Download as pps, pdf, or txt
You might also like
- Current Surgical Therapy 12Document1,828 pagesCurrent Surgical Therapy 12Huda Al-Anabr91% (34)
- Pcos - Clinical Case DiscussionDocument4 pagesPcos - Clinical Case Discussionreham macadatoNo ratings yet
- Presentation 2Document43 pagesPresentation 2talaarar695No ratings yet
- Polycystic Ovarian SyndromeDocument17 pagesPolycystic Ovarian SyndromeAhmed ElmohandesNo ratings yet
- NP020110 P18table1Document1 pageNP020110 P18table1Celine SuryaNo ratings yet
- Anovulatory InfertilityDocument57 pagesAnovulatory InfertilityUsha AnengaNo ratings yet
- Polycystic Ovary Syndrome 2016 NEJMDocument11 pagesPolycystic Ovary Syndrome 2016 NEJMGabrielaNo ratings yet
- Endometrial Hyperplasia and Endometrial CancerDocument14 pagesEndometrial Hyperplasia and Endometrial CancerAmmarNo ratings yet
- Polycystic Ovary SyndromeDocument11 pagesPolycystic Ovary SyndromeViridiana Briseño GarcíaNo ratings yet
- ?5 - Secondary AmenorrheaDocument5 pages?5 - Secondary AmenorrheaNashat SaadiNo ratings yet
- Cleveland Clinic Journal of Medicine 2004 Bembo 511 7Document7 pagesCleveland Clinic Journal of Medicine 2004 Bembo 511 7DewinsNo ratings yet
- Endometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDocument4 pagesEndometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDikie MustofadijayaNo ratings yet
- Polycystic Ovarian SyndromeDocument2 pagesPolycystic Ovarian SyndromeCarlo CruzNo ratings yet
- No. 34. Management of Infertility Caused by Ovulatory DysfunctionDocument19 pagesNo. 34. Management of Infertility Caused by Ovulatory DysfunctionAnnisa JuwitaNo ratings yet
- Polycystic Ovarian SyndromeDocument11 pagesPolycystic Ovarian Syndromezianab aliNo ratings yet
- Abnormal Uterine BleedingDocument11 pagesAbnormal Uterine BleedingKharmell Waters AndradeNo ratings yet
- ActivityDocument21 pagesActivityAbdullah ElgeddawyNo ratings yet
- Case Presentation Obstetrics & Gynecology Rumc: Attending: Dr. ShatsDocument14 pagesCase Presentation Obstetrics & Gynecology Rumc: Attending: Dr. ShatsNirmita J PatelNo ratings yet
- Polycystic Ovarian SyndromeDocument20 pagesPolycystic Ovarian SyndromeMuhammad khairul afizal RohimNo ratings yet
- Case Report: Pregnancy in An Infertile Woman With Polycystic Ovary SyndromeDocument4 pagesCase Report: Pregnancy in An Infertile Woman With Polycystic Ovary SyndromeEunice PalloganNo ratings yet
- Gestational Trophoblastic DiseaseDocument37 pagesGestational Trophoblastic DiseaseOlisa 'phage' Onyebuchi100% (1)
- InsulinomaDocument18 pagesInsulinomaBetta BeTta0% (1)
- Early Pregnancy Problems: Presented byDocument28 pagesEarly Pregnancy Problems: Presented byMalk OmryNo ratings yet
- PCOSDocument38 pagesPCOSJitendra Chaudhary100% (1)
- Secamenhyper 120208102817 Phpapp02Document31 pagesSecamenhyper 120208102817 Phpapp02Mohan DassNo ratings yet
- PCOS-Epidemiology: Age Which Approximately 4 Million IndividualsDocument66 pagesPCOS-Epidemiology: Age Which Approximately 4 Million IndividualsAseel wael alshareefNo ratings yet
- Medicine AssignmentDocument73 pagesMedicine AssignmentSahdhana IyerNo ratings yet
- PCOS DR BasimaDocument18 pagesPCOS DR BasimaA.H.ANo ratings yet
- Abnormal Uterine Bleeding in A 39 Year OldDocument16 pagesAbnormal Uterine Bleeding in A 39 Year OldEliana GerzonNo ratings yet
- سمنر نسائيهDocument20 pagesسمنر نسائيهsuad aliNo ratings yet
- PCOSDocument15 pagesPCOSAndyan Adlu PrasetyajiNo ratings yet
- Polycystic Ovarian SyndromeDocument46 pagesPolycystic Ovarian SyndromeStalin ChandrasekaranNo ratings yet
- Incidence of Endometrial Hyperplasia in 100 Cases Presenting With Polymenorrhagia/Menorrhagia in Perimenupausal WomenDocument4 pagesIncidence of Endometrial Hyperplasia in 100 Cases Presenting With Polymenorrhagia/Menorrhagia in Perimenupausal Womenfitrah fajrianiNo ratings yet
- Pre EclampsiaDocument12 pagesPre EclampsiaJohn Mark PocsidioNo ratings yet
- Amenorrhea: Evaluation & Treatment: Jurnal Reading Mohamad Athaullah 11.2012.062Document28 pagesAmenorrhea: Evaluation & Treatment: Jurnal Reading Mohamad Athaullah 11.2012.062Athaullah IsmailNo ratings yet
- Endometrial HyperplasiaDocument21 pagesEndometrial HyperplasiaEggyDs100% (3)
- Endometrial Hyperplasia - Gyn ReviewDocument18 pagesEndometrial Hyperplasia - Gyn ReviewFedrik Monte Kristo LimbongNo ratings yet
- A Common and Recognizable ConditionDocument27 pagesA Common and Recognizable ConditionWindy HapsariNo ratings yet
- MEN1 PPDocument15 pagesMEN1 PPAaron D. PhoenixNo ratings yet
- Gynecological Disorders in The Adolescent Gynecological Disorders in The AdolescentDocument31 pagesGynecological Disorders in The Adolescent Gynecological Disorders in The AdolescentarrypotterNo ratings yet
- Kri Edt 2018Document5 pagesKri Edt 2018Teguh Imana NugrahaNo ratings yet
- Under Supervision Of: Dr. Enas AdnanDocument9 pagesUnder Supervision Of: Dr. Enas AdnanSarraa NajimNo ratings yet
- My PCOSDocument54 pagesMy PCOSanees_aneessNo ratings yet
- 6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Document11 pages6 - Contemporary Management of Polycystic Ovarian Syndrome - 2019Johanna Bustos NutricionistaNo ratings yet
- Abnormal Uterine BleedingDocument22 pagesAbnormal Uterine BleedingAde JuandaNo ratings yet
- Polycystic Ovarian Syndrome DR. Hanaa Al HeideryDocument12 pagesPolycystic Ovarian Syndrome DR. Hanaa Al Heideryhacker ammerNo ratings yet
- Sop InfertDocument10 pagesSop InfertdrjosuejauNo ratings yet
- Karimzadeh 2010Document5 pagesKarimzadeh 2010Derevie Hendryan MoulinaNo ratings yet
- Polycystic Ovary Syndrome: A Review (Ricardo Azizz)Document3 pagesPolycystic Ovary Syndrome: A Review (Ricardo Azizz)Jeremy LickteigNo ratings yet
- AUB StartedDocument13 pagesAUB StartedIbrahim AbdullahNo ratings yet
- 11abnormal Uterine BleedingDocument32 pages11abnormal Uterine BleedingAkinbani MoyosoreNo ratings yet
- Uterine Bleeding-A Case StudyDocument4 pagesUterine Bleeding-A Case StudyRoanne Lagua0% (1)
- Contraception: Doctor's NoteDocument15 pagesContraception: Doctor's NoteRyubusa HayabusaNo ratings yet
- Sign of Hyperandrogenism PDFDocument6 pagesSign of Hyperandrogenism PDFmisbah_mdNo ratings yet
- PcosDocument9 pagesPcosMonomay HalderNo ratings yet
- Womens HealthDocument12 pagesWomens HealthPooja ChoudharyNo ratings yet
- Clinical Presentation and Diagnosis of Polycystic Ovarian SyndromeDocument9 pagesClinical Presentation and Diagnosis of Polycystic Ovarian SyndromeLia MeivianeNo ratings yet
- Gestational Trophoblastic DiseasesDocument37 pagesGestational Trophoblastic DiseasesEdwin OkonNo ratings yet
- Management of Abnormal Uterine Bleeding in Perimenarche: Diagnostic ChallengesDocument4 pagesManagement of Abnormal Uterine Bleeding in Perimenarche: Diagnostic ChallengesIda_Maryani94No ratings yet
- Association of Clinical Features With Obesity and Gonadotropin Levels in Women With Polycystic Ovarian SyndromeDocument4 pagesAssociation of Clinical Features With Obesity and Gonadotropin Levels in Women With Polycystic Ovarian Syndromedoctor wajihaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyFrom EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyNo ratings yet
- M.writing Skill Letter Writing (Aplication Letter)Document8 pagesM.writing Skill Letter Writing (Aplication Letter)Hafid JuniorNo ratings yet
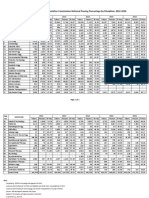
- PRC National Passing PercentageDocument2 pagesPRC National Passing PercentagenotshanderickNo ratings yet
- Perioperative NursingDocument15 pagesPerioperative Nursingmblanco.dchNo ratings yet
- Abortion Doctors Fail To Call AmbulancesDocument29 pagesAbortion Doctors Fail To Call AmbulancesCarole Novielli0% (1)
- Cardinal Santos Profile 2Document4 pagesCardinal Santos Profile 2Nina Fatima AllamNo ratings yet
- 0001 Interview Questions For Staff NursesDocument3 pages0001 Interview Questions For Staff NursesNatalia Fernández-Ochoa LlamazaresNo ratings yet
- Narrative ReportDocument2 pagesNarrative ReportLennieCartujanoLuceñoNo ratings yet
- Harmonized TTMF Assessment-Tool Final Draft Jul 27 2020Document10 pagesHarmonized TTMF Assessment-Tool Final Draft Jul 27 2020Jay EspinalNo ratings yet
- Westmead Obstetric AnaestheDocument85 pagesWestmead Obstetric Anaesthesum75No ratings yet
- National Electrical Code of The PhilippinesDocument5 pagesNational Electrical Code of The PhilippinesRuzel AmpoanNo ratings yet
- FR Radius UlnaDocument49 pagesFR Radius UlnaEkha SaraswatiNo ratings yet
- Overcrowding Patient and Improving Emergency Patient Flow in Emergency Department: A Literature ReviewDocument5 pagesOvercrowding Patient and Improving Emergency Patient Flow in Emergency Department: A Literature Reviewayu rahmaNo ratings yet
- Soal CampbellDocument5 pagesSoal CampbellAdryansyah ChaniagoNo ratings yet
- Antepartum HemorrhageDocument105 pagesAntepartum HemorrhageBablablo LolaleNo ratings yet
- Pain Management in Dentistry: Jeff Burgess, DDS, MSD (Retired) Clinical Assistant Professor, Department ofDocument14 pagesPain Management in Dentistry: Jeff Burgess, DDS, MSD (Retired) Clinical Assistant Professor, Department ofStefanus TabboNo ratings yet
- Gastric Bypass (GBP) and Sleeve Gastrectomy TR400.GBSG - Si: Da Vinci Si™ SystemDocument2 pagesGastric Bypass (GBP) and Sleeve Gastrectomy TR400.GBSG - Si: Da Vinci Si™ SystemShayne JacobsonNo ratings yet
- Medical Malpractice CasesDocument22 pagesMedical Malpractice CasesALEXANDRIA RABANES100% (2)
- Pre Operative Check List For OtDocument2 pagesPre Operative Check List For OtjaskiruNo ratings yet
- 201426112556-Ultrasom Musculoesq.Document5 pages201426112556-Ultrasom Musculoesq.Antero Marques CardosoNo ratings yet
- Teratogenic DrugsDocument8 pagesTeratogenic DrugsMudrekaNo ratings yet
- Final - Analgesia and Anaesthesia in Labor-FinalDocument22 pagesFinal - Analgesia and Anaesthesia in Labor-Finalnathsujitkr1980No ratings yet
- Michelle - Proctor@corrections - Govt.nz Cochrane Menstrual Disorders and Subfertility GroupDocument21 pagesMichelle - Proctor@corrections - Govt.nz Cochrane Menstrual Disorders and Subfertility GroupnarkeeshNo ratings yet
- Spouses Fredelicto Flores and Felicisima Flores v. Spouses Dominador Pineda and Virgina SacloloDocument5 pagesSpouses Fredelicto Flores and Felicisima Flores v. Spouses Dominador Pineda and Virgina SaclolojenizacallejaNo ratings yet
- AMREF Courses Calendar For 2009Document1 pageAMREF Courses Calendar For 2009Subi100% (2)
- ANESTHESIA (AIIMS & NEET - Recall Questions) Anesthesia T&DDocument4 pagesANESTHESIA (AIIMS & NEET - Recall Questions) Anesthesia T&DShweta SaraswatNo ratings yet
- Well Baby Write UpDocument3 pagesWell Baby Write UpNicklaus RiveraNo ratings yet
- Case ReportDocument5 pagesCase ReportNurRohmanNo ratings yet
- Septic Abortion PDFDocument4 pagesSeptic Abortion PDFmariachrismayaniNo ratings yet
- DT StrabismusDocument42 pagesDT StrabismushamzahNo ratings yet