Download as pdf or txt
You might also like
- Common General Practice Consultations - Notes For OSCEsDocument54 pagesCommon General Practice Consultations - Notes For OSCEshaydenfarquhar89% (9)
- History and Physical ExamDocument5 pagesHistory and Physical ExamAnastasia TjanNo ratings yet
- Medicine History and CounsellingDocument13 pagesMedicine History and Counsellingpranjl100% (1)
- Mnemonics for Medicine: Differential Diagnoses and Other PearlsFrom EverandMnemonics for Medicine: Differential Diagnoses and Other PearlsRating: 5 out of 5 stars5/5 (3)
- The Inner Cause: A Psychology of Symptoms from A to ZFrom EverandThe Inner Cause: A Psychology of Symptoms from A to ZRating: 5 out of 5 stars5/5 (2)
- Clinical Exam NotesDocument222 pagesClinical Exam Notesakansha_bhargava_6100% (1)
- Health Assessment Long Answer QuestionsDocument11 pagesHealth Assessment Long Answer QuestionsSraddha Patel50% (2)
- TB MeningitisDocument91 pagesTB MeningitischristianNo ratings yet
- History TakingDocument19 pagesHistory TakingAlice Verran100% (1)
- Cvsassessmentby 180123144727Document29 pagesCvsassessmentby 180123144727sas100% (1)
- Cardiac Assessment FormatDocument20 pagesCardiac Assessment FormatSalman Habeeb75% (4)
- Diagnosis & Evaluation of Respiratory DiseaseDocument99 pagesDiagnosis & Evaluation of Respiratory DiseaseAmalia Intan PermataNo ratings yet
- CVS - Case Sheet - FinalDocument8 pagesCVS - Case Sheet - FinalBunnyNo ratings yet
- Soap 2Document5 pagesSoap 2api-456313554No ratings yet
- Case No. 2:: Chief ComplaintDocument10 pagesCase No. 2:: Chief ComplaintJayson TrajanoNo ratings yet
- Clinical Exam NotesDocument222 pagesClinical Exam NotesNarcis PopaNo ratings yet
- Red Flags For The MRCGPDocument3 pagesRed Flags For The MRCGPUsm LeeNo ratings yet
- Common General Practice Consultations Notes For OSCEsDocument52 pagesCommon General Practice Consultations Notes For OSCEsNadia SalwaniNo ratings yet
- Dela Torre Case Presentation South GenDocument44 pagesDela Torre Case Presentation South GenRalph Dale Dela TorreNo ratings yet
- Pediatric Cardiovascular System History & ExaminationDocument74 pagesPediatric Cardiovascular System History & Examinationعبدالله Abdullah INo ratings yet
- NCLEX Study InformationDocument14 pagesNCLEX Study Informationrustiejade100% (4)
- Case Report 1 SALGADO Israel Written ReportDocument4 pagesCase Report 1 SALGADO Israel Written ReportISRAEL JULIANO SALGADONo ratings yet
- Taking History & Methods of Physical Examination For: Koray TopgülDocument38 pagesTaking History & Methods of Physical Examination For: Koray Topgülayadalshawki7100% (1)
- Case-1 On Open CholeDocument4 pagesCase-1 On Open CholeKhus RahoNo ratings yet
- SCHEME of The PEDIATRICS' CASE HISTORYDocument17 pagesSCHEME of The PEDIATRICS' CASE HISTORYManusheeNo ratings yet
- Soap Note TemplateDocument4 pagesSoap Note TemplateAdamNo ratings yet
- History and Examinatoin of The Cardiovascular SystemDocument47 pagesHistory and Examinatoin of The Cardiovascular Systemmawada abdallaNo ratings yet
- History Taking: Presenting Complaint: They Let Us Know About The DurationDocument10 pagesHistory Taking: Presenting Complaint: They Let Us Know About The DurationamsirakNo ratings yet
- Lecture 11 History TakingDocument6 pagesLecture 11 History Takingpxb8dhqgs9No ratings yet
- Did It Relieve The SymptomsDocument7 pagesDid It Relieve The SymptomsZeu JoNo ratings yet
- Common General Practice Consultations - Notes For OSCEsDocument53 pagesCommon General Practice Consultations - Notes For OSCEsChanel ClarkNo ratings yet
- CVS Case ProformaDocument2 pagesCVS Case ProformaRiyaSingh100% (1)
- History SURGERYDocument23 pagesHistory SURGERYmahmoud alhelalNo ratings yet
- 515Document972 pages515solecitodelmarazul100% (6)
- The Case History Scheme: Kyiv State Hospital Pediatric Department 1Document8 pagesThe Case History Scheme: Kyiv State Hospital Pediatric Department 1Fatemeh BemanaNo ratings yet
- Type The Document Title: Department of Surgery Case Report-IiDocument10 pagesType The Document Title: Department of Surgery Case Report-IiEyosiyas AbiyNo ratings yet
- Pediatric Clinical ExaminationDocument37 pagesPediatric Clinical ExaminationHalema Al OkshNo ratings yet
- 2 5404863613531850140 PDFDocument51 pages2 5404863613531850140 PDFzaid auglaNo ratings yet
- DR - Mary JohnPROTOCOL EXAMINATION-2Document9 pagesDR - Mary JohnPROTOCOL EXAMINATION-2Ria MasihNo ratings yet
- Chronic Rheumatic Valvular DiseaseDocument60 pagesChronic Rheumatic Valvular DiseaseReja AkramNo ratings yet
- HHD 9 Accident EmergencyDocument6 pagesHHD 9 Accident Emergencymusy9999No ratings yet
- Rheumatic Heart Disease With Mitral StenosisDocument28 pagesRheumatic Heart Disease With Mitral StenosiscitidotnetNo ratings yet
- HIVCase Report II Internal MedicineDocument12 pagesHIVCase Report II Internal Medicineaxmedfare138No ratings yet
- OSCE Medicine by DR BilanDocument77 pagesOSCE Medicine by DR BilanBukhaari MohamedNo ratings yet
- Examination of HydroceleDocument6 pagesExamination of HydroceleManas RanjanNo ratings yet
- Bedside OutputDocument5 pagesBedside OutputREGENE KRIS SIMMONE GAMILNo ratings yet
- Pediatrics Case PresentationDocument11 pagesPediatrics Case PresentationAishwarya Bharath0% (1)
- Internal MedicineDocument18 pagesInternal MedicineNashaat H. AlshawabkehNo ratings yet
- Enterobiasis CaseDocument4 pagesEnterobiasis CaseKimm Delos ReyesNo ratings yet
- Clinical Examination - Eric Sarpong-NtiamoahDocument52 pagesClinical Examination - Eric Sarpong-NtiamoahFathimathNo ratings yet
- CPC-Patho Version 6Document20 pagesCPC-Patho Version 6Bea SamonteNo ratings yet
- Reference Card For Who Emergency Unit Form GeneralDocument2 pagesReference Card For Who Emergency Unit Form GeneralGideon BahuleNo ratings yet
- CVS PDFDocument102 pagesCVS PDFmalik003No ratings yet
- History Taking & ExaminationDocument14 pagesHistory Taking & ExaminationMark AdrianNo ratings yet
- MS ReviewerDocument158 pagesMS ReviewerDexan Juridico100% (2)
- Cardiovascular Assessment: Assessment Uses of CVS AssessmentDocument8 pagesCardiovascular Assessment: Assessment Uses of CVS AssessmentKawaljit KaurNo ratings yet
- I. General DataDocument16 pagesI. General DataJaymart BieNo ratings yet
- Sabaneyev Sonata For Violin, Cello, and Piano, Op. 20Document71 pagesSabaneyev Sonata For Violin, Cello, and Piano, Op. 20Meow MeowNo ratings yet
- Digestion Fill-In NotesDocument1 pageDigestion Fill-In Notesapi-296488161No ratings yet
- Resume TemplateDocument13 pagesResume Templateuday_khandavilliNo ratings yet
- GEO289 Assignment 3Document4 pagesGEO289 Assignment 3Mabuti Jerald CNo ratings yet
- Elena Rodriguez Reflective EssayDocument1 pageElena Rodriguez Reflective EssayElena Rodriguez ZuletaNo ratings yet
- Immunology Spe Dual Marker: 10553470 Mrs - Ananya MishraDocument3 pagesImmunology Spe Dual Marker: 10553470 Mrs - Ananya MishraÑîrañjañ JhåNo ratings yet
- Online Entrance Test Instructions For CandidatesDocument20 pagesOnline Entrance Test Instructions For Candidatesshamimshafeb2005No ratings yet
- Kami Export - SCOPE The Necklace PlayDocument4 pagesKami Export - SCOPE The Necklace Playava riciglianoNo ratings yet
- Bio Ia 2Document8 pagesBio Ia 2juju FrancoisNo ratings yet
- 4500MB - CH 2 - Parr - Stirred Reactors and Pressure Vessels Catalog v15 Literature PDFDocument45 pages4500MB - CH 2 - Parr - Stirred Reactors and Pressure Vessels Catalog v15 Literature PDFglaubersgNo ratings yet
- High Yield Topics MCATDocument5 pagesHigh Yield Topics MCATkarijaniNo ratings yet
- Alkaloid Grupo-1Document6 pagesAlkaloid Grupo-1BRENDA MARYSABEL ESTEBAN HUARINo ratings yet
- Brainaid CaseDocument4 pagesBrainaid CaseJyotiraditya Kumar JhaNo ratings yet
- Emerging Trends in Sales ManagementDocument14 pagesEmerging Trends in Sales ManagementAbdul Quadir100% (7)
- Technology and Operations ManagementDocument26 pagesTechnology and Operations ManagementAnna Dolot100% (1)
- 2020년 중소기업 전략기술로드맵 28 조선Document449 pages2020년 중소기업 전략기술로드맵 28 조선박선호No ratings yet
- Check Manual: ES SeriesDocument42 pagesCheck Manual: ES SeriesArturo CalderonNo ratings yet
- Principals of Potato Storage PDFDocument91 pagesPrincipals of Potato Storage PDFplutocowNo ratings yet
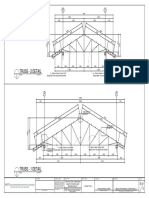
- Truss - 2 Detail: Scale 1: 50 MTRSDocument1 pageTruss - 2 Detail: Scale 1: 50 MTRSGerald MasangayNo ratings yet
- Job 1 Workout CalendarDocument1 pageJob 1 Workout CalendarnatalipaskalNo ratings yet
- The History of Computers: Done by - Anandhu Raj, Albin Raphy, Anirudh C. VinayanDocument42 pagesThe History of Computers: Done by - Anandhu Raj, Albin Raphy, Anirudh C. Vinayanarjun rajNo ratings yet
- Speedy ConstructionDocument57 pagesSpeedy Constructionritika bhatiaNo ratings yet
- Breach of ContractDocument27 pagesBreach of ContractTsholofelo50% (4)
- Felcom 15 Servi̇s ManualDocument236 pagesFelcom 15 Servi̇s ManualAnıl Kahya75% (8)
- ARA 111 (PREPARATORY ARABIC) - First Sem 2021Document15 pagesARA 111 (PREPARATORY ARABIC) - First Sem 2021Mohaimen GuroNo ratings yet
- AnnualReport - 2013 - BSPDocument88 pagesAnnualReport - 2013 - BSPlito77No ratings yet
- Collier - EditanDocument210 pagesCollier - EditanHachi JazuliNo ratings yet
- LOGIT ONE RegistrationDocument24 pagesLOGIT ONE RegistrationsitsekharNo ratings yet
- SCM Final ReportDocument12 pagesSCM Final ReportSYED DANIYAL HASSAN SHAHNo ratings yet
- Hyponic Full Catalog WEBDocument144 pagesHyponic Full Catalog WEBIsidro Pale CordobaNo ratings yet