Download as pdf or txt
You might also like
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- KPJ Healthcare University CollegeDocument95 pagesKPJ Healthcare University CollegeArchanah Rajamanikam50% (2)
- Pance Prep Pearls Antibiotics PDFDocument14 pagesPance Prep Pearls Antibiotics PDFkatNo ratings yet
- Pharm Practice QuestionsDocument42 pagesPharm Practice QuestionsShannon Garcia100% (1)
- Ob Gyn AdultDocument3 pagesOb Gyn AdultHarshit RastogiNo ratings yet
- Journal 2 Pneumonia - 3Document1 pageJournal 2 Pneumonia - 3dwi-148502No ratings yet
- Management of CAP in Adults - Ontario GovernmentDocument2 pagesManagement of CAP in Adults - Ontario GovernmentSukhvir AujlaNo ratings yet
- Guidelines For Treatment of Intra-Abdominal Infections in AdultsDocument10 pagesGuidelines For Treatment of Intra-Abdominal Infections in AdultsPratama InsaniNo ratings yet
- WFBMC Community Acquired Pneumonia (CAP) Treatment Guide For AdultsDocument2 pagesWFBMC Community Acquired Pneumonia (CAP) Treatment Guide For AdultsAlmas Safina KauserNo ratings yet
- Guideline For The Management of Community-Acquired PneumoniaDocument11 pagesGuideline For The Management of Community-Acquired PneumoniaCarlos VSNo ratings yet
- CAP Guidance 2020 Revision Final UpdatedDocument11 pagesCAP Guidance 2020 Revision Final UpdatedNeerajaNo ratings yet
- Fraser Health Antimicrobial Handbook 2016 - 04 - 25 - AspirationDocument1 pageFraser Health Antimicrobial Handbook 2016 - 04 - 25 - AspirationBoy ReynaldiNo ratings yet
- Glenda AnehDocument4 pagesGlenda AnehglendaNo ratings yet
- FeverDocument27 pagesFeverTilaye GebruNo ratings yet
- Streptococcus Pneumoniae Haemophilus Influenzae: Click HereDocument3 pagesStreptococcus Pneumoniae Haemophilus Influenzae: Click HereSiti Hidayatul FitriNo ratings yet
- Antibiotka PicuDocument4 pagesAntibiotka Picusunu rachmat100% (1)
- SHC Intra Abdominal GuidelinesDocument13 pagesSHC Intra Abdominal GuidelinesNguyễn Mạnh CườngNo ratings yet
- Antimicrobial Guidelines 2024Document99 pagesAntimicrobial Guidelines 2024Cesar HerreraNo ratings yet
- Empiric Antibiotic ListDocument2 pagesEmpiric Antibiotic ListpasswordNo ratings yet
- Cap Hap VapDocument2 pagesCap Hap Vapapi-535300613No ratings yet
- VAP Guidelines 7.7.04aDocument5 pagesVAP Guidelines 7.7.04aCorina DavidNo ratings yet
- SHC Outpatient Cough GuideDocument2 pagesSHC Outpatient Cough GuideKanaga6432No ratings yet
- Pulmonary InfectionsDocument16 pagesPulmonary InfectionsFawad AhmedNo ratings yet
- Camp General Servillano A Aquino, 2301 San Miguel, Tarlac CityDocument9 pagesCamp General Servillano A Aquino, 2301 San Miguel, Tarlac CityRuffa FriasNo ratings yet
- CPG Typhoid Fever 2017Document11 pagesCPG Typhoid Fever 2017Tam Adrian Aya-ayNo ratings yet
- Antibiotic Guidelines For SKIN AND SOFT TISSUE INFECTIONSDocument11 pagesAntibiotic Guidelines For SKIN AND SOFT TISSUE INFECTIONSlaptopgreyNo ratings yet
- Management of Healthcare-Associated Pneumonia (HCAP) in AdultsDocument3 pagesManagement of Healthcare-Associated Pneumonia (HCAP) in Adultstheseus5No ratings yet
- Pneumonia: Fever Cough Breathlessnes S DR J Pap/ich/ GMC Kottayam/19723Document4 pagesPneumonia: Fever Cough Breathlessnes S DR J Pap/ich/ GMC Kottayam/19723Firdouse ShajiNo ratings yet
- PneumoniaDocument17 pagesPneumoniaamrokhalefa21No ratings yet
- Hosp Ops II Week 3 Questions 1Document2 pagesHosp Ops II Week 3 Questions 1api-650133203No ratings yet
- Pediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic DiscussionDocument5 pagesPediatric Hospital-Acquired and Ventilator-Associated Pneumonia Topic Discussionapi-602288180No ratings yet
- Pneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Document2 pagesPneumonia Treatment Algorithm With Addendum For Aspiration 2015-2016.01.19Irsalina TriastutikNo ratings yet
- Coursera ABSDocument8 pagesCoursera ABSevanoNo ratings yet
- SHC Influenza Outpatient GuidelineDocument3 pagesSHC Influenza Outpatient GuidelineKanaga6432No ratings yet
- Antimicrobial Treatment Guidelines For Common Infections enDocument111 pagesAntimicrobial Treatment Guidelines For Common Infections enRoofia VahedianNo ratings yet
- Solid Tumor Febrile NeutropeniaDocument12 pagesSolid Tumor Febrile NeutropeniaSimonNo ratings yet
- Aminoglycosides: Pharmacology & TherapeuticsDocument24 pagesAminoglycosides: Pharmacology & TherapeuticsMarieNo ratings yet
- GNR Bacteremia De-Escalation Guide Final PDFDocument2 pagesGNR Bacteremia De-Escalation Guide Final PDFAbu Hammoud AlyazeediNo ratings yet
- Central Nervous System InfectionsDocument9 pagesCentral Nervous System InfectionsSaddamNo ratings yet
- Internal Abdominal Infection Treatment ProtocolDocument9 pagesInternal Abdominal Infection Treatment Protocolhatem newishyNo ratings yet
- Pediatrics Community Acquired Pneumonia: Isimijola OpeyemiDocument30 pagesPediatrics Community Acquired Pneumonia: Isimijola OpeyemiFavourNo ratings yet
- Escalation Guide For Gram-Negative Bacteremia StanfordDocument3 pagesEscalation Guide For Gram-Negative Bacteremia StanfordLuis MedinaNo ratings yet
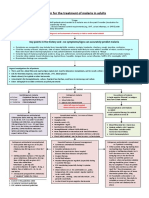
- Algorithm For The Treatment of Malaria in AdultsDocument1 pageAlgorithm For The Treatment of Malaria in AdultsRihab IsmaeelNo ratings yet
- Dr. Dian Kusumaningrum - PRESENTASI JCCA-ANTIBIOTIC DOSING IN CRITICALLY ILLDocument31 pagesDr. Dian Kusumaningrum - PRESENTASI JCCA-ANTIBIOTIC DOSING IN CRITICALLY ILLRestu TriwulandaniNo ratings yet
- Ckhs Empiric Antibiotic Guidance For Adult Pneumonia.2016Document3 pagesCkhs Empiric Antibiotic Guidance For Adult Pneumonia.2016surenvishvaNo ratings yet
- Diarrhea ADULTDocument10 pagesDiarrhea ADULTanakmaidNo ratings yet
- Slide Infectious DiseaseDocument42 pagesSlide Infectious Diseaseandirio7486No ratings yet
- 2RS. 3 PneumoniaDocument33 pages2RS. 3 PneumoniaMuath AlqarniNo ratings yet
- Antibiotic Policy - Final GovtMP - 211215 - 121049Document40 pagesAntibiotic Policy - Final GovtMP - 211215 - 121049Charchit MehtaNo ratings yet
- Cefixime: Suprax Class and CategoryDocument3 pagesCefixime: Suprax Class and CategoryArianne Joy SalvadorNo ratings yet
- 30 Glycopeptides Vancomycin and Teicoplanin 2015 Mandell Douglas and BDocument29 pages30 Glycopeptides Vancomycin and Teicoplanin 2015 Mandell Douglas and BHelen DyNo ratings yet
- BCCDC Non-Certified Practice Decision Support Tool Pelvic Inflammatory Disease (PID)Document10 pagesBCCDC Non-Certified Practice Decision Support Tool Pelvic Inflammatory Disease (PID)sandeepv08No ratings yet
- Drug Study of CiprofloxacinDocument3 pagesDrug Study of CiprofloxacinZyra MendozaNo ratings yet
- Empiric Treatment Guidelines Common InfectionsDocument9 pagesEmpiric Treatment Guidelines Common InfectionsShiza Batool100% (1)
- TASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)Document2 pagesTASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)ጉራማይሌ TubeNo ratings yet
- Severe Sepsis and Septic Shock Antibiotic Guide: Community AcquiredDocument6 pagesSevere Sepsis and Septic Shock Antibiotic Guide: Community AcquiredAnonymous G6zDTD2yNo ratings yet
- ChemotherapyDocument46 pagesChemotherapyErl D. Melitante100% (1)
- Penicillins and CephalosporinsDocument30 pagesPenicillins and CephalosporinsSri RamNo ratings yet
- NICU ABX ChartDocument11 pagesNICU ABX ChartdrchiNo ratings yet
- Fluconazole: ErthromycinDocument7 pagesFluconazole: ErthromycinAseel AlsheeshNo ratings yet
- CNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Document1 pageCNS: Ent:: Review Antibiotic Therapy Daily - Can You: Stop? Switch? Simplify? or State Duration?Fitri RachmadaniNo ratings yet
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!From EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Rating: 5 out of 5 stars5/5 (4)
- LEVOFLOXACIN MonographDocument3 pagesLEVOFLOXACIN Monographfayrouz fathiNo ratings yet
- Levofloxacin - Wikipedia, The Free EncyclopediaDocument19 pagesLevofloxacin - Wikipedia, The Free EncyclopediaAnkan PalNo ratings yet
- Screenshot 2021-06-19 at 21.33.17Document11 pagesScreenshot 2021-06-19 at 21.33.17bagus aldiNo ratings yet
- Minutesof 287 Thmeetingof Registration BoardDocument933 pagesMinutesof 287 Thmeetingof Registration BoardSaheefaNo ratings yet
- Levofloxacin On Tuberculosis TherapyDocument2 pagesLevofloxacin On Tuberculosis TherapyTopan BagaskaraNo ratings yet
- Manipulação 60 114Document55 pagesManipulação 60 114Zilmar OliveiraNo ratings yet
- IDSA Uncomplicated Cystitis and Pyelonephritis GuidelinesDocument18 pagesIDSA Uncomplicated Cystitis and Pyelonephritis GuidelinesDinoop Korol PonnambathNo ratings yet
- Drug ListDocument66 pagesDrug ListShashi DharNo ratings yet
- Kul3 - Pneumonia Uby s2-2011Document175 pagesKul3 - Pneumonia Uby s2-2011Suci HerawatiNo ratings yet
- Antibiotics 1Document41 pagesAntibiotics 1AlaaNo ratings yet
- Antibotics Venn DiagramDocument2 pagesAntibotics Venn DiagramTop Vids100% (1)
- Key Points PharmaDocument22 pagesKey Points PharmaZaib ZaibNo ratings yet
- Nahdi Pharma FileDocument477 pagesNahdi Pharma FileSarah JeanNo ratings yet
- MH BukuDocument33 pagesMH Bukunurul rezki fitrianiazisNo ratings yet
- MCQ Questions Lahore MedicalDocument36 pagesMCQ Questions Lahore MedicalClinicalTraining0% (1)
- Quinolones: Presented by Asst. Prof Jagir Patel Dept. PharmacologyDocument37 pagesQuinolones: Presented by Asst. Prof Jagir Patel Dept. PharmacologyJagirNo ratings yet
- Levofloxacin Versus MoxifloxacinDocument3 pagesLevofloxacin Versus MoxifloxacinRina Trihandayani PutriNo ratings yet
- Glevo RespicareDocument58 pagesGlevo RespicarekurutalaNo ratings yet
- Amended Levaquin ComplaintDocument82 pagesAmended Levaquin ComplaintDaily Caller News Foundation100% (2)
- Avoiding CPSEs - Laboratory Medication Vital SignsDocument30 pagesAvoiding CPSEs - Laboratory Medication Vital SignsForNo ratings yet
- 5) General BacteriologyDocument86 pages5) General BacteriologyIanBiagtanNo ratings yet
- Cellulitis and ErysipelasDocument9 pagesCellulitis and ErysipelasGabriel Muñoz LumbrerasNo ratings yet
- بطيخة الفارما (antibiotic) PDFDocument31 pagesبطيخة الفارما (antibiotic) PDFweele samaNo ratings yet
- AntibioticsDocument16 pagesAntibioticsVincent Raphael Baraan AcostaNo ratings yet
- 7 Pharmacology - FinalDocument17 pages7 Pharmacology - FinalIngrid NicolasNo ratings yet
- Final Filed Levaquin Complaint Johnson & Johnson JanssenDocument72 pagesFinal Filed Levaquin Complaint Johnson & Johnson JanssenMelayna LokoskyNo ratings yet
- AV Y TẾ 2Document27 pagesAV Y TẾ 2Đạt Bùi TiếnNo ratings yet