Download as pdf or txt
You might also like
- DSBPOPV26746Document2 pagesDSBPOPV26746Abha MahapatraNo ratings yet
- ReportDocument5 pagesReportajsangral194No ratings yet
- LabReportNew - 2023-07-29T172316.072Document6 pagesLabReportNew - 2023-07-29T172316.072Deependra YadavNo ratings yet
- 101 Test Aarogya 2.0:: Mrs - Phulwanti KaurDocument13 pages101 Test Aarogya 2.0:: Mrs - Phulwanti KaurNaunidh SinghNo ratings yet
- MR - SOMASEKHAR 4401 1339028Document2 pagesMR - SOMASEKHAR 4401 1339028Sampangi Bellary SomasekharNo ratings yet
- K SUJATHA-Female55 Years-927Document5 pagesK SUJATHA-Female55 Years-927vijaykumarNo ratings yet
- Aaop3438201-121123 2662Document1 pageAaop3438201-121123 2662fahadcaderNo ratings yet
- Machado PDFDocument4 pagesMachado PDFpm2001No ratings yet
- LabTest 29dec2023Document15 pagesLabTest 29dec2023Ayush KumarNo ratings yet
- FC1138497Document5 pagesFC1138497SK FahimNo ratings yet
- ReportDocument3 pagesReportFascino WhiteNo ratings yet
- Labreportnew AspxDocument2 pagesLabreportnew AspxAhana MondalNo ratings yet
- Laboratory Investigation Report::: Patient Name: Age/Sex:: Order Date Uhid: Ref. Doctor 2Document2 pagesLaboratory Investigation Report::: Patient Name: Age/Sex:: Order Date Uhid: Ref. Doctor 2tanmayNo ratings yet
- Date 24/dec/2022 08:32AM 03/dec/22 09:33AM 26/nov/22 09:05AM Unit Bio Ref IntervalDocument11 pagesDate 24/dec/2022 08:32AM 03/dec/22 09:33AM 26/nov/22 09:05AM Unit Bio Ref IntervalAmit SinghNo ratings yet
- Lab ReportDocument4 pagesLab ReportanilchowdaryNo ratings yet
- Bilas, Remedios Maloloy-On 2485027317Document5 pagesBilas, Remedios Maloloy-On 2485027317mjdigitalprint18No ratings yet
- Test ReportDocument2 pagesTest ReportChaudhary Ahmed IftikharNo ratings yet
- Report 2Document1 pageReport 2nhnreddyNo ratings yet
- PatientReport 2Document11 pagesPatientReport 2Sagarika MishraNo ratings yet
- PdfText - 2023-12-12T152233.242Document2 pagesPdfText - 2023-12-12T152233.242joshipriya208No ratings yet
- Test Name Result Biological Ref. Interval Method: Sodium FluorideDocument5 pagesTest Name Result Biological Ref. Interval Method: Sodium Fluorideumjadon2No ratings yet
- Wlifr1p4cvapn5otog23kbblDocument4 pagesWlifr1p4cvapn5otog23kbblGajanan KodnikarNo ratings yet
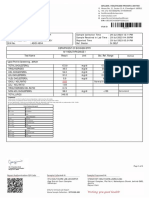
- Department of Biochemistry Iho - Rural Camp Package Test Name Result Unit Bio. Ref. RangeDocument4 pagesDepartment of Biochemistry Iho - Rural Camp Package Test Name Result Unit Bio. Ref. Rangethakurvikrant40678No ratings yet
- Hfi2em50gnsfhzbvravday4sDocument4 pagesHfi2em50gnsfhzbvravday4smishraamrit29No ratings yet
- 6364:07/12/2023 11:25:22 AM:Mr. Raman Singh:PH0004402539:34 (Y) /0 (M) /0 (D) :dr. Ankur N. Gupta:Male:SelfDocument6 pages6364:07/12/2023 11:25:22 AM:Mr. Raman Singh:PH0004402539:34 (Y) /0 (M) /0 (D) :dr. Ankur N. Gupta:Male:SelfSuryakant KumarNo ratings yet
- SR8767151Document2 pagesSR8767151imbipuldas14No ratings yet
- S28 - Likhitha Diagnostics Centre D.No:-2-177, Behind Gandhi Statue HYDRABAD-500039, AP. HyderabadDocument14 pagesS28 - Likhitha Diagnostics Centre D.No:-2-177, Behind Gandhi Statue HYDRABAD-500039, AP. HyderabadBhageerath AttheNo ratings yet
- ReportDocument7 pagesReportsri harshaNo ratings yet
- Efbu2630Document4 pagesEfbu2630Aniruddh NagaNo ratings yet
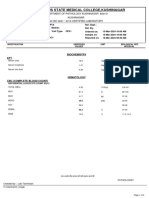
- Department of Haematology: Test Name Result Unit Bio. Ref. Range MethodDocument6 pagesDepartment of Haematology: Test Name Result Unit Bio. Ref. Range MethodJaya LakshmiNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveDocument5 pagesLaboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveP Nagaraju RajuNo ratings yet
- Bukurie MuhametajDocument1 pageBukurie Muhametajtironatirona455No ratings yet
- Lab Report NewDocument2 pagesLab Report NewPriya DubeyNo ratings yet
- Ajtj3770052-050224 2662Document1 pageAjtj3770052-050224 2662desilvamnimeshNo ratings yet
- Mrs - Lalita SharmaDocument8 pagesMrs - Lalita SharmaManju JaswalNo ratings yet
- 9443243103::::: Blood: Dhanvantri Nagar, Pondicherry - 605006, IndiaDocument1 page9443243103::::: Blood: Dhanvantri Nagar, Pondicherry - 605006, IndiaSurbhi JainNo ratings yet
- Wa0011.Document5 pagesWa0011.Akash TripathiNo ratings yet
- TrueDocument2 pagesTruedrdhananjaygupta9No ratings yet
- Mr. PAWAN JAINDocument1 pageMr. PAWAN JAINAshish BakliwalNo ratings yet
- Nnyy3999 PDFDocument2 pagesNnyy3999 PDFAshwin SagarNo ratings yet
- Department of Biochemistry Test Name Result Unit Bio. Ref. RangeDocument5 pagesDepartment of Biochemistry Test Name Result Unit Bio. Ref. RangeSudhanshuNo ratings yet
- Chemistry - I: TEST(s) Normal UNIT(s)Document1 pageChemistry - I: TEST(s) Normal UNIT(s)aaaNo ratings yet
- SnehaDocument3 pagesSneharazeena salamNo ratings yet
- Kongamdana: Clinical BiochemistryDocument5 pagesKongamdana: Clinical BiochemistryShariqNo ratings yet
- S28 - Mr. Kanthala Narender Reddy (Vedic Diagnostics) H.NO.-1-98/13/1, MADHAPUR, Hyderabad-500081, Telanagana ShaikpetDocument9 pagesS28 - Mr. Kanthala Narender Reddy (Vedic Diagnostics) H.NO.-1-98/13/1, MADHAPUR, Hyderabad-500081, Telanagana ShaikpetSiva rajNo ratings yet
- R11998655 Shruthi Nataras 070424065109Document1 pageR11998655 Shruthi Nataras 070424065109shruthia08No ratings yet
- Xrug7152 1 PDFDocument2 pagesXrug7152 1 PDFSarah ArpithaNo ratings yet
- Plot No.428, Phase-IV, Udyog Vihar, Gurgaon, Haryana - 122 015Document11 pagesPlot No.428, Phase-IV, Udyog Vihar, Gurgaon, Haryana - 122 015Pksk SkpkNo ratings yet
- Date 07/feb/2021 08:43AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument8 pagesDate 07/feb/2021 08:43AM Unit Bio Ref Interval: Laboratory Investigation ReportRaghav SinghNo ratings yet
- Ag83928800073199332 AlsDocument3 pagesAg83928800073199332 Alsanandk.bs7169No ratings yet
- 102 MR Rajesh Kumar Nanavati: BiochemistryDocument2 pages102 MR Rajesh Kumar Nanavati: BiochemistryRajesh NanavatiNo ratings yet
- Mama HP Resukts 10282023Document7 pagesMama HP Resukts 10282023AbieDiamanteNo ratings yet
- L96 - M/S Om Sai Path Lab Chiriyatand Khas Mahal More Patna BIHAR Mobile No:9334498936Document2 pagesL96 - M/S Om Sai Path Lab Chiriyatand Khas Mahal More Patna BIHAR Mobile No:9334498936sunny SINGHNo ratings yet
- Blood TestDocument2 pagesBlood TestAll You NeedNo ratings yet
- Department of Clinical Biochemistry: Investigation Name Result Bio. Ref. Range MethodDocument8 pagesDepartment of Clinical Biochemistry: Investigation Name Result Bio. Ref. Range MethodarupNo ratings yet
- Department of Biochemistry Test Name Result Unit Bio. Ref. RangeDocument3 pagesDepartment of Biochemistry Test Name Result Unit Bio. Ref. RangeAdityaNo ratings yet
- Labreportnew - 2024-03-15T102048.645Document4 pagesLabreportnew - 2024-03-15T102048.645AnkushNo ratings yet
- 100 Test Aarogya 2.0:: Mrs - Nisha KatouriaDocument18 pages100 Test Aarogya 2.0:: Mrs - Nisha KatouriaNisha KathuriaNo ratings yet
- Nanochromatography and Nanocapillary Electrophoresis: Pharmaceutical and Environmental AnalysesFrom EverandNanochromatography and Nanocapillary Electrophoresis: Pharmaceutical and Environmental AnalysesNo ratings yet
- AsyeywtyqwytqtyqDocument6 pagesAsyeywtyqwytqtyqRobee Camille Desabelle-SumatraNo ratings yet
- Good Ideas Ver 2Document2 pagesGood Ideas Ver 2testNo ratings yet
- TFN 01 19 2024 MateDocument5 pagesTFN 01 19 2024 MatemarigailedelacruzNo ratings yet
- Psych NotesDocument22 pagesPsych NotesArvinjohn GacutanNo ratings yet
- Real Rape Real PainDocument1 pageReal Rape Real PainfastbankingNo ratings yet
- Neuroconditions With AnswerDocument10 pagesNeuroconditions With AnswerYuvienco DrecoNo ratings yet
- 9 Natural Home Remedies and 4 Exercises To Fix Eye TwitchingDocument9 pages9 Natural Home Remedies and 4 Exercises To Fix Eye TwitchingQamar JamilNo ratings yet
- Type 2 Diabetes TreatmentDocument2 pagesType 2 Diabetes TreatmentRatnaPrasadNalamNo ratings yet
- HepatobiliaryDocument22 pagesHepatobiliarypaulandtess27No ratings yet
- Essential of Psychiatry For Asthenic and Dermatology PracticeDocument234 pagesEssential of Psychiatry For Asthenic and Dermatology PracticePsychiatry for ResidentsNo ratings yet
- Complication of Exodontia - 230507 - 034739Document9 pagesComplication of Exodontia - 230507 - 034739Mohammed K. AljaberyNo ratings yet
- Common Cancers in WomenDocument49 pagesCommon Cancers in WomenNaghib BogereNo ratings yet
- Linezolid Induced Toxic Optic Neuropathy.8Document3 pagesLinezolid Induced Toxic Optic Neuropathy.8arga LiannNo ratings yet
- Final Bio IADocument8 pagesFinal Bio IAVictor SERRANO100% (1)
- PN0211 Dysosmia FeaDocument5 pagesPN0211 Dysosmia FeasandaNo ratings yet
- Stones in Galbladder - Pitay Ki Pathri - Homeopathic MedicineDocument4 pagesStones in Galbladder - Pitay Ki Pathri - Homeopathic MedicineParwaz KamalNo ratings yet
- Spectrum of CT Find Ings in Rupture and Impending Rupture of Abdominal Aortic AneurysmsDocument3 pagesSpectrum of CT Find Ings in Rupture and Impending Rupture of Abdominal Aortic Aneurysmsgrarellano94No ratings yet
- Prisons and Health, 9 Infectious Diseases in PrisonDocument8 pagesPrisons and Health, 9 Infectious Diseases in PrisonBam ManNo ratings yet
- Braden ScaleDocument2 pagesBraden ScaleFrancis Alfred Escaran100% (1)
- Spinal PresentationDocument12 pagesSpinal PresentationavogadrocadoNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka: Pharmacology (RS3 & RS4) Q.P. CODE: 2710Document1 pageRajiv Gandhi University of Health Sciences, Karnataka: Pharmacology (RS3 & RS4) Q.P. CODE: 2710Nuhman Abdu RahmanNo ratings yet
- Health - Gastrointestinal DiseasesDocument6 pagesHealth - Gastrointestinal DiseasesMojaro SonNo ratings yet
- 1.understanding Cancer PPT LectureDocument184 pages1.understanding Cancer PPT LectureCherry Lou GuanzingNo ratings yet
- JCS-23-145 Doc 0 1Document5 pagesJCS-23-145 Doc 0 1Sabri AbyNo ratings yet
- Hope 1 - Q2 - M10Document14 pagesHope 1 - Q2 - M10Artlyne BunuanNo ratings yet
- Chicken Pox - NCPDocument2 pagesChicken Pox - NCPMaria Kyla VicenteNo ratings yet
- Full Download Book Translational Autoimmunity Volume 3 Autoimmune Disease Associated With Different Clinical Features PDFDocument41 pagesFull Download Book Translational Autoimmunity Volume 3 Autoimmune Disease Associated With Different Clinical Features PDFjohn.taylor275100% (26)
- FS11 Speech Pathologists Working With Older PeopleDocument2 pagesFS11 Speech Pathologists Working With Older Peopletammychance01No ratings yet
- Drug StudyDocument8 pagesDrug StudySamson, SatomiNo ratings yet
- LEK-obstetrics and GynecologyDocument102 pagesLEK-obstetrics and GynecologyDev RishabNo ratings yet