Download as pdf or txt
You might also like
- Philhealth Request LetterDocument2 pagesPhilhealth Request LetterKilaine Montilla92% (13)
- Memorial Hermann Discharge Papers - 3Document5 pagesMemorial Hermann Discharge Papers - 3Alaska JamesNo ratings yet
- BADAC Template - Executive OrderDocument5 pagesBADAC Template - Executive OrderDona JojuicoNo ratings yet
- MSI Health Card Renewal FormDocument1 pageMSI Health Card Renewal Formdohudohu2100% (1)
- Osha3788 PDFDocument2 pagesOsha3788 PDFoscarvega1029No ratings yet
- How To Request Your Covid - 19 Lab Report: Complete The Consent To Disclose Phi FormDocument3 pagesHow To Request Your Covid - 19 Lab Report: Complete The Consent To Disclose Phi FormAnithasree SrinivasanNo ratings yet
- Authorization For Receipt of Medical RecordDocument1 pageAuthorization For Receipt of Medical Recordmayreddy.anushaNo ratings yet
- Authorization of Release Medical Records/ Information Patient Name/s Dob: Dob: Dob: DobDocument1 pageAuthorization of Release Medical Records/ Information Patient Name/s Dob: Dob: Dob: DobTyler FarrNo ratings yet
- Official Medical Information and Release FormDocument2 pagesOfficial Medical Information and Release FormtheNOLAtreeNo ratings yet
- Patient Demographics 12-12-12Document4 pagesPatient Demographics 12-12-12api-233056868No ratings yet
- Reimbursement Claim - Claimants Statement - FinalDocument3 pagesReimbursement Claim - Claimants Statement - Finalsanyogitasawant5No ratings yet
- Request For Patient Records and Information or Authorization For Release1Document1 pageRequest For Patient Records and Information or Authorization For Release1akcabhay9No ratings yet
- Authorization FormDocument1 pageAuthorization FormRD Finders and Personal TrainingNo ratings yet
- Hipaa Release Form FloridaDocument3 pagesHipaa Release Form FloridaAlan WattsNo ratings yet
- Kansas State Board of Healing Arts: Complaint FormDocument4 pagesKansas State Board of Healing Arts: Complaint FormbgsradNo ratings yet
- Patient Registration Form 13Document4 pagesPatient Registration Form 13windawaty humolaNo ratings yet
- DHS DHS: Dedicated Healthcare Services (India) Private LimitedDocument1 pageDHS DHS: Dedicated Healthcare Services (India) Private Limiteddisk_la_poduNo ratings yet
- Records ReleaseDocument1 pageRecords ReleasechelseaNo ratings yet
- Adult NP Ppwrork KCPGDocument16 pagesAdult NP Ppwrork KCPGMary GreerNo ratings yet
- Phil HealthDocument1 pagePhil HealthLorence WarrenNo ratings yet
- Clinical Information Services Authorization For Disclosure ofDocument2 pagesClinical Information Services Authorization For Disclosure ofRIchard RobertsNo ratings yet
- Long Course RegistrationDocument1 pageLong Course RegistrationCFYN TigersharksNo ratings yet
- Pass Plan Request Form (Template)Document2 pagesPass Plan Request Form (Template)brooklynn.poitrasNo ratings yet
- Maxicare Maintenance FormDocument1 pageMaxicare Maintenance FormEdd Nysha ManguilimotanNo ratings yet
- Axa Mansard Health Corporate Form - Nathan Ayomide OriaifoDocument1 pageAxa Mansard Health Corporate Form - Nathan Ayomide OriaifoIsiNo ratings yet
- BSB FORM NO. 2-B - Application For Medical or Hospital AssistanceDocument1 pageBSB FORM NO. 2-B - Application For Medical or Hospital AssistanceRudejane TanNo ratings yet
- Chiropractic Application Form: Section A: Contact InformationDocument6 pagesChiropractic Application Form: Section A: Contact InformationAmanakeNo ratings yet
- Insurance Direct Billing Submission Fillable FormDocument2 pagesInsurance Direct Billing Submission Fillable FormAfreen FathimaNo ratings yet
- UVMC-Amendment Request FormDocument1 pageUVMC-Amendment Request FormMuhammad RosliNo ratings yet
- Medical Marijuana - ChangerequestformDocument2 pagesMedical Marijuana - Changerequestform420No ratings yet
- 14) ELIB-Female CI-Claim FormDocument7 pages14) ELIB-Female CI-Claim Formbibianna93No ratings yet
- Release of InformationDocument2 pagesRelease of Informationxstn15No ratings yet
- New Patient FormDocument7 pagesNew Patient FormajNo ratings yet
- Medical Marijuana - ApplicationformDocument2 pagesMedical Marijuana - Applicationform420100% (3)
- Refusal FormDocument1 pageRefusal FormViral Chann3LNo ratings yet
- Willits Otters Swim Team ApplicationDocument2 pagesWillits Otters Swim Team Applicationapi-423839129No ratings yet
- Request Letter 2 PDFDocument1 pageRequest Letter 2 PDFAnna Rose C. AlcazarenNo ratings yet
- Request Letter 2Document1 pageRequest Letter 2Rose Ann R. AbenidoNo ratings yet
- Name of Health Care Provider / Plan / Other/ Myself Address: (Please Fill in Below)Document1 pageName of Health Care Provider / Plan / Other/ Myself Address: (Please Fill in Below)Jennifer walNo ratings yet
- Health Records Miis-Immunization Record RequestDocument2 pagesHealth Records Miis-Immunization Record RequestHongyu ZhouNo ratings yet
- AR PDF-Authorization For Release Vet RecordsDocument1 pageAR PDF-Authorization For Release Vet RecordsbaxterinathetrollNo ratings yet
- JF Elite Plus Student Insurance Claim Form: ImportantDocument2 pagesJF Elite Plus Student Insurance Claim Form: ImportantJayesh GoplaniNo ratings yet
- New Patient Information Form PrintableDocument3 pagesNew Patient Information Form PrintableXyzNo ratings yet
- HIPAADocument1 pageHIPAAwade_takenishiddsNo ratings yet
- Request Form Service Record and CoeDocument2 pagesRequest Form Service Record and CoeARIEN ACAMPADONo ratings yet
- SwimmingPool Membership FormDocument1 pageSwimmingPool Membership FormSrujana MohantyNo ratings yet
- 2009 - Camp - Workshop - Medical - Authorization - Form - Rev. 1Document1 page2009 - Camp - Workshop - Medical - Authorization - Form - Rev. 1api-3699829No ratings yet
- Urgentcare FormDocument4 pagesUrgentcare Formapi-287654333No ratings yet
- SPC - Intake Form and POA Requires NotaryDocument2 pagesSPC - Intake Form and POA Requires NotaryVanessa Collins SimmsNo ratings yet
- Mountaineer Vision Center, PLLC: Do You Have Any of The Following Medical Conditions?Document5 pagesMountaineer Vision Center, PLLC: Do You Have Any of The Following Medical Conditions?doug_trovingerNo ratings yet
- Financial Assistance Claims Reimbursement Form 1Document1 pageFinancial Assistance Claims Reimbursement Form 1Ralph Ian LuyoNo ratings yet
- Request FormDocument2 pagesRequest FormGloriefe MeniosaNo ratings yet
- Authorization To Release InformationDocument1 pageAuthorization To Release InformationMalita CortilasNo ratings yet
- Mass IMMUNIZATION RECORD Request FormDocument3 pagesMass IMMUNIZATION RECORD Request Formwarriorsinrecoveryalex.rNo ratings yet
- 2013-2014 Returning Medical FormDocument10 pages2013-2014 Returning Medical FormKevin WangNo ratings yet
- Mifflintown Hose Co. #1: Volunteer ApplicationDocument8 pagesMifflintown Hose Co. #1: Volunteer ApplicationKeith H. BoremanNo ratings yet
- Earnings Release 82508 (1) - MarkDocument1 pageEarnings Release 82508 (1) - MarkTerry PetersonNo ratings yet
- CLAIMS 008 1022 7 Certificate of ClaimantDocument3 pagesCLAIMS 008 1022 7 Certificate of ClaimantEmsNo ratings yet
- EARISTians Portfolio 2023Document1 pageEARISTians Portfolio 2023Bea DulaNo ratings yet
- Claim FormDocument3 pagesClaim FormSumit ManglaniNo ratings yet
- New Patient Forms DigitalDocument5 pagesNew Patient Forms Digitalkarelen araujoNo ratings yet
- Proof of Payment ReportDocument1 pageProof of Payment Reportapi-676582318No ratings yet
- Estatement 2Document2 pagesEstatement 2api-676582318No ratings yet
- Nov 21 2019 Form 42 and 1Document10 pagesNov 21 2019 Form 42 and 1api-676582318No ratings yet
- Notice of Reassessment 2021 08 16 06 13 55 692252Document4 pagesNotice of Reassessment 2021 08 16 06 13 55 692252api-676582318No ratings yet
- Notice of Assessment 2022 03 17 11 16 57 195191Document4 pagesNotice of Assessment 2022 03 17 11 16 57 195191api-676582318No ratings yet
- Notice of Reassessment 2021 05 31 09 31 59 853056Document4 pagesNotice of Reassessment 2021 05 31 09 31 59 853056api-676582318No ratings yet
- Nov 21 2019 ADocument25 pagesNov 21 2019 Aapi-676582318No ratings yet
- Notice of Reassessment 2021 08 16 06 14 40 172371Document4 pagesNotice of Reassessment 2021 08 16 06 14 40 172371api-676582318No ratings yet
- Toronto Police Report RecordsDocument248 pagesToronto Police Report Recordsapi-676582318No ratings yet
- September 14 2019 BDocument30 pagesSeptember 14 2019 Bapi-676582318No ratings yet
- Oct 27 2017 2Document2 pagesOct 27 2017 2api-676582318No ratings yet
- Nov 21 2019 CDocument23 pagesNov 21 2019 Capi-676582318No ratings yet
- Nghiem Phuoc 109121 0601Document11 pagesNghiem Phuoc 109121 0601api-676582318No ratings yet
- Condo 2000aDocument1 pageCondo 2000aapi-676582318No ratings yet
- 0ct 27 2017 1Document4 pages0ct 27 2017 1api-676582318No ratings yet
- Sept 4 2017 2Document5 pagesSept 4 2017 2api-676582318No ratings yet
- Form 2 August 7 2020Document6 pagesForm 2 August 7 2020api-676582318No ratings yet
- Form 2 2020 August 7Document3 pagesForm 2 2020 August 7api-676582318No ratings yet
- Oct 27 2017 3Document5 pagesOct 27 2017 3api-676582318No ratings yet
- H 1446022Document3 pagesH 1446022api-676582318No ratings yet
- July 6 2017 2Document15 pagesJuly 6 2017 2api-676582318No ratings yet
- Sept 4 2017 3Document6 pagesSept 4 2017 3api-676582318No ratings yet
- Results - Doan Nghiem - Soft-CheckDocument4 pagesResults - Doan Nghiem - Soft-Checkapi-676582318No ratings yet
- Sept 4 2017 1Document1 pageSept 4 2017 1api-676582318No ratings yet
- March 28 2017 Fake Parents Gave Statment at HospitalDocument5 pagesMarch 28 2017 Fake Parents Gave Statment at Hospitalapi-676582318No ratings yet
- March 28 2017 Hospital Given Statements by Parents While in in The Rectangle ZoneDocument6 pagesMarch 28 2017 Hospital Given Statements by Parents While in in The Rectangle Zoneapi-676582318No ratings yet
- March 28 2017 Frame For Being On Form Ordered Form 2 2Document11 pagesMarch 28 2017 Frame For Being On Form Ordered Form 2 2api-676582318No ratings yet
- Power GridDocument16 pagesPower GridSandhya VairageNo ratings yet
- Aff of Undertaking Floor PlanDocument2 pagesAff of Undertaking Floor PlanTet LegaspiNo ratings yet
- Resume Const Mang FinalDocument3 pagesResume Const Mang Finalapi-291556059No ratings yet
- Country Report 2022 KAZDocument41 pagesCountry Report 2022 KAZJohnson JamesNo ratings yet
- Training Communications Organizational Manager in San Francisco Bay CA Resume Susyn AlmondDocument3 pagesTraining Communications Organizational Manager in San Francisco Bay CA Resume Susyn AlmondSusynAlmondNo ratings yet
- Health Law OutlineDocument38 pagesHealth Law OutlinemmaattttNo ratings yet
- Passive Euthanasia Draft Bill - Voice of Indian DoctorsDocument34 pagesPassive Euthanasia Draft Bill - Voice of Indian Doctorsrohan14185No ratings yet
- Bangalore PPN Hospital - ProcedureDocument16 pagesBangalore PPN Hospital - Procedureneeraj_ghs679No ratings yet
- DisciplineDocument11 pagesDisciplineAnusha Verghese100% (7)
- CGHS Enclosure 1Document77 pagesCGHS Enclosure 1bhupendrapawar279No ratings yet
- LBSM Calendar Year 09Document154 pagesLBSM Calendar Year 09Rachel E. Stassen-BergerNo ratings yet
- Hospital Choice Factors - TurkeyDocument18 pagesHospital Choice Factors - TurkeywintannNo ratings yet
- Reduced Canada Bay DRAFT Open Space and Recreation Strategy 190515Document136 pagesReduced Canada Bay DRAFT Open Space and Recreation Strategy 190515DorjeNo ratings yet
- Example Proposal 1Document4 pagesExample Proposal 1Rhon Mhay VirgoNo ratings yet
- Licence Application: (You Must Live in NSW To Be Issued With A NSW Licence)Document4 pagesLicence Application: (You Must Live in NSW To Be Issued With A NSW Licence)SebastianNo ratings yet
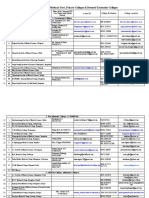
- Medical and Dental Colleges PH No. and e Mail Id ListDocument5 pagesMedical and Dental Colleges PH No. and e Mail Id ListYash RajNo ratings yet
- Philippine Health Insurance Corporation: Citystate Centre, 709 Shaw Boulevard, Pasig CityDocument10 pagesPhilippine Health Insurance Corporation: Citystate Centre, 709 Shaw Boulevard, Pasig CityJhosie GirayNo ratings yet
- Red Cross Group 4 Service Learning Poster-海报Document1 pageRed Cross Group 4 Service Learning Poster-海报Xie HangchenNo ratings yet
- AP Medical/Dental/AYUSH Admissions - 2020-21 Competent Authority Quota Provisional Verification ReportDocument1 pageAP Medical/Dental/AYUSH Admissions - 2020-21 Competent Authority Quota Provisional Verification ReportRajesh ToluchuriNo ratings yet
- Austroads Guide To Bridge Technology Part 7 - Maintenance and Management of Existing BridgesDocument335 pagesAustroads Guide To Bridge Technology Part 7 - Maintenance and Management of Existing Bridgestoddlbyrnes100% (1)
- Parents Welfare Act After It Lapsed Into LawDocument2 pagesParents Welfare Act After It Lapsed Into LawCarmel LouiseNo ratings yet
- Whip SpeechesDocument22 pagesWhip SpeechesJoicey CatamioNo ratings yet
- Public-Fiscal-Admin Syllabus DrLMVicencio FinalDocument8 pagesPublic-Fiscal-Admin Syllabus DrLMVicencio FinaltullasjuriNo ratings yet
- Community Health NursingLectureDocument40 pagesCommunity Health NursingLectureMJCNo ratings yet
- Whistleblower Lawsuit, KU HospitalDocument17 pagesWhistleblower Lawsuit, KU HospitalIan CummingsNo ratings yet
- Salary ScheduleDocument8 pagesSalary ScheduleJo AlzNo ratings yet
- PW379Document3 pagesPW379Greg MavhungaNo ratings yet
- Professional Regulation Commission: Republic of The Philippines ManilaDocument4 pagesProfessional Regulation Commission: Republic of The Philippines ManilaTheSummitExpressNo ratings yet