Download as pdf or txt
You might also like
- AMEE 2023 - Online Abstract BookDocument345 pagesAMEE 2023 - Online Abstract BookkxthshnkzcNo ratings yet
- Mbbs Bds Merit17Document750 pagesMbbs Bds Merit17Thota MaheshNo ratings yet
- 12 Tips For Community Based Medical EducationDocument4 pages12 Tips For Community Based Medical EducationRiry AmbarsaryNo ratings yet
- Branch Et Al 2001 Teaching The Human Dimensions of Care in Clinical SettingsDocument8 pagesBranch Et Al 2001 Teaching The Human Dimensions of Care in Clinical Settingsapi-264671444No ratings yet
- Student Voices Following Fieldwork FailureDocument14 pagesStudent Voices Following Fieldwork FailureSergioNo ratings yet
- Rowe - Blended Learning - 2012Document10 pagesRowe - Blended Learning - 2012Zilbran BerontaxNo ratings yet
- 1 s2.0 S1807593222001119 MainDocument6 pages1 s2.0 S1807593222001119 MainNadiraNo ratings yet
- A Qualitative Case Study of Best Practices in Holistic EducationFrom EverandA Qualitative Case Study of Best Practices in Holistic EducationNo ratings yet
- Article - INFUSION - OF - AGE-FRIENDLY - PRINCIPLES - INTO - CURRICULADocument1 pageArticle - INFUSION - OF - AGE-FRIENDLY - PRINCIPLES - INTO - CURRICULAHarlene ArabiaNo ratings yet
- Cbme 3Document5 pagesCbme 3Narendra Kumar GuptaNo ratings yet
- 1 s2.0 S2405844020307052 MainDocument4 pages1 s2.0 S2405844020307052 Mainrodriguescatia306992No ratings yet
- Education in PracticeDocument38 pagesEducation in PracticeTiti AjayiNo ratings yet
- Journal Pre-Proof: Nurse Education in PracticeDocument25 pagesJournal Pre-Proof: Nurse Education in PracticewidyadariNo ratings yet
- Revision of Thesis Problems of StudentsDocument56 pagesRevision of Thesis Problems of Studentsroselletimagos30No ratings yet
- Dissertation Ideas Mental Health Social WorkDocument4 pagesDissertation Ideas Mental Health Social WorkPayToDoMyPaperSingapore100% (1)
- Literature Review On Mentorship in NursingDocument7 pagesLiterature Review On Mentorship in Nursingafmzqlbvdfeenz100% (1)
- Collaborative LearningDocument12 pagesCollaborative LearningdoctorsujitNo ratings yet
- ResearchDocument14 pagesResearch9qhns8bcx5No ratings yet
- 1 s2.0 S1471595320310349 MainDocument6 pages1 s2.0 S1471595320310349 MainKAN NIMITPRASERTNo ratings yet
- Zareen Zaidi, Eric I. Rosenberg, Rebecca J. Beyth - Contemporary Challenges in Medical Education - From Theory To Practice-University of Florida Press (2019)Document297 pagesZareen Zaidi, Eric I. Rosenberg, Rebecca J. Beyth - Contemporary Challenges in Medical Education - From Theory To Practice-University of Florida Press (2019)INA SAKTINo ratings yet
- IntroagainDocument48 pagesIntroagainroselletimagos30No ratings yet
- Assignment - Essential QuestionsDocument5 pagesAssignment - Essential QuestionsFionah RetuyaNo ratings yet
- Ebp in Health EducationDocument25 pagesEbp in Health EducationPablito NazarenoNo ratings yet
- Diana Barnett Course Critique n5327 RDocument4 pagesDiana Barnett Course Critique n5327 Rapi-308950624No ratings yet
- Health Care ManagementDocument6 pagesHealth Care ManagementRajiv AroraNo ratings yet
- School Centered Interventions Intro SampleDocument11 pagesSchool Centered Interventions Intro SampleOwoso KudiratNo ratings yet
- Challenging Behaviour in Secondary SchooDocument23 pagesChallenging Behaviour in Secondary Schoosuleman0% (1)
- Branch 2015Document6 pagesBranch 2015Shabrina AliyahNo ratings yet
- The Code of Ethics For Nurses-More Relevant Than Ever: EditorialDocument2 pagesThe Code of Ethics For Nurses-More Relevant Than Ever: EditorialafsdsaadsNo ratings yet
- Classmate Peer-CoachingDocument14 pagesClassmate Peer-CoachingMontathar Abd Al NabiNo ratings yet
- Chapter Ii Revised EditionDocument19 pagesChapter Ii Revised EditionCharrie Faye Magbitang HernandezNo ratings yet
- Person Centred Care Literature ReviewDocument8 pagesPerson Centred Care Literature Reviewnidokyjynuv2100% (1)
- The Problems and Adjustments Encountered by The NursingDocument32 pagesThe Problems and Adjustments Encountered by The Nursingjezzabellganda100% (3)
- J5 (Scopus)Document10 pagesJ5 (Scopus)Imrul KayesNo ratings yet
- The Development of A Questionnaire To Assess The Readiness (Nurse)Document6 pagesThe Development of A Questionnaire To Assess The Readiness (Nurse)neizhaNo ratings yet
- Twelve Tips For Getting Started Using Mixed Methods in Medical Education ResearchDocument6 pagesTwelve Tips For Getting Started Using Mixed Methods in Medical Education ResearchlmadrazoNo ratings yet
- Content ServerDocument11 pagesContent ServerMona AL-FaifiNo ratings yet
- Specialty: Journal of Applied Behavior Analysis NumberDocument6 pagesSpecialty: Journal of Applied Behavior Analysis NumberalpNo ratings yet
- Communication Skills in Medical Education: An Integrated ApproachDocument13 pagesCommunication Skills in Medical Education: An Integrated ApproachMedicina IcesiNo ratings yet
- Community Medicine in Homoeopathy - Way Forward To Reform and InstituteDocument4 pagesCommunity Medicine in Homoeopathy - Way Forward To Reform and InstituteDr JeshNo ratings yet
- Nurse Education in Practice: Original ResearchDocument7 pagesNurse Education in Practice: Original ResearchSuriyanis LambeNo ratings yet
- Teaching & Learning in Context:: A Curriculum PerspectiveDocument35 pagesTeaching & Learning in Context:: A Curriculum PerspectiveMira ManoharanNo ratings yet
- Applying Self-Directed Learning Strategy To Enhance Nursing Students' Critical Thinking SkillsDocument12 pagesApplying Self-Directed Learning Strategy To Enhance Nursing Students' Critical Thinking SkillsZilbran BerontaxNo ratings yet
- Adaptation of The Academic Coping Strategies Scale in Turkey: A Study With UndergraduatesDocument19 pagesAdaptation of The Academic Coping Strategies Scale in Turkey: A Study With UndergraduatesShanmuga PriyaNo ratings yet
- Adult Learnng RoleDocument13 pagesAdult Learnng RoleLoganathan ChandrasekarNo ratings yet
- Dizon - Padrigone - Chapter 1 PDFDocument5 pagesDizon - Padrigone - Chapter 1 PDFViktoria DizonNo ratings yet
- Activity 3.1Document7 pagesActivity 3.1sanchezanya34No ratings yet
- Research Clinical Instructors RevisedDocument28 pagesResearch Clinical Instructors RevisedKateMighty AgbalogNo ratings yet
- Inclusive Education Literature ReviewDocument6 pagesInclusive Education Literature Reviewafmzrxbdfadmdq100% (1)
- Developing Interprofessional Communication SkillsDocument5 pagesDeveloping Interprofessional Communication SkillsWai AbrahamNo ratings yet
- Report For Teacher Training5Document10 pagesReport For Teacher Training5Aqsa ShafiqueNo ratings yet
- Coping Skills AdolescentsDocument19 pagesCoping Skills AdolescentsZayra UribeNo ratings yet
- COMSEP Journal Club December 2018: What Was The Study Question?Document4 pagesCOMSEP Journal Club December 2018: What Was The Study Question?robert dudasNo ratings yet
- Thomas 2016Document6 pagesThomas 2016Septyana M ANo ratings yet
- Final NaDocument42 pagesFinal NaChastin PeriasNo ratings yet
- Transformative Leadership Training in Medical Education A TopologyDocument9 pagesTransformative Leadership Training in Medical Education A Topologyslahri7No ratings yet
- Group4 Clinical Teaching 2Document22 pagesGroup4 Clinical Teaching 2Dexter PlamencoNo ratings yet
- Curriculum Planning & DevelopmentDocument13 pagesCurriculum Planning & DevelopmentMark Madridano100% (1)
- Promoting Student Resilience in School Contexts: Theory Into PracticeDocument9 pagesPromoting Student Resilience in School Contexts: Theory Into Practiceapi-303037281No ratings yet
- Health Promotion in Context: A Reflective-Analytical ModelDocument6 pagesHealth Promotion in Context: A Reflective-Analytical Modelmitha letoNo ratings yet
- Preventive Mental Health at School: Evidence-Based Services for StudentsFrom EverandPreventive Mental Health at School: Evidence-Based Services for StudentsNo ratings yet
- Schedule FTF Clerks 11 Oct 15 NovDocument5 pagesSchedule FTF Clerks 11 Oct 15 NovAngela Saldajeno100% (1)
- First Round Merit List of All India UG 2022Document15 pagesFirst Round Merit List of All India UG 2022Manswi SahareNo ratings yet
- NSV Empanelled Providers List District: Kancheepuram YEAR: 2019-20 (As On 16.12.2019)Document5 pagesNSV Empanelled Providers List District: Kancheepuram YEAR: 2019-20 (As On 16.12.2019)CHANDRAN MAHANo ratings yet
- Simulation in Health Care Education: Perspectives in Biology and Medicine February 2008Document6 pagesSimulation in Health Care Education: Perspectives in Biology and Medicine February 2008Birendra MahatNo ratings yet
- PDFDocument98 pagesPDFPrince Kumar singhNo ratings yet
- Gift ListDocument15 pagesGift ListSubhranil BarmanNo ratings yet
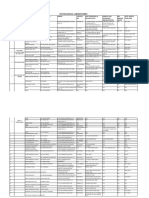
- Admission Committee For Professional Post-Graduate Medical Courses (Acppgmc) and All India - Medical College, Baroda. Year-2018-2019 .Document5 pagesAdmission Committee For Professional Post-Graduate Medical Courses (Acppgmc) and All India - Medical College, Baroda. Year-2018-2019 .Abhishek JoshiNo ratings yet
- Jubilee Mission College of Nursing: Management Details of Contact PersonDocument1 pageJubilee Mission College of Nursing: Management Details of Contact PersonGD KVNo ratings yet
- District DataDocument242 pagesDistrict Dataayush.bullethealthcareNo ratings yet
- MMMD Allot 2010Document73 pagesMMMD Allot 2010weepingwillowleafNo ratings yet
- Gui Tu Fucuehs7 Tu FududuDocument212 pagesGui Tu Fucuehs7 Tu FududuAkash PareekNo ratings yet
- 2nd Round Seat Allotment Result MDMS MDS Final NET2Document52 pages2nd Round Seat Allotment Result MDMS MDS Final NET2SARKAR JAVED AKHTARNo ratings yet
- List of Permitted ASU Colleges 2019Document17 pagesList of Permitted ASU Colleges 2019Dr-Sudhir Dutt BhardwajNo ratings yet
- Bharati Vidyapeeth (Deemed To Be University) Medical College & Hospital, Sangli PG (MD/MS) Seats InformationDocument6 pagesBharati Vidyapeeth (Deemed To Be University) Medical College & Hospital, Sangli PG (MD/MS) Seats Informationvishal wadNo ratings yet
- SB 3: Medical Marijuana BillDocument26 pagesSB 3: Medical Marijuana BillSteven DoyleNo ratings yet
- Gyne Onco Mission 2022Document5 pagesGyne Onco Mission 2022Dominque RabastoNo ratings yet
- Effective Educational and Clinical SupervisionDocument19 pagesEffective Educational and Clinical SupervisionMohammad Sutami100% (1)
- All India Pre-Medical/ Pre-Dental Test: TimelineDocument3 pagesAll India Pre-Medical/ Pre-Dental Test: TimelineAsmitNo ratings yet
- 1st Paying ListDocument314 pages1st Paying ListsmaricadhgNo ratings yet
- MD Peadiatrics NMC CURRICULUMDocument67 pagesMD Peadiatrics NMC CURRICULUMraghava mbbs100% (1)
- 5391 Choice ListDocument4 pages5391 Choice ListAhmed VanzaraNo ratings yet
- First Admission List March23 PDFDocument387 pagesFirst Admission List March23 PDFMedic IronyNo ratings yet
- NextGenU March2Document2 pagesNextGenU March2Anonymous vxLhRlVgjHNo ratings yet
- BUC Medicine Professional Development Study GuideDocument37 pagesBUC Medicine Professional Development Study GuideHabiba AhmedNo ratings yet
- Five Year Faculty Development Plan: Cagayan State UniversityDocument7 pagesFive Year Faculty Development Plan: Cagayan State UniversityAL Babaran CanceranNo ratings yet
- Medical Sociology: Some Problems For Study: C Parvathamma S SharadammaDocument4 pagesMedical Sociology: Some Problems For Study: C Parvathamma S SharadammaSiddardhaNo ratings yet
- 123 Anywhere ST., Any City, ST 12345 123-456-7890 Hello@Reallygreatsite - Com WWW - Reallygreatsite.com @reallygreatsiteDocument1 page123 Anywhere ST., Any City, ST 12345 123-456-7890 Hello@Reallygreatsite - Com WWW - Reallygreatsite.com @reallygreatsitevaen ronaNo ratings yet
- Medical College Gujarat Admission AnnouncementDocument16 pagesMedical College Gujarat Admission AnnouncementMonkey_002No ratings yet
- Bedside TeachingDocument23 pagesBedside TeachingBella HannaNo ratings yet