagesCVFshurreiNo ratings yet
- 2nd HRPTA - Minutes of The MeetingDocument2 pages2nd HRPTA - Minutes of The MeetingMafey DadivasNo ratings yet
- Memorandum Deped DewormingDocument1 pageMemorandum Deped DewormingKristin Villasenot100% (1)
- Pilot Testing - Letter To BrgyDocument1 pagePilot Testing - Letter To BrgyCara Basnic Lagura100% (1)
- Guidance Program Sy 2022-2023Document2 pagesGuidance Program Sy 2022-2023Lorena RomeroNo ratings yet
- Monitoring Tool For Functional School ClinicDocument5 pagesMonitoring Tool For Functional School ClinicYatts De La Cuesta100% (1)
- Appearance Certificate BlankDocument2 pagesAppearance Certificate Blankalvin_isipNo ratings yet
- Techno Hiv Summit CertificateDocument8 pagesTechno Hiv Summit CertificateVenice RaieNo ratings yet
- D Epartment of E Ducation: R Epublic of The P HilippinesDocument3 pagesD Epartment of E Ducation: R Epublic of The P HilippinesAlmira AguadoNo ratings yet
- Department of Social Welfare and Development 4ps Cvs TemplateDocument1 pageDepartment of Social Welfare and Development 4ps Cvs TemplateSelda Venturayo-Nebril CabusasNo ratings yet
- School Clinic Action Plan-2023-2024Document3 pagesSchool Clinic Action Plan-2023-2024May Cordero PamunagNo ratings yet
- Adopt A Barangay Program EditedDocument6 pagesAdopt A Barangay Program Editedrichele valenciaNo ratings yet
- CIVIL SERVICE FORM 41 Medical CertificateDocument1 pageCIVIL SERVICE FORM 41 Medical CertificateElc Elc ElcNo ratings yet
- Program Proper MañanitaDocument2 pagesProgram Proper MañanitaCogie PeraltaNo ratings yet
- Matias B. Salvador Memorial Elementary School: Republic of The Philippines Department of EducationDocument3 pagesMatias B. Salvador Memorial Elementary School: Republic of The Philippines Department of EducationGuia Marie Diaz BriginoNo ratings yet
- Department of Education: School Dental Health Care Program (SDHCP) Monitoring ToolDocument3 pagesDepartment of Education: School Dental Health Care Program (SDHCP) Monitoring Toollowella formento100% (1)
- Emcee ScriptDocument3 pagesEmcee ScriptAlex Abonales DumandanNo ratings yet
- The Milestones of Polomolok Central Elementary SchoolDocument2 pagesThe Milestones of Polomolok Central Elementary SchoolLee Ziel0% (1)
- Didactic UnitDocument3 pagesDidactic UnittareixaNo ratings yet
- Narrative Report 3rd YearDocument27 pagesNarrative Report 3rd YearKissMarje EsnobeRaNo ratings yet
- Derrick LetterDocument5 pagesDerrick LetterJosette Mae AtanacioNo ratings yet
- Feeding Action ResearchDocument5 pagesFeeding Action ResearchMaria Judelyn Grana TuaresNo ratings yet
- Campaign SpeechDocument1 pageCampaign SpeechYannah MarianoNo ratings yet
- Certification Mam EdnaDocument1 pageCertification Mam EdnaArmi Alcantara BautistaNo ratings yet
- SSG Classroom Officers List and Geographical Location FormDocument3 pagesSSG Classroom Officers List and Geographical Location FormEugene Salem AbulocNo ratings yet
- Accomplishment ReportDocument2 pagesAccomplishment ReportWena Mae CristobalNo ratings yet
- Project E-Localized: A Utilization of Electronic Books and Printed Localized Reading Materials To Enhance The Level of Reading Comprehension in Filipino of Grade ThreeDocument5 pagesProject E-Localized: A Utilization of Electronic Books and Printed Localized Reading Materials To Enhance The Level of Reading Comprehension in Filipino of Grade ThreePsychology and Education: A Multidisciplinary JournalNo ratings yet
- Other Trainings - SPMCDocument1 pageOther Trainings - SPMCRia Tiglao Fortugaliza100% (1)
- School Action Plan Research Sy 2022 2023Document2 pagesSchool Action Plan Research Sy 2022 2023AYESSA ROMUALDONo ratings yet
- Reflection Paper On Lecture Series 2 - Teaching Deaf Students Physical EducationDocument2 pagesReflection Paper On Lecture Series 2 - Teaching Deaf Students Physical EducationCatherine Sagario OliquinoNo ratings yet
- Action Plan Gulayan Sa Paaralan Program (GPP) S.Y. 2019 - 2020Document3 pagesAction Plan Gulayan Sa Paaralan Program (GPP) S.Y. 2019 - 2020Jessah Chris Eve ValleNo ratings yet
- Action Plan and Accomplishment Report (Indonesia)Document4 pagesAction Plan and Accomplishment Report (Indonesia)Ezra Angeli Cariño JoaquinNo ratings yet
- Gen. Santos Avenue, Bicutan, Taguig CityDocument16 pagesGen. Santos Avenue, Bicutan, Taguig CityArianne B. CabañezNo ratings yet
- Department of Education: Republic of The PhilippinesDocument6 pagesDepartment of Education: Republic of The PhilippinesJESSIE JAMES YAPAONo ratings yet
- CS Form No. 212 Attachment - Work Experience Sheet...Document3 pagesCS Form No. 212 Attachment - Work Experience Sheet...Jm uniteNo ratings yet
- Taal SHS 3rd NSED 2Document9 pagesTaal SHS 3rd NSED 2Elizalde Lopez PiolNo ratings yet
- Reading Validation TemplateDocument1 pageReading Validation TemplateAURORA BAUTISTANo ratings yet
- Solid Mixed With LiquidDocument2 pagesSolid Mixed With LiquidRaqueliza Molina Villapa100% (6)
- Catch Up Fridays AttendanceDocument6 pagesCatch Up Fridays AttendanceGladys CarreonNo ratings yet