Professional Documents
Culture Documents
Nutrition Down Syndrome
Nutrition Down Syndrome
Uploaded by
Octavianus KevinOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Nutrition Down Syndrome
Nutrition Down Syndrome
Uploaded by
Octavianus KevinCopyright:
Available Formats
Review
Nutritional challenges in children and adolescents with
Down syndrome
Marianne Nordstrøm, Kjetil Retterstøl, Sigrun Hope, Svein Olav Kolset
Several features and comorbidities in Down syndrome have nutritional implications and consequences. In infancy Lancet Child Adolesc Health
and early childhood, children with Down syndrome have a high risk of oral motor difficulties and pharyngeal 2020; 4: 455–64
dysphagia with aspiration, which both require systematic attention. To improve nutritional status in children who are Department of Nutrition,
Institute of Basic Medical
underweight and who have clinical signs of feeding problems, further evaluation of underlying causes is required. Sciences, University of Oslo,
Clinical interventions should promote swallowing safety and development of feeding abilities. Even from 4–5 years of Oslo, Norway
age, overweight in children with Down syndrome can be a concern. To prevent disease later in life, an urgent need (M Nordstrøm PhD,
exists for more research on nutritional aspects in the prevention and treatment of obesity in adolescents with Down Prof K Retterstøl MD,
SO Kolset PhD); Frambu
syndrome. This Review did not find any data to support the use of dietary supplementation, except when deficiency is Resource Centre for Rare
documented. Additionally, the literature reported the need for more research that uses larger study samples and Disorders, Siggerud, Norway
control groups and that addresses important nutritional challenges in children and adolescents with Down syndrome. (M Nordstrøm); and Unit for
Inborn and Hereditary
Neuromuscular Disorders,
Introduction national Danish cohort of children with type 1 diabetes, Department of Neurology
Down syndrome is caused by trisomy of the whole or a the prevalence of Down syndrome was four-times higher (M Nordstrøm), Lipid Clinic
part of chromosome 21. It is the most common cause of than in the general population.12 (K Retterstøl), and Department
mild to moderate intellectual disability and affects around Guidelines have been developed to facilitate health of Neuro Habilitation
(S Hope MD), Oslo University
one in 800 to one in 900 liveborn infants, although this supervision in this patient group. These strategies Hospital, Oslo, Norway
prevalence varies between countries because of describe nutrition and physical activity as areas that Correspondence to:
differences in maternal age and prenatal screening.1,2 require ongoing assessment throughout childhood to Prof Svein Olav Kolset,
Children with Down syndrome have characteristic, establish and maintain healthy weight.13 Children with Department of Nutrition,
phenotypic features, delays in psychomotor development, Down syndrome have an increased risk of feeding Institute of Basic Medical
Sciences, University of Oslo,
and an increased rate of congenital malformations.3 On problems and obesity.14,15 It is well known that establish Oslo 0316, Norway
an individual level, children with Down syndrome show ment of healthy eating habits in childhood is important s.o.kolset@medisin.uio.no
large variability because some have mild symptoms and for the prevention of disease later in life and that
complications, whereas others are more severely affected. increasing longevity in Down syndrome is likely to
This variability also applies to the risk of health problems lead to increased manifestation of lifestyle-associated
related to nutrition in this patient group. diseases.16 Obesity is known to be associated with type 2
In children with Down syndrome, attention to diabetes, cardiovascular disease, and some types of
nutritional intake and status is important because
several features and comorbidities have nutritional
implications and consequences (panel). Key messages
When assessing nutrition in children and adolescents • Increased focus on nutritional measures is important for the health and wellbeing of
with Down syndrome, clinicians should be aware of children and adolescents with Down syndrome
health conditions that might influence nutritional care • Reduced feeding abilities with increased risk of dysphagia and aspiration are
and dietary advice. Congenital heart defects are found in predominant in the first years of life, and clinical screening for feeding problems and
approximately 45% of children with Down syndrome, evaluation of children with feeding difficulties, low weight gain, or underweight is
most often in the form of atrioventricular septum defect important in this phase
and ventricular septum defect.4 Anomalies in the • Excessive weight gain is a concern for many children with Down syndrome from
gastrointestinal tract (eg, duodenal atresia, Hirschsprung 4–5 years of age and investigations of energy requirements, nutritional intakes, and
disease, and anorectal malformations) occur in 4–6% of evaluation of clinical methods for assessment of overweight and obesity in Down
these children.5–7 The prevalence of coeliac disease is syndrome are required
increased in those with Down syndrome and has been • More in-depth studies with representative samples and controlled study designs that
shown to vary between different countries, but a use cutting edge methods and technologies are needed to develop strategies for
2018 meta-analysis showed a pooled prevalence of 5·8% evidence-based prevention and treatments of obesity in people with Down syndrome
in children and adults with Down syndrome compared • General recommendations for intakes of micronutrients in relation to age and gender
with 0·5–1% of people in the general population.8 should also be applied for children and adolescents with Down syndrome, as no
Additionally, children with Down syndrome have an evidence exists of beneficial clinical effects of intakes above these recommendations,
increased risk of comorbidities such as hypotonia and except when deficiency is reported
orofacial dysfunction that can affect the feeding ability of • The dual challenge of preventing the risk of undernutrition in the first year of living
the child,9 and thyroid disease (eg, hypothyroidism),10 and obesity in later years calls for systematic nutritional evaluations throughout
which can potentially affect energy metabolism. Auto childhood and adolescent years for people with Down syndrome
immunity is also increased in Down syndrome.11 In a
www.thelancet.com/child-adolescent Vol 4 June 2020 455
Review
Netherlands,7 55% in Israel,5 63% in Mexico,19 and 67% in
Panel: Clinical features of Down syndrome with nutritional Saudi Arabia.20 In an Italian study18 that included
relevance 560 children with Down syndrome, the mean duration of
• Hypotonia breastfeeding was 54 days (SD 111) compared with
• Oropharyngeal abnormalities 165 days (SD 120) in controls. Congenital malformations,
• Gastrointestinal malformations and dysmotility prematurity, perceived milk insufficiency, suckling
• Reduced growth rate difficulties, and maternal depression were factors found
• Hypothyroidism to restrict breastfeeding.5,18,20,21 Furthermore, admission of
• Coeliac disease neonates to hospital confers a risk of reduced breast
• Type 1 diabetes feeding.
• Intellectual disability In infants with Down syndrome aged 0–3 months,
• Behavioural and psychiatric disorders most parents describe extended feeding duration
(30–60 min).21 This duration could be exhausting for both
the child and parents. In these first few months after
birth, parents of a child with Down syndrome often
Monitoring of nutritional status experience stress and difficult emotions, such as shock
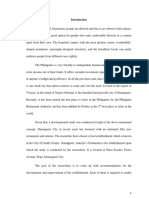
Screening
• Clinical examination of feeding ability
• Assessment of nutritional intake and use of supplementation
and grief, due to the diagnosis of the syndrome in their
• Measurement of weight and length or height and monitoring of growth pattern child. These emotions can further complicate feeding
• Annual blood test of iron status from 1 year of age practices. Frustration and depression in mothers have
been reported as influential factors in the termination of
breastfeeding.18,20
Poor feeding ability, low weight gain, or Excessive weight gain or overweight
Although some babies with Down syndrome struggle
underweight • Evaluation of feeding behaviours and physical with feeding initially, it is important to recognise that
• Refer infants and small children with feeding activity patterns most babies and mothers can make the transition to
Examination
problems to videofluoroscopic swallow • Measure thyroid-stimulating hormone
assessment in blood breastfeeding with time and guidance from competent
• Consider possible underlying causes such as health professionals.22 Thus, family-oriented support can
heart defects or gastrointestinal problems,
including gastrointestinal tract malformation,
enhance breastfeeding practice, facilitate early parent–
constipation, gastro-oesophageal reflux, and child bonding, and improve long-term child outcomes.22,23
coeliac disease
Feeding and swallowing problems
Relevant interventions Relevant interventions Children with Down syndrome often have reduced feeding
• Altered feeding techniques or adjustment • Education on healthy dietary choices and abilities and approximately 55–60% have problems with
Treatment
of food consistency portion sizes to parents and the child with
• Intervention to strengthen oral motor Down syndrome
feeding and swallowing.24,25 For a period, typically from age
function • Promote participation in regular physical 0–3 months, 13–40% of these children require a nasogastric
• Fortified diet or enteral nutrition activity tube for adequate nutrition5,21,26 and 2–5% receive gastro
• In coeliac disease, gluten-free diet
stomy.5,21 Children with an atrioventricular septal defect are
more likely to need gastrostomy.27
Figure: Suggested nutritional assessment in children with Down syndrome
For the early detection of feeding problems, all children
with Down syndrome should be clinically screened for
cancers. In Down syndrome, obesity is also linked to feeding and swallowing concerns (figure). Structural and
reduced functional abilities and activities of daily functional oropharyngeal abnormalities, immature neuro
living.17 Few previous reviews have assessed nutritional motor development, and hypotonia lead to decreased
aspects in this group. To further describe and explore neuromotor function and are associated with suckling
nutritional challenges in children and adolescents with problems, poor lip seal, dysphagia, and aspiration.9,21,25,28
Down syndrome, we searched and assessed the 64% of children with Down syndrome have been reported
scientific literature with the aim to describe feeding to have oral motor difficulties and 57% have been reported
abilities, nutritional intakes, and nutritional status in to have pharyngeal dysphagia with aspiration.25 Of those
this patient group and to provide some suggestions for with aspiration, almost all (90%) aspirated silently. In a
relevant clinical measures and interventions. 2019 study, aspiration was detected in 32% of infants with
Down syndrome before age 6 months and in 52% of
Infancy and breastfeeding children aged 6–12 months.29 In this study, children who
Most neonates with Down syndrome are offered human had a swallowing assessment after age 6 months were
milk, but the proportion and duration of exclusive more likely to have unchanged findings on follow-up than
breastfeeding are reduced compared with neonates children assessed before age 6 months. This finding
without Down syndrome.5,18 The number of children with suggests that timing of swallowing assessment could
Down syndrome who are exclusively breastfed varies potentially influence outcomes. High rates of pharyngeal
between countries from 43% in Italy,18 to 48% in the dysphagia were also described by O’Neill and colleagues,28
456 www.thelancet.com/child-adolescent Vol 4 June 2020
Review
who found that 116 (58%) of 201 children with Down food, holding food in the mouth without chewing,
syndrome were diagnosed after videofluoroscopic drooling, or preference for intense flavours. By contrast,
swallowing assessment. Accordingly, we suggest that behaviours typically seen in oral hypersensitivity are food
videofluoroscopic swallowing assessment should be selectivity regarding texture or temperature (often being
offered to children who present with clinical symptoms mistaken as being a so-called picky eater). Preference for
during meals (figure).24,25 In children with pharyngeal selected types of foods was reported as a common
dysphagia, this assessment should be followed by behaviour related to food in children with Down
recommendations of feeding modifications as needed. syndrome.36 Despite this patient group having higher
Relevant dietary interventions in a study of 46 children by rates of feeding problems and often lower feeding skills
Jackson and colleagues25 included thickened liquids in 34 than children without Down syndrome, no association
(74%) children, changed feeding procedure to control flow was observed between difficult mealtime behaviours
rate or bolus size in 5 (11%) children, and no oral intake in reported by the parent and the feeding skills of the child.37
4 (9%) children. Additionally, parents of toddlers with Down syndrome
The age at introduction to solid food is similar for both did not report more challenging mealtime behaviours
children with Down syndrome and those without Down than parents of children without Down syndrome of the
syndrome, with 46% of children with Down syndrome same age.37
introduced to solids at age 6–9 months and 38% at age
9–12 months.20 Nevertheless, learning to eat solid foods Parental feeding practices and eating
starting with pureed food and baby cereal and progressing behaviours
to regular table foods is a long process. Development of Reports on parental feeding practices have shown that
feeding abilities and self-feeding skills is, similarly to parents put less pressure on the child to eat, had greater
other developmental milestones, often delayed in weight concerns, and used more restrictions36 with the
children with Down syndrome.14,30 As the required skills child with Down syndrome than they did with the child’s
become more advanced, these children are increasingly siblings.38 Additionally, the use of restrictions and
delayed in their development and the age difference for monitoring of food intake were more frequent among
acquiring these skills increases between children with parents of overweight children with Down syndrome
and without Down syndrome.30 Feeding difficulties can than among parents of children with Down syndrome of
remain a challenge with problems predominantly related a healthy weight in a study of individuals (aged 2–9 years)
to oral motor function, followed by the pharyngeal phase with spina bifida, autism spectrum disorders, and Down
and the oesophageal phase in children with Down syndrome.39 In a study by Osaili and colleagues,36 47 (57%)
syndrome aged 2–7 years.14 In the oral phase, immature of 82 parents with a child with Down syndrome reported
chewing patterns and poor bolus control are common that their child frequently continued to eat as long as
concerns. In children aged 1–4 years, common difficulties food was present. The potential effect of parental practice
are encountered when food textures are chewy, firm, and on eating behaviour and the risk of overweight in young
gummy or rubbery; whereas, creamy, soft, and purée people with Down syndrome has not been properly
textures are often reported as more acceptable.31 However, investigated. Eating behaviour is an important issue to
with increased age, food textures that are crispy, dry, and address in future studies because it has potential
hard are more likely to be managed by the child.31 implications for both younger and older children related
Issues related to dental health are also highly relevant to the development of obesity.
in the assessment of feeding and swallowing issues in
children with Down syndrome, because these children Nutritional status
have an increased risk of dental abnormalities and severe The mean weight and length at birth is reduced in
tooth wear32,33 that can also potentially affect their ability to neonates with Down syndrome, with mean birthweight
chew. Parents and health professionals should be aware closer to the mean of unaffected children than birth
that extended bottle-feeding and use of a pacifier (for length.6 Reduced growth rate leading to final short stature
>24 months) have been associated with development of is a well known characteristic of people with Down
open bite and crossbite in children with Down syndrome.34 syndrome.
Structural training programmes that strengthen oral Growth charts for people with Down syndrome from
motor function and adjustment of food consistency birth to age 18–20 years have been developed on the basis
are relevant interventions for children with poor oro of several national cohorts.40–46 Traditionally, growth
pharyngeal motor abilities.35 In the study by Jackson and curves can be useful in children without Down syndrome
colleagues,25 28 (20%) of 138 children with a mean age of to monitor growth and nutritional status. For children
2·1 years (SD 3·2) also had difficulties with oral sensory with Down syndrome, weight-for-length charts that are
processing and could have benefited from interventions specific to their diagnosis can be used to screen for
that increased tolerance to facial and oral stimuli to growth faltering and wasting, but might be less precise
address such difficulties. Behaviour typically seen in oral in determining overweight than for those without Down
hyposensitivity includes overstuffing the mouth with syndrome.40
www.thelancet.com/child-adolescent Vol 4 June 2020 457
Review
As a consequence of the increased risk of overweight motor milestones, such as starting to walk after the age
and obesity, the mean body-mass index (BMI) percentile of 2 years.51 By contrast, in a larger cohort study of
for the age of children with Down syndrome increases 856 children with Down syndrome who had a mean age
during childhood when plotted on curves developed for of 8·8 years (SD 6·5), iron deficiency was more common
the general population. Based on data from a French (10% [18 children]) in children younger than 36 months
Down syndrome cohort,41 mean BMI was in the than in those older than 3 years (4% [28 children]).52 In
25th percentile in girls and boys aged 0–1 year. this study, in addition to haemoglobin parameters, other
Furthermore, mean BMI was in the 50th percentile in parameters are suggested, like ferritin and red cell
girls aged 3 years and in boys aged 4 years and, thereafter, distribution width. An Italian study showed that children
in the 75th percentile for girls aged 5 years and boys aged with Down syndrome had a high risk of low 25-hydroxy-
12 years of age. In adolescents aged 18 years, mean BMI vitamin D levels compared with controls, with 24 (77%)
was in the 80th percentile for girls and above the of 31 children having vitamin D deficiency.53 These
75th percentile for boys with Down syndrome.41 Therefore, studies suggest that blood tests for iron deficiency and
when BMI curves are used that are specific to Down vitamin levels could be of clinical importance.
syndrome, recognising that these curves only describe
the normal distribution of BMI values in the cohort and Obesity
do not necessarily represent an ideal weight status is Prevention and treatment of obesity are important issues
important.40,41 Plotting an individual on a BMI curve that for children and adolescents with Down syndrome. In a
is specific to Down syndrome only provides information review addressing overweight and obesity in children
about weight status in comparison with other people who and adolescents with Down syndrome, decreased energy
have Down syndrome. Subsequently, this type of curve expenditure at rest, increased leptin levels, untreated
can classify a person with Down syndrome to be a healthy hypothyroidism, unhealthy diet, and low physical activity
weight, although they would otherwise be classified as were described as factors that were likely to contribute to
overweight or obese with standard curves.47 However, excessive weight gain.15 In line with this hypothesis, a
because individuals with Down syndrome tend to have a 2018 study on total energy expenditure that used doubly
shorter stature, the curves and cutoffs developed for labelled water in nine children with Down syndrome
children without Down syndrome have been found to (mean 10·0 years [SD 3·9]) found that children with the
overestimate obesity and body fat percentage as meas condition required 500–800 fewer calories per day than
ured by dual-energy x-ray absorptiometry.48 Therefore, children without Down syndrome.54 However, studies on
additional examinations might be required to screen for nutritional intake did not find a decreased energy intake
overweight and obesity and associated health outcomes. in children with Down syndrome compared with
Measuring skinfolds at four locations (triceps, biceps, controls, but rather an increased energy intake55 or no
subscapular, and suprailiac) is an alternative method to difference in energy intake between children with and
assess adiposity and equations have been developed for without Down syndrome.56
children with reduced growth.49 Compared with the body Reduced cognitive abilities might influence food choices
fat percentage measured by dual-energy x-ray absorptio and activity levels in children. However, Jankowicz-
metry, the prediction equation for reduced growth, which Szymanska and colleagues57 found no clear correlation
was specifically developed for groups with health between the degree of intellectual disability and nutritional
conditions affecting growth, did well in children with status when adolescents with Down syndrome and mild
Down syndrome.49 Another option might be the use of intellectual disability were compared with other adolescents
waist circumference. A strong correlation (r=0·85) with Down syndrome and moderate intellectual disability.
between waist circumference measurements and body fat Poor knowledge of healthy foods has been described in
percentage measured by bioelectical impedance analysis children and adolescents with Down syndrome aged 11–18
has been described in a small study of 19 children and years.58 Even so, an intervention study that consisted of an
adolescents with Down syndrome.50 Even though these 18-session education programme on physical activity,
results indicate that bioelectical impedance analysis and healthy eating, and motivational skills only resulted in a
waist circumference could be promising methods in shift towards a decrease in the frequency of consumption
clinical practice, additional validation is required before of sweets, with no other changes in dietary habits
such methods could be recommended. observed.59
The prevalence of iron deficiency anaemia was To date, most interventions for obesity in children and
investigated in an uncontrolled study of 149 children and adolescents with Down syndrome have been based on
adolescents with Down syndrome (aged 0–20 years). exercise, with mixed and inconclusive effects on weight
This study found that 4 (5%) of 83 children who were loss.15 However, some studies have involved multi
younger than 10 years and 7 (14%) of 51 children aged 10 component interventions. In a small, 6-month nutrition
years or older had iron deficiency anaemia.51 This study and exercise intervention study (n=21), no weight loss
further described an association between a haemoglobin was observed in the group that received a 16-session
concentration that was lower than average and delays in nutrition and exercise education programme with
458 www.thelancet.com/child-adolescent Vol 4 June 2020
Review
Study design Age (years) Country Method Results
Magenis et al Case-control study (Down 5–18 Brazil Parent completed Higher intakes of energy, protein, and carbohydrates in Down syndrome group than
(2018)55 syndrome group n=19 and 3-day food record in control group; proportions of participants with intakes below RDA:
control group n=19) vitamin D 14 (74%), nicotinic acid 4 (21%), folic acid 5 (26%), pantothenic acid
7 (37%), calcium 5 (26%), and thiamine 2 (11%); no significant difference in
proportions with suboptimal intakes of micronutrients between Down syndrome
group and control group
Samarkandy et al Case-control study (Down 5–12 Saudi Arabia Parent completed No significant difference in energy intake between Down syndrome group and
(2012)56 syndrome group n=108 3-day food record sibling control group; significantly lower intakes of protein, vitamin A, riboflavin,
and control group n=113) calcium, and potassium in Down syndrome group than in controls
Grammatikopoulou Cross-sectional study (child 2–18 (child Greece Parent completed Highest intakes in total energy and macronutrients in adolescent group (as
et al (2008)61 Down syndrome group group aged 2–9 3-day food record expected); suboptimal intakes of micronutrients for children with Down syndrome
n=11 and adolescent Down and adolescent (presented as mean percentage of RDA): folic acid 81%, vitamin D 70%, vitamin E
syndrome group n=23) group aged 35%, vitamin K 49%, and iron 76%; suboptimal intakes of micronutrients for
10–18) adolescents with Down syndrome (presented as mean percentage of RDA): folic acid
84%, biotin 60%, vitamin D 94%, vitamin E 87%, vitamin K 43%, and calcium 90%
RDA=recommended dietary allowances.
Table 1: Studies on nutritional intake in children with Down syndrome
individualised plans for diet and exercise.60 Nevertheless, throughout the body. To ensure short-term and long-
in the group where parents also received education in term health, most countries have developed recom
behavioural strategies, such as diet and activity mendations for daily intakes. A study by Reza and
monitoring, short-term goal setting, and positive colleagues65 found that exercise, with and without intake
reinforcement, participants lost an average of 2·7 kg. At of calcium and vitamin D from enriched milk, had a
the 1-year follow-up visit, mean weight loss was 1·9 kg positive effect on bone mineral density in children with
from baseline weight.60 This study indicates the potential Down syndrome (table 2). The interventions in this
importance of family-oriented interventions and study mimic the general recommendations of physical
education for successful weight loss and maintenance, activity and intakes of calcium and vitamin D from foods
but needs to be further evaluated in larger samples. and provide some evidence that adherence to these
recommendations also has positive effects on bone
Nutritional intake and assessment health in children with Down syndrome.65 Likewise, in a
Assessment of nutritional intake is an essential component study by Stagi and colleagues,53 a positive but inadequate
in the prevention and treatment of abnormal weight status effect was shown when children and adolescents with
and micronutrient deficits. However, few studies have Down syndrome who had low baseline levels of
addressed dietary intakes in children and adolescents with 25-hydroxy vitamin D were supplemented with
Down syndrome and no specific dietary pattern in this 10 µg/day of vitamin D3. This study did not investigate
group has been shown to be associated with an increased total intake of vitamin D in the diet, but described a
risk of overweight.15 Intakes below recommended dietary reduced intake of vitamin D from fortified milk in the
allowances of various micronutrients were found in some group of participants with Down syndrome (table 2).
individuals.55,61 Compared with siblings, reduced intakes of The study indicates the importance of adequate
protein and particular micronutrients have also been vitamin D intake to prevent low vitamin D status and
documented (table 1).56 Parents of young children are most that adherence to general recommendations might be
often able to present an accurate picture of their child’s inadequate in people with Down syndrome who already
typical dietary habits and nutritional intake. Because of the have a deficiency.
widespread use of dietary supplements in children with The presence of an extra copy of chromosome 21 causes
Down syndrome,62 all assessments of nutritional intake in an overexpression of genes located on this chromosome
this population should include questions about use of and further metabolic alterations that lead to increased
herbal and dietary supplements. As children with Down levels of oxidative stress and abnormalities in zinc metab
syndrome grow older, additional methods might be olism.72,73 Subsequently, dietary interventions involving
required to provide adequate dietary data. Technology- higher intakes of supplements of selected antioxidants,
based methods like image-based food records accessible by vitamins, and minerals than general recommendations
mobile phone have been found to be accepted, feasible, have been hypothesised to contribute to the normalisation
and promising for nutritional assessment in adolescents of biochemical processes. Consequently, the effect of the
with Down syndrome.63,64 syndrome on the nervous system and intellectual ability
might be ameliorated.
Dietary supplementation studies Although several studies involving dietary sup
Vitamins, minerals, and antioxidants from the diet are plements have reported improvements in biochemical
important cofactors in many biochemical processes markers, no study to date has been able to translate
www.thelancet.com/child-adolescent Vol 4 June 2020 459
Review
Study design Age Country Intervention Daily* intervention Measurements Results
duration
Before intervention After intervention
Stagi et al Controlled 4–19 years Italy 6 months 10 µg oral cholecalciferol Plasma 25(OH) D levels, Significantly lower 25(OH) Increased plasma 25(OH) D
(2015)53 intervention (November to serum calcium and D levels in Down syndrome levels in Down syndrome
study (Down May) phosphate, bone specific group than in control (but not control) group, but
syndrome alkaline phosphate, and group; 14 (45%) children still significantly lower than
group n=31 and parathyroid hormone; in Down syndrome group control group; 8 (29%)
control group evaluation of dietary had deficient (<20 ng/mL) children in Down syndrome
n=99) vitamin D intake by 25(OH) D levels and 10 group had deficient 25(OH)
interview with parents on (32%) had severe D levels and 7 (22%) had
use of vitamin D fortified deficiency (≤10 ng/mL); severe deficiency;
milk higher parathyroid parathyroid hormone levels
hormone levels in Down still higher in Down
syndrome group than in syndrome group than in
control group; less control group
vitamin D fortified milk
consumed by Down
syndrome group than by
control group
Reza et al Four-arm 7–12 years Iran 4 months Group A: exercise (45 min Bone mineral density at Approximately 430 mg Significantly higher bone
(2013)65 randomised weight-bearing activities right proximal femur neck per day dietary calcium mineral density in all groups;
controlled trial three times per week) and by dual-energy x-ray intake in all groups; similar combined exercise and
(Down calcium (daily intake of absorptiometry physical activity pattern in calcium group: 14·6%
syndrome 500 mL of cow’s milk all groups increase; exercise group:
group n=48) enriched with vitamin D 8·6% increase; calcium
containing 200 mg calcium group: 3·5% increase; no
per serving); group B: intervention: 1·3% increase
calcium; group C: exercise;
group D: no intervention
Parisotto Case-control 3–14 years Brazil 6 months in 400 mg vitamin E and Antioxidant enzymatic ·· Significant differences in
et al study (Down Down 500 mg ascorbic acid activity from whole blood, antioxidant enzymatic
(2014)66 syndrome syndrome haemolysates, and in activity between Down
group n=21 and group only serum samples syndrome and control group;
control group more normalised antioxidant
n=18) enzymatic activity values in
Down syndrome group;
increased vitamin E levels in
whole blood of Down
syndrome group
Lakshmi Case-control 5–16 years India 6 months in 1 mg/kg bodyweight zinc, Serum Lower acetylcholinesterase Increased and more
et al study (Down Down 1·5 mg vitamin A, 17 mg acetylcholinesterase and and butyrylcholinesterase normalised values of
(2008)67 syndrome syndrome vitamin E, 100 mg ascorbic butyrylcholinesterase values in Down syndrome acetylcholinesterase and
group n=40 group only acid, 10 mg thiamine, 10 mg group than in control butyrylcholinesterase in
and control riboflavin, 3 mg pyroxidine, group Down syndrome group than
group n=40) 5 µg cyanocobalamin, 50 mg in control group
nicotinic acid, 1 mg folic
acid, 12·5 mg calcium
pantothenate, 2·5 mg
copper, 60 µg selenium,
1·4 mg manganese, and 5 µg
chromium
Ellis et al Four-arm 0–7 UK 18 months Group A: antioxidants Antioxidant enzymatic ·· No clinically or statistically
(2008)68 single-blinded months (10 µg selenium, 5 mg zinc, activity in red blood cells; significant outcomes
randomised 0·9 mg vitamin A, 100 mg lipid peroxidation
controlled trial vitamin E, and 50 mg biomarker in urine; clinical
(Down ascorbic acid) and 0·1 mg improvements by
syndrome folic acid (n=41); group B: quotient on Griffiths
group n=156) antioxidants (n=40); mental developmental
group C: 0·1 mg folic acid scale and MacArthur
(n=36); group D: placebo communicative
(n=39) development inventory
(Table 2 continues on next page)
these findings into improvements in clinical outcomes any description of clinical outcome measures. The
(table 2). An important limitation of research is that randomised controlled trial by Ellis and colleagues68 had
most studies include small samples and do not include a stricter study design than most Down syndrome
460 www.thelancet.com/child-adolescent Vol 4 June 2020
Review
Study design Age Country Intervention Daily* intervention Measurements Results
duration
Before intervention After intervention
(Continued from previous page)
Nachvak Three-arm 7–15 years Iran 4 months in Group A: 268 mg d-alpha Serum thiobarbituric acid ·· Higher levels of oxidative
et al randomised Down tocopherol; group B: 100 mg reactive substances and stress markers in Down
(2014)69 controlled trial syndrome thioctic acid; group C: urinary 8-hydroxy-2- syndrome group than in
(Down group only placebo deoxyguanosine oxidative sibling control group; no
syndrome stress markers change in thiobarbituric acid
group n=93 and reactive substances after any
sibling control intervention in all groups;
group n=26) significantly lower urinary
8-hydroxy-2-
deoxyguanosine in d-alpha
tocopherol group than in
placebo group
Marreiro Uncontrolled 10–19 Brazil 4 weeks 30 mg zinc Measures of zinc-related ·· Increased zinc concentration
et al intervention years nutritional status in in plasma and decreased
(2009)70 study (Down plasma and erythrocytes; concentration in
syndrome serum concentration of erythrocytes; no difference in
group n=16) thyroid hormones serum thyroid hormone
(thyroxine and concentration
tri-iodothyronine)
Gualandri Uncontrolled 1–14 years Italy 30 days in 200 mg thioctic acid and Thiol groups, septic ·· 13 children withdrew so
et al intervention children with 200 mg cysteine reactive oxygen species, results based on
(2003)71 study (Down compromised and total antioxidant 20 participants; significant
syndrome redox balance status in serum increase in serum thiol
group n=33) at baseline groups and antioxidant
capacity in serum; significant
decrease in serum total and
septic reactive oxygen
species
*Unless otherwise indicated.
Table 2: Dietary intervention studies in children with Down syndrome
studies to date and included a relatively large sample of the USA, 49% reported that they gave or had given
156 infants with Down syndrome with a mean age of supplements to their child, with antioxidants and
4 months at enrolment. The researchers investigated vitamins being the most popular supplement
the effect of antioxidants and folic acid supplementation categories.62 On average, the children used three
and did not find any improvements on oxidative stress, supplements (range 1–18). 87% of these parents reported
which was biochemically measured, or cognitive improve ments in language, immunity, and attention.
functions, which were measured by the development of This finding shows a discrepancy between scientific
major motor milestones and language development literature and opinions of the parents that needs to be
(table 2).68 Furthermore, a systematic review from 2002 systematically addressed.
by Michael Salman74 did not find evidence that cognitive
function or psychomotor development were affected by Dietary issues related to coeliac disease and
any combination of supplement with vitamins or type 1 diabetes
minerals. We did not identify any studies on the safety As previously mentioned, children with Down syndrome
of dietary supplements, which is a concern because have an increased risk of coeliac disease8 and type 1
some of the doses that have been used in diabetes.12 The only available treatment for coeliac disease
supplementation studies have been high (table 2). is a gluten-free diet (figure). In a small study of nine people
Gastrointestinal distress has been reported as a side- (aged 12–50 years) with Down syndrome who were
effect of dietary sup plementation.62,68 No association diagnosed with coeliac disease, clinical improvements in
between the use of vitamin supplements and the risk of anaemia and diarrhoea and improved, less irritable
leukaemia has been found in children with Down behaviour were observed at 1 year of follow-up in
syndrome.75 participants who had good diet compliance.76 Apart from
Despite minimal evidence of the effect of various this observation, we did not identify any other studies that
dietary supplementations, their use remains common in described aspects related to diet or determinants of diet
children with Down syndrome. In a survey of compliance in children with both Down syndrome and
1167 parents with a child with Down syndrome from coeliac disease or type 1 diabetes.
www.thelancet.com/child-adolescent Vol 4 June 2020 461
Review
above. This concern calls for early prevention to avoid
Search strategy and selection criteria later comorbidities. The switch between preventing the
We searched Ovid MEDLINE for articles using the following risk of undernutrition in the child’s first year of life and
search terms “Down syndrome” AND (“nutrition” OR obesity in later life is a challenge to treatment. Clearly, a
“nutritional” OR “feeding” OR “diet” OR “dietary”). We limited need exists for more research on nutritional aspects in
our search to articles published in English from Jan 1, 2000, to the prevention and treatment of obesity in Down
Aug 19, 2019. We considered this period relevant for health- syndrome.
care practice because of the increased survival rate of children Contributors
with Down syndrome who are born with congenital MN did the literature search, identified relevant articles, read included
studies, drafted, and finalised the Review and tables. MN also made
malformations and improvements in medical and nutritional the figures and participated in discussions and revision of the Review.
treatment. Our search identified 351 articles. We assessed SH contributed to the planning of the first draft of the manuscript
titles and abstracts for studies in children and adolescents with clinical cases and relevant pathology linked to nutrition and
with Down syndrome. We included original studies that used commented on the Review. KR contributed to the planning of the
literature search, the use of selection criteria, and the first draft of
various descriptive and intervention designs and the most the Review with clinical examples and relevant pathology linked to
recent review articles that were nutritionally relevant. We nutrition. KR also contributed to finalising and revising the Review.
excluded case reports, adult population studies, and studies SOK contributed to the planning of the literature search, the use of
in animal models. Additionally, guidelines for health selection criteria, and did the literature search. SOK also contributed
to the outline of the Review, preliminary drafting and finalising of
supervision in children with Down syndrome were assessed the manuscript, and participated in discussions and revision of
and included. We identified 57 articles that matched our the Review.
criteria. We did a supplementary search for the identification Declaration of interests
of diagnosis-specific growth curves. All authors declare no competing interests.
References
1 Loane M, Morris JK, Addor MC, et al. Twenty-year trends in the
Limitations and future perspectives prevalence of Down syndrome and other trisomies in Europe:
impact of maternal age and prenatal screening. Eur J Hum Genet
Little research has been done on the nutritional 2013; 21: 27–33.
challenges in children and adolescents with Down 2 de Graaf G, Buckley F, Dever J, Skotko BG. Estimation of live birth
syndrome, with few published intervention studies. and population prevalence of Down syndrome in nine U.S. states.
Several studies include small numbers of participants Am J Med Genet A 2017; 173: 2710–19.
3 Ostermaier KK. Down syndrome: clinical features and diagnosis.
with wide age distributions and inadequate descriptions 2019. https://www.uptodate.com/contents/down-syndrome-clinical-
of health status. Additionally, many studies include features-and-diagnosis (accessed Aug 13, 2019).
cohorts that were followed up at specialist clinics 4 Freeman SB, Bean LH, Allen EG, et al. Ethnicity, sex, and the
incidence of congenital heart defects: a report from the National
and could, therefore, be selective populations. More Down Syndrome Project. Genet Med 2008; 10: 173–80.
in-depth studies with representative samples and 5 Ergaz-Shaltiel Z, Engel O, Erlichman I, Naveh Y, Schimmel MS,
controlled study designs are needed that use cutting- Tenenbaum A. Neonatal characteristics and perinatal complications
in neonates with Down syndrome. Am J Med Genet A 2017;
edge methods and technologies. This Review shows that 173: 1279–86.
an urgent need exists for studies that address energy 6 Mircher C, Toulas J, Cieuta-Walti C, et al. Anthropometric charts
requirements and nutritional intakes and status that and congenital anomalies in newborns with Down syndrome.
Am J Med Genet A 2017; 173: 2166–75.
should be the basis for the development of targeted,
7 Weijerman ME, van Furth AM, Vonk Noordegraaf A,
randomised clinical interventions. Knowledge on van Wouwe JP, Broers CJ, Gemke RJ. Prevalence, neonatal
relevant health issues in Down syndrome in general, characteristics, and first-year mortality of Down syndrome:
and nutritional issues in this patient group in particular, a national study. J Pediatr 2008; 152: 15–19.
8 Du Y, Shan LF, Cao ZZ, Feng JC, Cheng Y. Prevalence of celiac
is needed for such studies to be of high quality and disease in patients with Down syndrome: a meta-analysis.
relevance for doctors and clinical dietitians who work Oncotarget 2018; 9: 5387–96.
with this group. 9 Faulks D, Collado V, Mazille MN, Veyrune JL, Hennequin M.
Masticatory dysfunction in persons with Down’s syndrome.
Part 1: aetiology and incidence. J Oral Rehabil 2008; 35: 854–62.
Conclusions 10 Pierce MJ, LaFranchi SH, Pinter JD. Characterization of thyroid
Increased focus on nutritional measures is important abnormalities in a large cohort of children with Down syndrome.
Horm Res Paediatr 2017; 87: 170–78.
for the health and wellbeing of children and adolescents
11 Gillespie KM, Dix RJ, Williams AJ, et al. Islet autoimmunity in
with Down syndrome. Specific clinical features of Down children with Down’s syndrome. Diabetes 2006; 55: 3185–88.
syndrome have nutritional relevance and need to be 12 Bergholdt R, Eising S, Nerup J, Pociot F. Increased prevalence of
addressed systematically. There are different nutritional Down’s syndrome in individuals with type 1 diabetes in Denmark:
a nationwide population-based study. Diabetologia 2006;
implications in various age groups, with feeding 49: 1179–82.
problems predominant in the first years of life. Clinical 13 Bull MJ, Committee on Genetics. Health supervision for children
screening for feeding problems and evaluation of with Down syndrome. Pediatrics 2011; 128: 393–406.
children with feeding difficulties and low weight gain is 14 Anil MA, Shabnam S, Narayanan S. Feeding and swallowing
difficulties in children with Down syndrome. J Intellect Disabil Res
important. Excessive weight gain is a concern for many 2019; 63: 992–1014.
children with Down syndrome aged 4–5 years and
462 www.thelancet.com/child-adolescent Vol 4 June 2020
Review
15 Bertapelli F, Pitetti K, Agiovlasitis S, Guerra-Junior G. Overweight 39 Polfuss M, Simpson P, Neff Greenley R, Zhang L, Sawin KJ.
and obesity in children and adolescents with Down Parental feeding behaviors and weight-related concerns in children
syndrome–prevalence, determinants, consequences, and with special needs. West J Nurs Res 2017; 39: 1070–93.
interventions: a literature review. Res Dev Disabil 2016; 57: 181–92. 40 Zemel BS, Pipan M, Stallings VA, et al. Growth charts for children
16 Englund A, Jonsson B, Zander CS, Gustafsson J, Anneren G. with Down syndrome in the United States. Pediatrics 2015;
Changes in mortality and causes of death in the Swedish Down 136: e1204–11.
syndrome population. Am J Med Genet A 2013; 161A: 642–49. 41 Mircher C, Briceno LG, Toulas J, et al. Growth curves for French
17 Nordstrom M, Hansen BH, Paus B, Kolset SO. Accelerometer- people with Down syndrome from birth to 20 years of age.
determined physical activity and walking capacity in persons with Am J Med Genet A 2018; 176: 2685–94.
Down syndrome, Williams syndrome and Prader-Willi syndrome. 42 Tuysuz B, Goknar NT, Ozturk B. Growth charts of Turkish children
Res Dev Disabil 2013; 34: 4395–403. with Down syndrome. Am J Med Genet A 2012; 158A: 2656–64.
18 Pisacane A, Toscano E, Pirri I, et al. Down syndrome and 43 Van Gameren-Oosterom HB, Van Dommelen P,
breastfeeding. Acta Paediatr 2003; 92: 1479–81. Oudesluys-Murphy AM, Buitendijk SE, Van Buuren S,
19 Flores-Lujano J, Perez-Saldivar ML, Fuentes-Panana EM, et al. Van Wouwe JP. Healthy growth in children with Down syndrome.
Breastfeeding and early infection in the aetiology of childhood PLoS One 2012; 7: e31079.
leukaemia in Down syndrome. Br J Cancer 2009; 101: 860–64. 44 Su X, Lau JT, Yu CM, et al. Growth charts for Chinese Down
20 Al-Sarheed M. Feeding habits of children with Down’s syndrome syndrome children from birth to 14 years. Arch Dis Child 2014;
living in Riyadh, Saudi Arabia. J Trop Pediatr 2006; 52: 83–86. 99: 824–29.
21 Lewis E, Kritzinger A. Parental experiences of feeding problems in 45 Bertapelli F, Machado MR, Roso RD, Guerra-Junior G. Body mass
their infants with Down syndrome. Downs Syndr Res Pract 2004; index reference charts for individuals with Down syndrome aged
9: 45–52. 2–18 years. J Pediatr (Rio J) 2017; 93: 94–99.
22 Cullen EG. Breastfeeding and Down syndrome: a comprehensive 46 Styles ME, Cole TJ, Dennis J, Preece MA. New cross sectional stature,
guide for mothers and medical professionals. Hanover, MA: weight, and head circumference references for Down’s syndrome in
Julia’s Way, 2019. the UK and Republic of Ireland. Arch Dis Child 2002; 87: 104–08.
23 King G, Williams L, Hahn Goldberg S. Family-oriented services in 47 Sica CD, Cesa CC, Pellanda LC. Growth curves in Down syndrome
pediatric rehabilitation: a scoping review and framework to with congenital heart disease. Rev Assoc Med Bras (1992) 2016;
promote parent and family wellness. Child Care Health Dev 2017; 62: 414–20.
43: 334–47. 48 Samur San-Matin JE, Goncalves EM, Bertapelli F, Mendes RT,
24 Stanley MA, Shepherd N, Duvall N, et al. Clinical identification of Guerra-Junior G. Body mass index cutoff point estimation as
feeding and swallowing disorders in 0–6 month old infants with obesity diagnostic criteria in Down syndrome adolescents.
Down syndrome. Am J Med Genet A 2019; 179: 177–82. Nutr Hosp 2016; 33: 571.
25 Jackson A, Maybee J, Moran MK, Wolter-Warmerdam K, Hickey F. 49 Wendel D, Weber D, Leonard MB, et al. Body composition
Clinical characteristics of dysphagia in children with Down estimation using skinfolds in children with and without health
syndrome. Dysphagia 2016; 31: 663–71. conditions affecting growth and body composition. Ann Hum Biol
26 Genova L, Cerda J, Correa C, Vergara N, Lizama M. Good health 2017; 44: 108–20.
indicators in children with Down syndrome: high frequency of 50 Goncalves Machado A, Lummertz Magenis M, Bongiolo AM,
exclusive breastfeeding at 6 months. Rev Chil Pediatr 2018; Castro K, da Silva MA, Schweigert Perry ID. Bioelectrical
89: 32–41. impedance analysis: body composition in children and adolescents
27 Mackman CA, Loomba RS, Slicker J, Bartz PJ. Growth trajectory in with Down syndrome. Minerva Pediatr 2017; 69: 560–63.
children with trisomy 21 with and without atrioventricular septal 51 Tenenbaum A, Malkiel S, Wexler ID, Levy-Khademi F, Revel-Vilk S,
defect. Congenit Heart Dis 2016; 11: 348–53. Stepensky P. Anemia in children with Down syndrome.
28 O’Neill AC, Richter GT. Pharyngeal dysphagia in children with Int J Pediatr 2011; 2011: 813541.
Down syndrome. Otolaryngol Head Neck Surg 2013; 149: 146–50. 52 Hart SJ, Zimmerman K, Linardic CM, et al. Detection of iron
29 Jackson A, Maybee J, Wolter-Warmerdam K, DeBoer E, Hickey F. deficiency in children with Down syndrome. Genet Med 2019;
Associations between age, respiratory comorbidities, and dysphagia published online Nov 12. DOI:10.1038/s41436-019-0699-3.
in infants with Down syndrome. Pediatr Pulmonol 2019; 53 Stagi S, Lapi E, Romano S, et al. Determinants of vitamin D levels
54: 1853–59. in children and adolescents with Down syndrome. Int J Endocrinol
30 Frank K, Esbensen AJ. Fine motor and self-care milestones for 2015; 2015: 896758.
individuals with Down syndrome using a retrospective chart review. 54 Polfuss M, Sawin KJ, Papanek PE, et al. Total energy expenditure
J Intellect Disabil Res 2015; 59: 719–29. and body composition of children with developmental disabilities.
31 Ross CF, Bernhard CB, Smith-Simpson S. Parent-reported ease of Disabil Health J 2018; 11: 442–46.
eating foods of different textures in young children with Down 55 Magenis ML, Machado AG, Bongiolo AM, Silva MAD, Castro K,
syndrome. J Texture Stud 2019; 50: 426–33. Perry IDS. Dietary practices of children and adolescents with Down
32 Oliveira AC, Paiva SM, Martins MT, Torres CS, Pordeus IA. syndrome. J Intellect Disabil 2018; 22: 125–34.
Prevalence and determinant factors of malocclusion in children 56 Samarkandy MM, Mohamed BA, Al-Hamdan AA. Nutritional
with special needs. Eur J Orthod 2011; 33: 413–18. assessment and obesity in Down syndrome children and their
33 Bell EJ, Kaidonis J, Townsend GC. Tooth wear in children with siblings in Saudi Arabia. Saudi Med J 2012; 33: 1216–21.
Down syndrome. Aust Dent J 2002; 47: 30–35. 57 Jankowicz-Szymanska A, Mikolajczyk E, Wojtanowski W. The effect
34 Oliveira AC, Pordeus IA, Torres CS, Martins MT, Paiva SM. of the degree of disability on nutritional status and flat feet in
Feeding and nonnutritive sucking habits and prevalence of open adolescents with Down syndrome. Res Dev Disabil 2013; 34: 3686–90.
bite and crossbite in children/adolescents with Down syndrome. 58 Jobling A, Cuskelly M. Young people with Down syndrome:
Angle Orthod 2010; 80: 748–53. a preliminary investigation of health knowledge and associated
35 Faulks D, Mazille MN, Collado V, Veyrune JL, Hennequin M. behaviours. J Intellect Dev Disabil 2006; 31: 210–18.
Masticatory dysfunction in persons with Down’s syndrome. 59 Hinckson EA, Dickinson A, Water T, Sands M, Penman L.
Part 2: management. J Oral Rehabil 2008; 35: 863–69. Physical activity, dietary habits and overall health in overweight and
36 Osaili TM, Attlee A, Naveed H, et al. Physical status and parent- obese children and youth with intellectual disability or autism.
child feeding behaviours in children and adolescents with Down Res Dev Disabil 2013; 34: 1170–78.
syndrome in the United Arab Emirates. 60 Curtin C, Bandini LG, Must A, et al. Parent support improves
Int J Environ Res Public Health 2019; 16: 2264. weight loss in adolescents and young adults with Down syndrome.
37 van Dijk M, Lipke-Steenbeek W. Measuring feeding difficulties in J Pediatr 2013; 163: 1402–08.
toddlers with Down syndrome. Appetite 2018; 126: 61–65. 61 Grammatikopoulou MG, Manai A, Tsigga M,
38 O’Neill KL, Shults J, Stallings VA, Stettler N. Child-feeding Tsiligiroglou-Fachantidou A, Galli-Tsinopoulou A, Zakas A. Nutrient
practices in children with Down syndrome and their siblings. intake and anthropometry in children and adolescents with Down
J Pediatr 2005; 146: 234–38. syndrome–a preliminary study. Dev Neurorehabil 2008; 11: 260–67.
www.thelancet.com/child-adolescent Vol 4 June 2020 463
Review
62 Lewanda AF, Gallegos MF, Summar M. Patterns of dietary 71 Gualandri W, Gualandri L, Demartini G, et al. Redox balance in
supplement use in children with Down syndrome. J Pediatr 2018; patients with Down’s syndrome before and after dietary
201: 100–05. supplementation with alpha-lipoic acid and L-cysteine.
63 Bathgate KE, Sherriff JL, Leonard H, et al. Feasibility of assessing Int J Clin Pharmacol Res 2003; 23: 23–30.
diet with a mobile food record for adolescents and young adults 72 Lima AS, Cardoso BR, Cozzolino SF. Nutritional status of zinc in
with Down syndrome. Nutrients 2017; 9: 273. children with Down syndrome. Biol Trace Elem Res 2010; 133: 20–28.
64 Polfuss M, Moosreiner A, Boushey CJ, Delp EJ, Zhu F. Technology- 73 Marques RC, de Sousa AF, do Monte SJ, Oliveira FE,
based dietary assessment in youth with and without developmental do Nascimento Nogueira N, Marreiro DN. Zinc nutritional status in
disabilities. Nutrients 2018; 10: 1482. adolescents with Down syndrome. Biol Trace Elem Res 2007;
65 Reza SM, Rasool H, Mansour S, Abdollah H. Effects of calcium and 120: 11–18.
training on the development of bone density in children with Down 74 Salman M. Systematic review of the effect of therapeutic dietary
syndrome. Res Dev Disabil 2013; 34: 4304–09. supplements and drugs on cognitive function in subjects with
66 Parisotto EB, Garlet TR, Cavalli VL, et al. Antioxidant intervention Down syndrome. Eur J Paediatr Neurol 2002; 6: 213–19.
attenuates oxidative stress in children and teenagers with Down 75 Blair CK, Roesler M, Xie Y, et al. Vitamin supplement use among
syndrome. Res Dev Disabil 2014; 35: 1228–36. children with Down’s syndrome and risk of leukaemia: a Children’s
67 Lakshmi KT, Surekha RH, Srikanth B, Jyothy A. Serum Oncology Group (COG) study. Paediatr Perinat Epidemiol 2008;
cholinesterases in Down synrome children before and after 22: 288–95.
nutritional supplementation. Singapore Med J 2008; 49: 561–64. 76 Nisihara RM, Bonacin M, da Silva Kotze LM, de Oliveira NP,
68 Ellis JM, Tan HK, Gilbert RE, et al. Supplementation with Utiyama S. Monitoring gluten-free diet in coeliac patients with
antioxidants and folinic acid for children with Down’s syndrome: Down’s syndrome. J Hum Nutr Diet 2014; 27 (suppl 2): 1–3.
randomised controlled trial. BMJ 2008; 336: 594–97.
69 Nachvak SM, Neyestani RT, Mahboob AS, Sabour S, Keshawarz AS, © 2020 Elsevier Ltd. All rights reserved.
Speakman JR. α-Tocopherol supplementation reduces biomarkers
of oxidative stress in children with Down syndrome: a randomized
controlled trial. Eur J Clin Nutr 2014; 68: 1119–23.
70 Marreiro D do N, de Sousa AF, Nogueira N do N, Oliveira FE.
Effect of zinc supplementation on thyroid hormone metabolism of
adolescents with Down syndrome. Biol Trace Elem Res 2009;
129: 20–27.
464 www.thelancet.com/child-adolescent Vol 4 June 2020
You might also like
- Euthanasia Examined Ethical Clinical and Legal PerspectivesDocument357 pagesEuthanasia Examined Ethical Clinical and Legal PerspectivesFelipe TauferNo ratings yet
- Lengo Savings Plan PremierDocument9 pagesLengo Savings Plan PremierPado DjochieNo ratings yet
- List of The PhobiaDocument8 pagesList of The PhobiaRjvm Net Ca FeNo ratings yet
- Down Syndrome Associated ComplicationsDocument3 pagesDown Syndrome Associated ComplicationsAlyssa Jean AlcoranNo ratings yet
- BF03327743 2Document6 pagesBF03327743 2Mohammad shaabanNo ratings yet
- Seizure Disorders: School-Age Children and Adolescents 609Document30 pagesSeizure Disorders: School-Age Children and Adolescents 609Fahri GunawanNo ratings yet
- Feeding Problems Including Avoidant Restrictive Food Intake Disorder in Young Children With Autism Spectrum Disorder in A Multiethnic PopulationDocument12 pagesFeeding Problems Including Avoidant Restrictive Food Intake Disorder in Young Children With Autism Spectrum Disorder in A Multiethnic PopulationKaren MurilloNo ratings yet
- Nutritional Status of Neurologically Impaired Children - Impact On ComorbidityDocument9 pagesNutritional Status of Neurologically Impaired Children - Impact On ComorbidityEvelynNo ratings yet
- Pereira Et Al 2009 Prader Willi Syndrome A Review For Pediatric Nutrition ProfessionalsDocument6 pagesPereira Et Al 2009 Prader Willi Syndrome A Review For Pediatric Nutrition Professionalsvcnflga08No ratings yet
- 1993 - BARKER Et Al - Fetal Nutrition and Cardiovascular Disease in Adult LifeDocument4 pages1993 - BARKER Et Al - Fetal Nutrition and Cardiovascular Disease in Adult LifeSamanta MonteiroNo ratings yet
- JP 2014116Document5 pagesJP 2014116koas forensikNo ratings yet
- Estreñimiento y TeaDocument9 pagesEstreñimiento y TeaElena Martin LopezNo ratings yet
- Arfid Tea Eval y ManejoDocument7 pagesArfid Tea Eval y ManejoDalilaNo ratings yet
- Research Paper: Dietary Shortcomings in Children On A Gluten-Free DietDocument7 pagesResearch Paper: Dietary Shortcomings in Children On A Gluten-Free DietIsha GargNo ratings yet
- Gastroesophageal Reflux: Natural Evolution, Diagnostic Approach and TreatmentDocument7 pagesGastroesophageal Reflux: Natural Evolution, Diagnostic Approach and TreatmentYanis Widhiya NingrumNo ratings yet
- Lagan 2020Document16 pagesLagan 2020Aurha Akmal GinarisNo ratings yet
- Medical Management of Children With Down SyndromeDocument8 pagesMedical Management of Children With Down SyndromeMariana OrozcoNo ratings yet
- Feedingandeating Disordersinchildren: Rachel Bryant-WaughDocument11 pagesFeedingandeating Disordersinchildren: Rachel Bryant-WaughValeria PNo ratings yet
- Childhood Obesity SMJ-62-167Document6 pagesChildhood Obesity SMJ-62-167abNo ratings yet
- Eating Disorders in Adolescents With Chronic Gastrointestinal PDFDocument9 pagesEating Disorders in Adolescents With Chronic Gastrointestinal PDFJúlia PriyaNo ratings yet
- Rehabilitation in Down Syndrome Patient With Malnutrition, Sensory Processing Disorder, Obstructive Sleep Apnea: A Case ReportDocument6 pagesRehabilitation in Down Syndrome Patient With Malnutrition, Sensory Processing Disorder, Obstructive Sleep Apnea: A Case Reportmelda lamtiurNo ratings yet
- Down Syndrome Scott DunlopDocument3 pagesDown Syndrome Scott DunlopYwagar YwagarNo ratings yet
- Naskah Publikasi-204Document8 pagesNaskah Publikasi-204Achmad YunusNo ratings yet
- Modulo 03 CONTROL DE LECTURADocument10 pagesModulo 03 CONTROL DE LECTURAGloria Morales BastiasNo ratings yet
- dt1 BioquimicosDocument10 pagesdt1 Bioquimicosmajoydan113001No ratings yet
- Consequences of Childhood Obesity: CommentaryDocument7 pagesConsequences of Childhood Obesity: CommentaryNil NilNo ratings yet
- Prevalence and Characteristics of Avoidant/ Restrictive Food Intake Disorder in A Cohort of Young Patients in Day Treatment For Eating DisordersDocument8 pagesPrevalence and Characteristics of Avoidant/ Restrictive Food Intake Disorder in A Cohort of Young Patients in Day Treatment For Eating DisordersAhmad Tri Anggara SasmitaNo ratings yet
- 6 Nutrisi LBNDocument7 pages6 Nutrisi LBNRizalMarubobSilalahiNo ratings yet
- Cal Kins 2011Document19 pagesCal Kins 2011Dara Dasawulansari SyamsuriNo ratings yet
- Reading Lactante 20Document7 pagesReading Lactante 20ANDREA CARDENAS RODRIGUEZNo ratings yet
- A Rodriguez, 2008Document8 pagesA Rodriguez, 2008Anibal LeNo ratings yet
- Infant Gastroesophageal Reflux Disease Management Consensus 2024Document8 pagesInfant Gastroesophageal Reflux Disease Management Consensus 2024Dayana FajardoNo ratings yet
- FisherDocument4 pagesFisherNelson Syah HabibiNo ratings yet
- The Safety of Sedation For Overweight Obese Children in The Dental SettingDocument6 pagesThe Safety of Sedation For Overweight Obese Children in The Dental SettingMohammed LudoNo ratings yet
- Gastroesophageal Reflux Disease (GERD) in ChildrenDocument7 pagesGastroesophageal Reflux Disease (GERD) in ChildrenAndhika DNo ratings yet
- F S D G S: Eeding and Wallowing Ysfunction IN Enetic YndromesDocument11 pagesF S D G S: Eeding and Wallowing Ysfunction IN Enetic YndromespaulaNo ratings yet
- Zahra Publication 2Document2 pagesZahra Publication 2HenziweiNo ratings yet
- Mairs R Et Al 2016Document8 pagesMairs R Et Al 2016Camilla ValeNo ratings yet
- TEA - Conducta GastrointestinalDocument16 pagesTEA - Conducta GastrointestinalFlgo Cristian SepulvedaNo ratings yet
- 1 s2.0 S0140673622026125 MainDocument16 pages1 s2.0 S0140673622026125 MainCaylynn WoWNo ratings yet
- Journal KeperawatanDocument16 pagesJournal KeperawatanAmiLia CandrasariNo ratings yet
- Yajnik 2014Document11 pagesYajnik 2014Hashem Essa QatawnehNo ratings yet
- Rubio Cabezas Et Al 2014 Pediatric DiabetesDocument18 pagesRubio Cabezas Et Al 2014 Pediatric DiabetesTomi YamilNo ratings yet
- Autism Spectrum DisorderDocument1 pageAutism Spectrum Disordersarmiyati zainuddinNo ratings yet
- Down Syndrome, Turner Syndrome, and Klinefelter SyndromeDocument22 pagesDown Syndrome, Turner Syndrome, and Klinefelter SyndromeRegieta LalusuNo ratings yet
- Eating Disorders in The Adolescent PatientDocument15 pagesEating Disorders in The Adolescent PatientThaily MoralesNo ratings yet
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptWestiNo ratings yet
- Frequency of Malnutrition Among Children Under 2 Years and Its Relationship With Inadequate Breast Feeding PracticeDocument3 pagesFrequency of Malnutrition Among Children Under 2 Years and Its Relationship With Inadequate Breast Feeding PracticeAndhika SatriyaNo ratings yet
- Wa0018.Document7 pagesWa0018.mahesh shindeNo ratings yet
- Lapkas Anak (Prof Dr. Hj. Bidasari)Document74 pagesLapkas Anak (Prof Dr. Hj. Bidasari)Maral Bimanti Febrilina100% (1)
- Intra Uterine Growth RetardationDocument46 pagesIntra Uterine Growth RetardationIba Ghannam100% (1)
- Anthropometry Assessment in Children With Disease Related MalnutritionDocument10 pagesAnthropometry Assessment in Children With Disease Related Malnutritionberlian29031992No ratings yet
- Optimizing An Aversion Feeding Therapy Protocol For A Child With Foodproteininduced Enterocolitis Syndrome Fpies 2161 105X 1000287Document4 pagesOptimizing An Aversion Feeding Therapy Protocol For A Child With Foodproteininduced Enterocolitis Syndrome Fpies 2161 105X 1000287Rafia AwanNo ratings yet
- Rakel: Textbook of Family Medicine, 7th Ed.Document4 pagesRakel: Textbook of Family Medicine, 7th Ed.Nicolás Rojas MontenegroNo ratings yet
- Eating ProblemsDocument4 pagesEating ProblemsNicolás Rojas MontenegroNo ratings yet
- Eating ProblemsDocument4 pagesEating ProblemsximerodriguezcNo ratings yet
- Lectura Control 2 - Asignatura 3Document12 pagesLectura Control 2 - Asignatura 3CamilaGarridoNo ratings yet
- Revision Obesidad Infantil 2021Document16 pagesRevision Obesidad Infantil 2021yakdoc2023No ratings yet
- Medical Management of Children With Down Syndrome: Symposium: Special NeedsDocument8 pagesMedical Management of Children With Down Syndrome: Symposium: Special NeedsVijayakanth VijayakumarNo ratings yet
- Components of The Metabolic Syndrome Are Negative Predictors of WeightDocument6 pagesComponents of The Metabolic Syndrome Are Negative Predictors of WeightRaquel BoffNo ratings yet
- MantelDocument13 pagesManteljacopo pruccoliNo ratings yet
- The Children of Mothers With Eating Disorders: Priti Patel, Rebecca Wheatcroft, Rebecca J. Park, and Alan SteinDocument2 pagesThe Children of Mothers With Eating Disorders: Priti Patel, Rebecca Wheatcroft, Rebecca J. Park, and Alan SteinHafidz YahyaNo ratings yet
- English in Paediatrics 2: Textbook for Mothers, Babysitters, Nurses, and PaediatriciansFrom EverandEnglish in Paediatrics 2: Textbook for Mothers, Babysitters, Nurses, and PaediatriciansNo ratings yet
- Management of Postoperative Enterocutaneous Fi Stulae in Children A Decade Experience in A Single CentreDocument8 pagesManagement of Postoperative Enterocutaneous Fi Stulae in Children A Decade Experience in A Single CentreOctavianus KevinNo ratings yet
- 2022 Calendar One PageDocument1 page2022 Calendar One PageOctavianus KevinNo ratings yet
- PhaseAngleICU ISCBC Final NorecDocument18 pagesPhaseAngleICU ISCBC Final NorecOctavianus KevinNo ratings yet
- Nutritional ManagementDocument315 pagesNutritional ManagementOctavianus KevinNo ratings yet
- 2022 Weekly Calendar MondayDocument3 pages2022 Weekly Calendar MondayOctavianus KevinNo ratings yet
- Energey Balance and CancerDocument189 pagesEnergey Balance and CancerOctavianus KevinNo ratings yet
- What Is Subjective Global Assessment Nutritional Status?: Allan S. ADocument6 pagesWhat Is Subjective Global Assessment Nutritional Status?: Allan S. AOctavianus KevinNo ratings yet
- MIcronutrients Role in Pulmonary Disease (RESPINA 13 NOV 21)Document24 pagesMIcronutrients Role in Pulmonary Disease (RESPINA 13 NOV 21)Octavianus KevinNo ratings yet
- Fnins 14 00190Document17 pagesFnins 14 00190Octavianus KevinNo ratings yet
- Glutamin Medi 94 E1319Document12 pagesGlutamin Medi 94 E1319Octavianus KevinNo ratings yet
- Evaluation of Muscle and Fat Loss As Diagnostic Criteria For MalnutritionDocument10 pagesEvaluation of Muscle and Fat Loss As Diagnostic Criteria For MalnutritionOctavianus KevinNo ratings yet
- Epidemiologi GGKDocument10 pagesEpidemiologi GGKOctavianus KevinNo ratings yet
- When Is It Appropriate To Use Arginine in Critical Illness?Document7 pagesWhen Is It Appropriate To Use Arginine in Critical Illness?Octavianus KevinNo ratings yet
- MMF 1.0.0Document2 pagesMMF 1.0.0unconformistNo ratings yet
- Perfect Match: Application To Adopt or Foster A Cat or KittenDocument2 pagesPerfect Match: Application To Adopt or Foster A Cat or KittenChichinete MadalinaNo ratings yet
- First DraftDocument83 pagesFirst DraftNicole Cliano0% (1)
- Humiliation JoiDocument4 pagesHumiliation JoibestdumimarianNo ratings yet
- Public Health Aspects of Cream-Filled Pastries. A Review: Frankl. BryanDocument8 pagesPublic Health Aspects of Cream-Filled Pastries. A Review: Frankl. BryanChristine Joy PanlilioNo ratings yet
- LO1Clean The Bar AreasDocument27 pagesLO1Clean The Bar AreasEiszel CadacioNo ratings yet
- Detailed Lesson PlanDocument49 pagesDetailed Lesson PlanNaisy MagalonaNo ratings yet
- Periodic Table FiltersDocument2 pagesPeriodic Table Filtersecaterina8No ratings yet
- Orbino, Frances Anne N. 4th Rot FdarDocument2 pagesOrbino, Frances Anne N. 4th Rot FdarFrances OrbinoNo ratings yet
- Guidelines - Aceh and NiasDocument25 pagesGuidelines - Aceh and NiasBenny Aryanto SihalohoNo ratings yet
- Sample CFD PaperDocument7 pagesSample CFD PaperNurikNo ratings yet
- What Exactly Is Adrenal FatigueDocument3 pagesWhat Exactly Is Adrenal FatiguejhNo ratings yet
- The Effect of Hydrotherapy On Blood Pressure of DOIDocument4 pagesThe Effect of Hydrotherapy On Blood Pressure of DOIPhocachinnoNo ratings yet
- Aliphatic PDFDocument19 pagesAliphatic PDFK &WNo ratings yet
- Addiction: Digital AssessmentDocument4 pagesAddiction: Digital AssessmentNarender SirimallaNo ratings yet
- Unit-1 Some Basic Concepts of ChemistryDocument4 pagesUnit-1 Some Basic Concepts of ChemistryJleodennis RajNo ratings yet
- The Health Anxiety Inventory Development and Validation of Scales For The Measurement of Health Anxiety and HypochondriasisDocument11 pagesThe Health Anxiety Inventory Development and Validation of Scales For The Measurement of Health Anxiety and HypochondriasisJan LAWNo ratings yet
- Rooftop Fish FarmsDocument4 pagesRooftop Fish FarmsbobsraineyNo ratings yet
- Pharmacogenetics Lecture NotesDocument5 pagesPharmacogenetics Lecture NotesMark Russel Sean LealNo ratings yet
- Consumer Buying Behaviour QuestionnaireDocument4 pagesConsumer Buying Behaviour Questionnaireruchi mishraNo ratings yet
- The Structure and Function of MacromoleculesDocument70 pagesThe Structure and Function of MacromoleculesLustried Nadyang100% (1)
- Falsafah Betty NeumanDocument23 pagesFalsafah Betty NeumanmaheswariNo ratings yet
- Medical School Guidelines and Sample EssaysDocument73 pagesMedical School Guidelines and Sample EssaysJacques Diambra Odi100% (1)
- Impact of Covid 19 On EnvironmentDocument20 pagesImpact of Covid 19 On EnvironmentRamkishan JaiswarNo ratings yet
- PAMET LinkDocument8 pagesPAMET LinkkimmeyaaaaaaaahNo ratings yet
- Padampur ReportDocument16 pagesPadampur ReportSaudagar BiswalNo ratings yet
- CASP Randomised Controlled Trial Checklist 2018 - Fillable - FormDocument5 pagesCASP Randomised Controlled Trial Checklist 2018 - Fillable - FormEllieNo ratings yet