Download as pdf or txt
You might also like
- Kathleen McInnis-Dittrich - Social Work With Older Adults-Pearson (2013)Document399 pagesKathleen McInnis-Dittrich - Social Work With Older Adults-Pearson (2013)NICOLAS CISTERNAS SANDOVAL92% (12)
- Introduction On Gerontology NursingDocument36 pagesIntroduction On Gerontology NursingRuby Corazon Ediza50% (4)
- Clinical Function EQuIP6 Standard Tables. Final. 1Document25 pagesClinical Function EQuIP6 Standard Tables. Final. 1Intan PermataNo ratings yet
- Anaya-Estrada J-Attitudes and Believes PaperDocument14 pagesAnaya-Estrada J-Attitudes and Believes PaperAngel AnayaNo ratings yet
- 3e - End of Life Care-Russian PDFDocument2 pages3e - End of Life Care-Russian PDFtemp001bunnNo ratings yet
- Geria Prelims 1Document4 pagesGeria Prelims 1kurtsalvadorbsnNo ratings yet
- NCM 114 Mod4Document21 pagesNCM 114 Mod4Samantha Bolante100% (1)
- Biologyofageing 200410161806Document70 pagesBiologyofageing 200410161806Risda ArbaNo ratings yet
- 2 Theories of Aging PlpsDocument38 pages2 Theories of Aging Plpsclaire yowsNo ratings yet
- Geriatrics HandoutDocument16 pagesGeriatrics HandoutDiana BautistaNo ratings yet
- Concepts and Theories of Aging: Princy Francis M I Yr MSC (N) JmconDocument48 pagesConcepts and Theories of Aging: Princy Francis M I Yr MSC (N) Jmconcj bariasNo ratings yet
- Module 5 6Document5 pagesModule 5 6Nora VarshavskiNo ratings yet
- Geriatric Nursing: Theories of AgingDocument4 pagesGeriatric Nursing: Theories of AgingNikkaDablioNo ratings yet
- Lecture 1 2Document5 pagesLecture 1 2Raiden VizcondeNo ratings yet
- Concepts, Principles and Theories in The Care of Older AdultsDocument16 pagesConcepts, Principles and Theories in The Care of Older AdultsMARY CLAIRE SUMILHIGNo ratings yet
- Module 2 - Dynamics of The Aging ProcessDocument111 pagesModule 2 - Dynamics of The Aging ProcessAYTONA, JAMAICA F.No ratings yet
- Medical Surgical 3: Prepared By: Caroline V. San DiegoDocument43 pagesMedical Surgical 3: Prepared By: Caroline V. San DiegoJosh Nico JaoNo ratings yet
- NCM 114 ReviewerDocument9 pagesNCM 114 ReviewerLovely DaroleNo ratings yet
- Theories of AgingDocument36 pagesTheories of AgingSjerwin Anthony Gianan100% (1)
- Care of The Older Adult Handouts PrelimsDocument7 pagesCare of The Older Adult Handouts PrelimsAmanda Joy TuizaNo ratings yet
- Geriatric Nursing - SampleDocument7 pagesGeriatric Nursing - SampleCherry Joyce BascoNo ratings yet
- Gerontology and Geriatrics: Dr. Bernardo D. Morantte JRDocument9 pagesGerontology and Geriatrics: Dr. Bernardo D. Morantte JRRenz Francis SasaNo ratings yet
- PROFED 1 Midterm ReviewerDocument4 pagesPROFED 1 Midterm ReviewerK. U. A.No ratings yet
- Gerontological Nursing and Home Based Care-1-1Document148 pagesGerontological Nursing and Home Based Care-1-1joanwanjiku847No ratings yet
- NCM 114 ReviewerDocument12 pagesNCM 114 ReviewerEmmanuelNo ratings yet
- Late AdulthoodDocument43 pagesLate AdulthoodAsthra R.No ratings yet
- Nursing Elective 4rth Copy CompleteDocument229 pagesNursing Elective 4rth Copy CompleteGeddy SarigumbaNo ratings yet
- Theories On AgingDocument32 pagesTheories On AgingAerickt Sioco-InsertoNo ratings yet
- Stress Final-NepDocument82 pagesStress Final-NepChonkayshek Rias BarrunNo ratings yet
- Gerontological PrelimDocument126 pagesGerontological PrelimAyessa Yvonne PanganibanNo ratings yet
- Geria 2 TheoriesDocument73 pagesGeria 2 TheoriesMark DominicNo ratings yet
- TEMARIO GERIATRÍA Parte 1Document10 pagesTEMARIO GERIATRÍA Parte 1MARIANo ratings yet
- BIOETHICS Unit 1 and 2Document9 pagesBIOETHICS Unit 1 and 2Fae Nicole MangilimanNo ratings yet
- Care of The Chronically Ill and The Older PersonDocument109 pagesCare of The Chronically Ill and The Older PersonJennifer Gross100% (3)
- Theories of Aging: Akshata Hinge Akshata AradhyeDocument15 pagesTheories of Aging: Akshata Hinge Akshata AradhyeAditi ChaurasiaNo ratings yet
- Adult CareDocument44 pagesAdult CareACERET, IVAN LAURENTINE G.No ratings yet
- Young Old Middle-Old Old-Old (Ages Elite OldDocument5 pagesYoung Old Middle-Old Old-Old (Ages Elite OldReignlyNo ratings yet
- Geriatrics 1Document22 pagesGeriatrics 1valdez.adler.lNo ratings yet
- NCM 114: Care of The Older Adult Instructor: Gino Paulo A. Buizon, R.NDocument9 pagesNCM 114: Care of The Older Adult Instructor: Gino Paulo A. Buizon, R.NJay VillasotoNo ratings yet
- Concept and Theory of Ageing1Document23 pagesConcept and Theory of Ageing1honeyy825No ratings yet
- M1. B4. U6. Elderly CareDocument83 pagesM1. B4. U6. Elderly CareprashantNo ratings yet
- Nursing Ageing of TheoriesDocument10 pagesNursing Ageing of Theoriesprema balusamyNo ratings yet
- ReportDocument13 pagesReportDoneva Lyn MedinaNo ratings yet
- Neuroendocrine Andneurochemical Theories in AgingDocument3 pagesNeuroendocrine Andneurochemical Theories in Agingiheart musicNo ratings yet
- Ncm114j Care of The Older AdultsDocument10 pagesNcm114j Care of The Older AdultsCarl John ManaloNo ratings yet
- NCM114 Week 1 4Document7 pagesNCM114 Week 1 4Daisy RoseteNo ratings yet
- Psycological Ageing of TheoriesDocument7 pagesPsycological Ageing of Theoriesprema balusamyNo ratings yet
- S207 LP01 Week3 NotesDocument50 pagesS207 LP01 Week3 NoteseloithatNo ratings yet
- GerontologyDocument150 pagesGerontologyKakak wawa95No ratings yet
- Thebiologyofageing 170828072832Document42 pagesThebiologyofageing 170828072832Risda ArbaNo ratings yet
- Care of The Chronically Ill and The Older PersonDocument8 pagesCare of The Chronically Ill and The Older PersonAnne Con100% (1)
- Theories of Ageing: DR Prema BalusamyDocument19 pagesTheories of Ageing: DR Prema Balusamyprema balusamyNo ratings yet
- Psych NotesDocument17 pagesPsych NotesAlexa ParagamacNo ratings yet
- Perspective of AgingDocument21 pagesPerspective of AgingMarianne Joyce ManzoNo ratings yet
- Geriatric Nursing Week2Document45 pagesGeriatric Nursing Week2Matt Lao DionelaNo ratings yet
- Grade 7 Self-Learning ModuleDocument14 pagesGrade 7 Self-Learning Moduledibose8563100% (1)
- Human Development: Management Public Behaviour Novita D PutriDocument68 pagesHuman Development: Management Public Behaviour Novita D PutriNovi JCorpsNo ratings yet
- Dev Psych Chapter 2Document6 pagesDev Psych Chapter 2KARYLLE MAE MACOROLNo ratings yet
- Intro To Pharmacuetical Care - Lesson 2Document11 pagesIntro To Pharmacuetical Care - Lesson 2michelle bualNo ratings yet
- Anp Presentation On GeriatricsDocument114 pagesAnp Presentation On Geriatricsgeetanjali behl100% (3)
- NCM 114 Theories of AgingDocument30 pagesNCM 114 Theories of AgingThea IlaoNo ratings yet
- Group 4Document10 pagesGroup 4Franz CaputolanNo ratings yet
- Bioethical IssuesDocument22 pagesBioethical IssuesALYSSA NICOLE GINESNo ratings yet
- The Longevity Code: Unlocking the Secrets to Living a Longer, Healthier, and More Vibrant LifeFrom EverandThe Longevity Code: Unlocking the Secrets to Living a Longer, Healthier, and More Vibrant LifeNo ratings yet
- Decade Report Full Report Final-LinkedDocument250 pagesDecade Report Full Report Final-LinkedJosh Arno M SilitongaNo ratings yet
- Death and DyingDocument139 pagesDeath and DyingMeredith Galvez100% (1)
- Final EvaluationDocument17 pagesFinal Evaluationapi-603938769No ratings yet
- Baker 2022Document11 pagesBaker 2022ahmad azhar marzuqiNo ratings yet
- Introductory Medical Surgical Nursing Timby 11th Edition Test BankDocument14 pagesIntroductory Medical Surgical Nursing Timby 11th Edition Test Bankteresastoneniegwrjcyt100% (30)
- End-Of-Life Decision Making Across CulturesDocument15 pagesEnd-Of-Life Decision Making Across CulturesPamNo ratings yet
- Client Comfort and End-of-Life Care Reflection and QuestionsDocument4 pagesClient Comfort and End-of-Life Care Reflection and QuestionsArkham100% (1)
- L - NHS EoLC Programme Holistic Common Assessment Document 2010Document32 pagesL - NHS EoLC Programme Holistic Common Assessment Document 2010instranapNo ratings yet
- Ilovepdf MergedDocument53 pagesIlovepdf MergedJoel CalapiñaNo ratings yet
- Case ReflectionDocument7 pagesCase ReflectionAmanat KangNo ratings yet
- Dignity in Care The Human Side of Medicine Harvey Max Chochinov Full ChapterDocument67 pagesDignity in Care The Human Side of Medicine Harvey Max Chochinov Full Chapterjoshua.little480100% (17)
- End of Life Care PPPDocument43 pagesEnd of Life Care PPPElaine SUNo ratings yet
- Humanistic Nursing Theory: Application To Hospice and Palliative CareDocument9 pagesHumanistic Nursing Theory: Application To Hospice and Palliative CareNYONGKERNo ratings yet
- Advance Care Planning-Malaysian Hospice Congress - DR Wu Huei YawDocument42 pagesAdvance Care Planning-Malaysian Hospice Congress - DR Wu Huei Yawmalaysianhospicecouncil6240No ratings yet
- Social Experiment 1 1Document5 pagesSocial Experiment 1 1SandyNo ratings yet
- Chochinov Dignity TherapyDocument6 pagesChochinov Dignity TherapySimona DavidNo ratings yet
- Goals of Patient Care GuidelineDocument12 pagesGoals of Patient Care GuidelineangelaNo ratings yet
- Kematian Di ICUDocument24 pagesKematian Di ICURahmida RahmyNo ratings yet
- End of Life Assignment - Plo4Document4 pagesEnd of Life Assignment - Plo4api-550346996No ratings yet
- Primary Care Workforce NeedsDocument16 pagesPrimary Care Workforce NeedsTanea IstratiiNo ratings yet
- EuthanasiaDocument14 pagesEuthanasiaVin BitzNo ratings yet
- Predicting End of Life: de Anna Looper, RN CHPNDocument4 pagesPredicting End of Life: de Anna Looper, RN CHPNSathiswebNo ratings yet
- Paliative Care - Parents PerspectivesDocument17 pagesPaliative Care - Parents Perspectivescarolina riveraNo ratings yet
- A Communication Strategy and Brochure For Relatives of Patients Dying in The ICU - Nejm - Lautrette - 469sa1Document79 pagesA Communication Strategy and Brochure For Relatives of Patients Dying in The ICU - Nejm - Lautrette - 469sa1Manuel PernetasNo ratings yet
- Aging Concepts and Controversies 9th Edition Moody Test Bank DownloadDocument6 pagesAging Concepts and Controversies 9th Edition Moody Test Bank DownloadPaula Marshall100% (21)
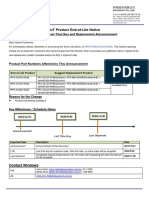
- Product Phase Out Notice IPPC 6152 6172 6192 R2AEDocument1 pageProduct Phase Out Notice IPPC 6152 6172 6192 R2AEguruh anindraNo ratings yet