Download as pdf or txt
You might also like
- Rilke's Book of Hours: Love Poems To GodDocument12 pagesRilke's Book of Hours: Love Poems To GodAlfonso14% (7)
- Lisa Blackman-Immaterial Bodies - Affect, Embodiment, Mediation (2012) PDFDocument241 pagesLisa Blackman-Immaterial Bodies - Affect, Embodiment, Mediation (2012) PDFCristina PeñamarínNo ratings yet
- Relations and FunctionsDocument10 pagesRelations and Functionskiahjessie100% (6)
- Treatment of Chronic InfectionDocument6 pagesTreatment of Chronic InfectionJonathan Munoz EscobedoNo ratings yet
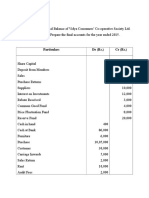
- Final AccountDocument7 pagesFinal Accountswati100% (3)
- Pin Site Care Using Chlorhexidine Case Study Report: Desak Wayan SuarsedewiDocument10 pagesPin Site Care Using Chlorhexidine Case Study Report: Desak Wayan SuarsedewiBabang YasNo ratings yet
- 217-Article Text-1787-1-10-20210904Document15 pages217-Article Text-1787-1-10-20210904Saffa AzharaaniNo ratings yet
- Pin Site Care Using Chlorhexidine Case Study Report: Desak Wayan SuarsedewiDocument10 pagesPin Site Care Using Chlorhexidine Case Study Report: Desak Wayan Suarsedewiirfani28No ratings yet
- Post-Instrumentation Infection Treatment NewDocument27 pagesPost-Instrumentation Infection Treatment NewmarmerosNo ratings yet
- Periodontology 2000 - 2023 - Monje - Selecting Biomaterials in The Reconstructive Therapy of Peri ImplantitisDocument20 pagesPeriodontology 2000 - 2023 - Monje - Selecting Biomaterials in The Reconstructive Therapy of Peri Implantitisodontosaludloschillos2023No ratings yet
- Local Anesthesia 2 - GaoDocument74 pagesLocal Anesthesia 2 - GaoIsak ShatikaNo ratings yet
- Do Patients With Prosthetic Joints Require Dental Antimicrobial ProphylaxisDocument3 pagesDo Patients With Prosthetic Joints Require Dental Antimicrobial Prophylaxistsiko111No ratings yet
- Endodontic Flare-Ups: An UpdateDocument6 pagesEndodontic Flare-Ups: An UpdateÁNGELA PAZ RIQUELME CEBALLOSNo ratings yet
- Chronic OsteomyelitisDocument6 pagesChronic Osteomyelitisdedyalkarni08No ratings yet
- Zalavras 2017Document14 pagesZalavras 2017alexi.garciaNo ratings yet
- Bone Graft SubstitutesDocument5 pagesBone Graft SubstitutessarraNo ratings yet
- Periimplantitele Diagnostic Si TratamentDocument10 pagesPeriimplantitele Diagnostic Si TratamentmarianNo ratings yet
- 2 - Care of Pin SitesDocument5 pages2 - Care of Pin SitessolihinNo ratings yet
- The Principles and Practice of Open Fracture Care, 2018: Amna Diwan, Kyle R. Eberlin, Raymond Malcolm SmithDocument7 pagesThe Principles and Practice of Open Fracture Care, 2018: Amna Diwan, Kyle R. Eberlin, Raymond Malcolm SmithMaria Dwi TibarsoniNo ratings yet
- Infection Following Bone Tumor Resection and Reconstruction With Tumoral Prostheses: A Literature Review F. CDocument9 pagesInfection Following Bone Tumor Resection and Reconstruction With Tumoral Prostheses: A Literature Review F. CWilson MartinezNo ratings yet
- Antibiotic BeadsDocument5 pagesAntibiotic BeadsAstary PasorongNo ratings yet
- Malleolar Fractures: Surgical Site Infection and Its Risk FactorsDocument18 pagesMalleolar Fractures: Surgical Site Infection and Its Risk FactorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Miller 1983Document3 pagesMiller 1983Francisco Castillo VázquezNo ratings yet
- Injury: F. Lavini, C. Dall'Oca, S. Mezzari, T. Maluta, E. Luminari, F. Perusi, E. Vecchini, B. MagnanDocument6 pagesInjury: F. Lavini, C. Dall'Oca, S. Mezzari, T. Maluta, E. Luminari, F. Perusi, E. Vecchini, B. MagnanTefera LeteboNo ratings yet
- Simpson 2017Document9 pagesSimpson 2017saimanojkosuriNo ratings yet
- Pathogenesis and Management of Fracture-Related InfectionDocument7 pagesPathogenesis and Management of Fracture-Related InfectionJeremi SetiawanNo ratings yet
- Diagnosis and Management of Osteomyelitis: Gunawan, B SetiyohadiDocument5 pagesDiagnosis and Management of Osteomyelitis: Gunawan, B SetiyohadiAndre PhanNo ratings yet
- Complications of Frontal Sinus Fractures: Stephen E. Metzinger, M.D., F.A.C.S., and Rebecca C. Metzinger, M.DDocument8 pagesComplications of Frontal Sinus Fractures: Stephen E. Metzinger, M.D., F.A.C.S., and Rebecca C. Metzinger, M.DYohana SepthiyaNo ratings yet
- Diagnostics 12 01289Document15 pagesDiagnostics 12 01289Sushmica BaquiranNo ratings yet
- Complications of The Surgical Treatment of Fractures of The Tibial Plateau Prevalence, Causes, and ManagementDocument15 pagesComplications of The Surgical Treatment of Fractures of The Tibial Plateau Prevalence, Causes, and ManagementraynaldidjohariofcNo ratings yet
- Tibial No UnionDocument8 pagesTibial No Unionjuan pagesNo ratings yet
- Presentasi PABI Pekanbaru 2021Document20 pagesPresentasi PABI Pekanbaru 2021raudhatul muttaqinNo ratings yet
- 2008 Classification and Management of Acute WoundsDocument5 pages2008 Classification and Management of Acute WoundsMiguel Angel Carrasco MedinaNo ratings yet
- Pathophysiology: Laboratory StudiesDocument8 pagesPathophysiology: Laboratory Studiesrahma perwitasariNo ratings yet
- Implant Es 1Document8 pagesImplant Es 1Karla AlanisNo ratings yet
- Cement Beads and Cement Spa Indications,.3Document6 pagesCement Beads and Cement Spa Indications,.3Erika LlorenNo ratings yet
- DAIRDocument12 pagesDAIRCris JiménezNo ratings yet
- Inflamacion y Blance Inmunologico en Implantologia 2019Document7 pagesInflamacion y Blance Inmunologico en Implantologia 2019Javier Figueroa FuentesNo ratings yet
- The International Journal of Periodontics & Restorative DentistryDocument10 pagesThe International Journal of Periodontics & Restorative DentistryGerard GonzalezNo ratings yet
- Mohomad Al-Sawah, Guy Richard Pupp, DPM, FACFAS : DPM Priya Samant, DPM Dustan Mascarenhas, MDDocument1 pageMohomad Al-Sawah, Guy Richard Pupp, DPM, FACFAS : DPM Priya Samant, DPM Dustan Mascarenhas, MDbaoNo ratings yet
- Peri Implant Disease PDFDocument32 pagesPeri Implant Disease PDFHajra FarooqNo ratings yet
- Harrsion 1991 PDFDocument8 pagesHarrsion 1991 PDFrozh rasulNo ratings yet
- Bioengineering 11 00357Document15 pagesBioengineering 11 00357Shahmeer HassanNo ratings yet
- Implant ComplicationsDocument66 pagesImplant ComplicationsVivek LathNo ratings yet
- Mantenimiento de ImplanteDocument6 pagesMantenimiento de ImplanteCris JiménezNo ratings yet
- Evolution in Management of Tibial Pilon FracturesDocument9 pagesEvolution in Management of Tibial Pilon FracturestripodegrandeNo ratings yet
- Dental Implants: Maintenance, Care and Treatment of Peri-Implant InfectionDocument9 pagesDental Implants: Maintenance, Care and Treatment of Peri-Implant Infectionالعمري العمريNo ratings yet
- EBP EONSMalignantFungatingWoundsDocument30 pagesEBP EONSMalignantFungatingWoundsNaoval Meilandi Nurjaman100% (1)
- Acute Wound Management: Revisiting The Approach To Assessment, Irrigation, and Closure ConsiderationsDocument9 pagesAcute Wound Management: Revisiting The Approach To Assessment, Irrigation, and Closure ConsiderationsOscar Alexis Jiménez ViverosNo ratings yet
- Different Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowDocument6 pagesDifferent Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowMadhuchandra HirehalliNo ratings yet
- Wound InfectionDocument6 pagesWound InfectionCatarina DiasNo ratings yet
- Sub-Trochanteric Femoral Fractures: Challenges and SolutionsDocument7 pagesSub-Trochanteric Femoral Fractures: Challenges and SolutionsJanethNo ratings yet
- Management of Aseptic Tibial NonunionDocument11 pagesManagement of Aseptic Tibial NonunionJawad KhanNo ratings yet
- Patzakis Open Fracture Management PDFDocument15 pagesPatzakis Open Fracture Management PDFNurul AtiahNo ratings yet
- Inflammation, Bone Healing and OsteonecrosisDocument11 pagesInflammation, Bone Healing and OsteonecrosislliuyueeNo ratings yet
- Infection: Long Bone Osteomyelitis in Adults: Fundamental Concepts and Current TechniquesDocument7 pagesInfection: Long Bone Osteomyelitis in Adults: Fundamental Concepts and Current TechniquesAdriana NavaNo ratings yet
- Surgical Techniques ToDocument9 pagesSurgical Techniques Toalkhalijia dentalNo ratings yet
- Research Reports in Oral and Maxillofacial Surgery Rroms 5 055Document10 pagesResearch Reports in Oral and Maxillofacial Surgery Rroms 5 055aguunggpNo ratings yet
- Modes of Failure of Proximal Femoral Nail (PFN) in Unstable Trochanteric FracturesDocument10 pagesModes of Failure of Proximal Femoral Nail (PFN) in Unstable Trochanteric FracturesSrikanthNo ratings yet
- The Incidence of Infection in Open Cruris FractureDocument3 pagesThe Incidence of Infection in Open Cruris FractureArif DanuartaNo ratings yet
- Deigiudici2016 231022 130836Document7 pagesDeigiudici2016 231022 130836Cristian SanchezNo ratings yet
- Fcimb 12 908859Document17 pagesFcimb 12 908859ShivangiJainNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Dislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementFrom EverandDislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementNigel Shaun MatthewsNo ratings yet
- Safe Zone For Anterior Retractor Placement in Total HipDocument5 pagesSafe Zone For Anterior Retractor Placement in Total HipFilip starcevicNo ratings yet
- Prospective 5-Year Study With 96 Short Curved Fitmore ™ Hip Stems Shows A High Incidence of Cortical Hypertrophy With No Clinical RelevanceDocument9 pagesProspective 5-Year Study With 96 Short Curved Fitmore ™ Hip Stems Shows A High Incidence of Cortical Hypertrophy With No Clinical RelevanceFilip starcevicNo ratings yet
- Evaluation of The Painful Total Knee Arthroplasty.99377Document9 pagesEvaluation of The Painful Total Knee Arthroplasty.99377Filip starcevic100% (1)
- Jkfs 32 102Document5 pagesJkfs 32 102Filip starcevicNo ratings yet
- Fox News Seeks Cost Against WASHLITEDocument5 pagesFox News Seeks Cost Against WASHLITELaw&Crime0% (1)
- Planning, Design, Construction and RehabilitationDocument440 pagesPlanning, Design, Construction and RehabilitationMilica BebinaNo ratings yet
- Prayer LetterDocument9 pagesPrayer LetterJohnNo ratings yet
- Pandaigdigang AkdaDocument46 pagesPandaigdigang AkdatheaeahNo ratings yet
- Reign of Terror DBQ Packet Answers 2Document38 pagesReign of Terror DBQ Packet Answers 2salgado.sNo ratings yet
- Bios Life Slim UAEDocument4 pagesBios Life Slim UAEJey BautistaNo ratings yet
- Philsec Investment v. CA (GR. No. 103493. June 19, 1997)Document15 pagesPhilsec Investment v. CA (GR. No. 103493. June 19, 1997)Mayjolica AgunodNo ratings yet
- Part-ORA Subparts GEN and ATO: Workshop On Reg. 1178/2011 and 290/2012 Lisbon, PortugalDocument51 pagesPart-ORA Subparts GEN and ATO: Workshop On Reg. 1178/2011 and 290/2012 Lisbon, PortugalMário MineiroNo ratings yet
- The Empty DrumDocument1 pageThe Empty DrumMina Kumari SinghNo ratings yet
- Renaissance and ReformationDocument21 pagesRenaissance and ReformationVictoria MonacelliNo ratings yet
- G8 Group - Versatile - Topic - Ethics and Basic Principles Governing An Audit - Leader - MD Emran Mia PDFDocument13 pagesG8 Group - Versatile - Topic - Ethics and Basic Principles Governing An Audit - Leader - MD Emran Mia PDFTanjin keyaNo ratings yet
- 1ST and 2ND Level AssessmentDocument2 pages1ST and 2ND Level AssessmentKathleen Nichole PatocNo ratings yet
- Baroid (Waste Management)Document30 pagesBaroid (Waste Management)Maychel Wibowo100% (1)
- Putting The Balanced ScorecardDocument12 pagesPutting The Balanced ScorecardArnabNo ratings yet
- Spice Model Laser Diode 15diDocument8 pagesSpice Model Laser Diode 15diParker333100% (1)
- CanastaDocument4 pagesCanastaPrincess DaisyNo ratings yet
- Effects of Total Plasma Protein ConcentrDocument4 pagesEffects of Total Plasma Protein ConcentrThuy NguyenNo ratings yet
- Act No 2031 NILDocument30 pagesAct No 2031 NILHp AmpsNo ratings yet
- Class 10Document9 pagesClass 10Vijay GuptaNo ratings yet
- 2841 A Watermark For Large LanguageDocument24 pages2841 A Watermark For Large LanguageAdithyaNo ratings yet
- Grade-8 (Science) Third QuarterDocument1 pageGrade-8 (Science) Third Quartertrexia autidaNo ratings yet
- Relationscapes Movement Art Philosophy by Erin Manning 2009 Cambridge Ma The Mit Press X 268 PP Images Notes Bibliography Index Dollar3200 HardcoverDocument4 pagesRelationscapes Movement Art Philosophy by Erin Manning 2009 Cambridge Ma The Mit Press X 268 PP Images Notes Bibliography Index Dollar3200 HardcoverHonglan HuangNo ratings yet
- The Cancel Culture: Baluyos - EncaboDocument17 pagesThe Cancel Culture: Baluyos - EncaboibantoyNo ratings yet
- Principles of Learning and Motivation p11Document3 pagesPrinciples of Learning and Motivation p11Wilson Jan AlcopraNo ratings yet