Download as pdf or txt
You might also like
- Ictal and Postictal Psychiatric Disturbances - TrimbleDocument5 pagesIctal and Postictal Psychiatric Disturbances - Trimblegoo99No ratings yet
- Dr. Reckeweg Reference Guide - United RemediesDocument4 pagesDr. Reckeweg Reference Guide - United RemediesshubhamformeNo ratings yet
- Ictal and Peri-Ictal Psychopathology: Marco Mula and Francesco MonacoDocument6 pagesIctal and Peri-Ictal Psychopathology: Marco Mula and Francesco MonacoJonathan DavisNo ratings yet
- Epilspia y Comobilidad PsiquiatricaDocument17 pagesEpilspia y Comobilidad PsiquiatricaManuel Alejandro Pinzon OlmosNo ratings yet
- Management of Psychogenic Nonepileptic SeizuresDocument3 pagesManagement of Psychogenic Nonepileptic SeizuresRudolph MuliawanNo ratings yet
- Psychiatric Disorders Associated With EpilepsyDocument18 pagesPsychiatric Disorders Associated With EpilepsyAllan DiasNo ratings yet
- Conversion Disorder: The Brain's Way of Dealing With Psychological Conflicts. Case Report of A Patient With Non-Epileptic SeizuresDocument7 pagesConversion Disorder: The Brain's Way of Dealing With Psychological Conflicts. Case Report of A Patient With Non-Epileptic SeizuresMaria Von Shaft100% (1)
- Epilepsy and Psychiatric DisordersDocument7 pagesEpilepsy and Psychiatric DisordersAlejandro QuinteroNo ratings yet
- Psychiatric Disorders in Epilepsy - Chapter16 - Foong2015Document4 pagesPsychiatric Disorders in Epilepsy - Chapter16 - Foong2015BirhanuNo ratings yet
- Post-Traumatic Epilepsy (JNCN 2014-Summer)Document6 pagesPost-Traumatic Epilepsy (JNCN 2014-Summer)skyclad_21No ratings yet
- Psychiatric Aspects of Epilepsy: A Review: InroductionDocument6 pagesPsychiatric Aspects of Epilepsy: A Review: InroductionAdam MochtarNo ratings yet
- Psychogenic Stroke A Case ReportDocument4 pagesPsychogenic Stroke A Case Reporteditorial.boardNo ratings yet
- CTP NotesDocument8 pagesCTP Notesrupangishah7No ratings yet
- Interictal Psychosis - A Case of Psychosis of EpilepsyDocument3 pagesInterictal Psychosis - A Case of Psychosis of EpilepsyJAVED ATHER SIDDIQUINo ratings yet
- Psychogenic VertigoDocument4 pagesPsychogenic VertigoLenny SulystioNo ratings yet
- L 8 NewDocument13 pagesL 8 NewWeronika Tomaszczuk-KłakNo ratings yet
- Michiel Sen 2017Document1 pageMichiel Sen 2017Muhammad IlhaamNo ratings yet
- EpilepsiaManifestaciones Psicologicas de La Epilepsia en La Infancia DR Juan Luis Moya HLCMDocument7 pagesEpilepsiaManifestaciones Psicologicas de La Epilepsia en La Infancia DR Juan Luis Moya HLCMeducacionchileNo ratings yet
- Mental Health Perspectives of Epilepsy: Focus On Anxiety DisordersDocument9 pagesMental Health Perspectives of Epilepsy: Focus On Anxiety DisorderserikafebriyanarNo ratings yet
- Neuropsicologia de La EpilepsiaDocument12 pagesNeuropsicologia de La Epilepsiaanon_809668623100% (1)
- Status Epilepticus Work-Up and Management in AdultsDocument9 pagesStatus Epilepticus Work-Up and Management in AdultsAnonymous QLadTClydkNo ratings yet
- The Psychiatric Comorbidity of Epilepsy PDFDocument14 pagesThe Psychiatric Comorbidity of Epilepsy PDFTanjung E SumekarNo ratings yet
- FTD Psychiatric DDDocument11 pagesFTD Psychiatric DDlaraviNo ratings yet
- Assessment of The Quality of Life of Young Men Suffering From EpilepsyDocument3 pagesAssessment of The Quality of Life of Young Men Suffering From EpilepsyHerald Scholarly Open AccessNo ratings yet
- EpilepsieDocument19 pagesEpilepsieFlorin Calin LungNo ratings yet
- Whr01 Fact Sheet1 enDocument4 pagesWhr01 Fact Sheet1 enlala_bojaNo ratings yet
- Original Paper Comorbidity of Epilepsy and Depression in Al Husseini Teaching Hospital in Holy Kerbala /iraq in 2018Document9 pagesOriginal Paper Comorbidity of Epilepsy and Depression in Al Husseini Teaching Hospital in Holy Kerbala /iraq in 2018sarhang talebaniNo ratings yet
- Epilepsy & Behavior: Andres M. KannerDocument3 pagesEpilepsy & Behavior: Andres M. KannerIzara Maité Mondragón MorenoNo ratings yet
- Neurobiology of SchizophreniaDocument11 pagesNeurobiology of SchizophreniaJerry JacobNo ratings yet
- CHAPTER 50 CLINICAL SPECTRUM - Baulac - 2007Document8 pagesCHAPTER 50 CLINICAL SPECTRUM - Baulac - 2007Natasha MarksNo ratings yet
- Abdulsalam Mohammed Yakasai Physiotherapy Intervention in Children With EpiDocument17 pagesAbdulsalam Mohammed Yakasai Physiotherapy Intervention in Children With Epinaveen chaudharyNo ratings yet
- Neuropsychiatric Symptoms of Multiple Sclerosis - State of The ArtDocument12 pagesNeuropsychiatric Symptoms of Multiple Sclerosis - State of The ArtRenato GuedesNo ratings yet
- Manual para No Morir de AmorDocument34 pagesManual para No Morir de AmorArgenis SalinasNo ratings yet
- Epilepsy DR LindaDocument8 pagesEpilepsy DR LindaLaylaNo ratings yet
- 10 1016@j Paed 2020 06 003 PDFDocument5 pages10 1016@j Paed 2020 06 003 PDFCarlos MichasNo ratings yet
- Amboni 2010Document7 pagesAmboni 2010Marcela Paz GazmuriNo ratings yet
- Health HX&SBARDocument6 pagesHealth HX&SBARMary Rose Silva GargarNo ratings yet
- Hingray 2016Document7 pagesHingray 2016syrieuxNo ratings yet
- Tolchin2020 Neurop. Epilepsia 2020Document16 pagesTolchin2020 Neurop. Epilepsia 2020Carolina MuñozNo ratings yet
- Organic Brain SyndromeDocument10 pagesOrganic Brain SyndromeJavaid IqbalNo ratings yet
- Seizure - NCBIDocument9 pagesSeizure - NCBILaura Campos ModestoNo ratings yet
- Conversion Disorder: Etiology/ Causal FactorsDocument4 pagesConversion Disorder: Etiology/ Causal FactorsSrishti GaurNo ratings yet
- Author 'S Accepted Manuscript: 10.1016/j.psym.2016.05.005Document40 pagesAuthor 'S Accepted Manuscript: 10.1016/j.psym.2016.05.005jose luisNo ratings yet
- Introduction Ped EpilepsyDocument15 pagesIntroduction Ped EpilepsyD PharmaNo ratings yet
- BMJ Article 2Document7 pagesBMJ Article 2aruna kakiNo ratings yet
- Epilepsy & Behavior: A B B C D D D D A e A e A e FDocument9 pagesEpilepsy & Behavior: A B B C D D D D A e A e A e FKamel BourasNo ratings yet
- Authortest, Musaib-AliDocument3 pagesAuthortest, Musaib-AliShadrackNo ratings yet
- The Psychosis of EpilepsyDocument4 pagesThe Psychosis of EpilepsyAlphSeanNo ratings yet
- Encefalitis Autoinmune 2Document9 pagesEncefalitis Autoinmune 2Alejandro PiscitelliNo ratings yet
- 285 FullDocument7 pages285 FullfranciscoNo ratings yet
- 10 11648 J Ajp 20220802 15Document9 pages10 11648 J Ajp 20220802 15Roberto SoehartonoNo ratings yet
- 2015 Juri CognitionintheearlystagesofadultepilepsyDocument4 pages2015 Juri CognitionintheearlystagesofadultepilepsyManuel CarreonNo ratings yet
- Epilepsy PDFDocument15 pagesEpilepsy PDFMohamedErrmaliNo ratings yet
- Dissociative Amnesia Disorder - Kaplan & Sadock Synopsis of PsychiatryDocument4 pagesDissociative Amnesia Disorder - Kaplan & Sadock Synopsis of PsychiatryGian GiananNo ratings yet
- Epilepsy and Associated ComorbiditiesDocument3 pagesEpilepsy and Associated ComorbiditiesVictor Martin PeresNo ratings yet
- The Epidemiology of Epilepsy: ReviewDocument7 pagesThe Epidemiology of Epilepsy: ReviewArnaldo Pérez SellésNo ratings yet
- Epilepsia - 2007 - Nadkarni - Psychosis in Epilepsy PatientsDocument3 pagesEpilepsia - 2007 - Nadkarni - Psychosis in Epilepsy PatientsMichael UNo ratings yet
- Avaliação e Manejo de Convulsões Agudas em CriançasDocument11 pagesAvaliação e Manejo de Convulsões Agudas em CriançasMaiquiel MaiaNo ratings yet
- Hmed 2011 72 Sup6 M88Document4 pagesHmed 2011 72 Sup6 M88yakiniku10eNo ratings yet
- Examination of The Respiratory SystemDocument12 pagesExamination of The Respiratory SystemChris Jardine LiNo ratings yet
- Manjula PDocument6 pagesManjula PRanjani PNo ratings yet
- Department of Molecular Virology: COVID-19 (Corona) VirusDocument1 pageDepartment of Molecular Virology: COVID-19 (Corona) Virusshoaib chNo ratings yet
- Marilyne M. Lange, Cornelis J. H. van de Velde (auth.), Vincenzo Valentini, Hans-Joachim Schmoll, Cornelis J. H. van de Velde (eds.)-Multidisciplinary Management of Rectal Cancer_ Questions and Answer.pdfDocument354 pagesMarilyne M. Lange, Cornelis J. H. van de Velde (auth.), Vincenzo Valentini, Hans-Joachim Schmoll, Cornelis J. H. van de Velde (eds.)-Multidisciplinary Management of Rectal Cancer_ Questions and Answer.pdfIrinaMariaStrugari100% (1)
- Evidence Based Practice On Typhoid FeverDocument22 pagesEvidence Based Practice On Typhoid FeverRhia CortezNo ratings yet
- 05a Aravind Eye Hospital, Madurai, IndiaDocument4 pages05a Aravind Eye Hospital, Madurai, IndiaSubhadra HaribabuNo ratings yet
- Low-Flow Acute Kidney InjuryDocument11 pagesLow-Flow Acute Kidney InjuryJuan Manuel Lopez VargasNo ratings yet
- Urinary Diversions UrostomyDocument15 pagesUrinary Diversions Urostomymardsz100% (3)
- Circulating Case Slip: Name of Student Student NumberDocument12 pagesCirculating Case Slip: Name of Student Student NumberEugenio Roque Casaclang De Leon IiiNo ratings yet
- A-Plus Multi Criticalcare Brochure Full 20130529 FinalDocument14 pagesA-Plus Multi Criticalcare Brochure Full 20130529 Finalnusthe2745No ratings yet
- Case Study 3, Female Genital Mutilation (FGM)Document4 pagesCase Study 3, Female Genital Mutilation (FGM)Mikaela Joy GreganaNo ratings yet
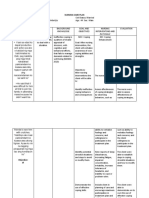
- Nursing Care Plan: RationaleDocument3 pagesNursing Care Plan: Rationaleimnas100% (1)
- Acute Post-Surgical Pain Management: A Critical Appraisal of Current PracticeDocument42 pagesAcute Post-Surgical Pain Management: A Critical Appraisal of Current PracticeMmenyeneNo ratings yet
- Cedera KepalaDocument102 pagesCedera KepalaNesaNo ratings yet
- Clinical Assessment and Treatment of Attention Deficit Hyperactivity Disorder in AdultsDocument15 pagesClinical Assessment and Treatment of Attention Deficit Hyperactivity Disorder in Adults733No ratings yet
- Enlarged Uvula Causes and TreatmentDocument6 pagesEnlarged Uvula Causes and TreatmentMoinul HaqueNo ratings yet
- Collection of Quotes After NeurolepticsDocument30 pagesCollection of Quotes After NeurolepticsMarcos WrightNo ratings yet
- Diabetes and ExerciseDocument12 pagesDiabetes and ExercisePranav SNo ratings yet
- Atypical PneumoniaDocument30 pagesAtypical PneumoniachandanNo ratings yet
- M G Jedar2012.PDF (PDFDrive)Document190 pagesM G Jedar2012.PDF (PDFDrive)Vrushabh DharmikNo ratings yet
- Distribution of Causes of Abnormal Uterine Bleeding Using The New FIGO Classification SystemDocument3 pagesDistribution of Causes of Abnormal Uterine Bleeding Using The New FIGO Classification SystemirmaarmiyahNo ratings yet
- Relationship Between Temporomandibular Joint Disorders and Body PostureDocument8 pagesRelationship Between Temporomandibular Joint Disorders and Body PostureCiceu Voicu100% (1)
- GAD With Info SheetDocument4 pagesGAD With Info SheetEM RiveralNo ratings yet
- Etiologies of Fever of Unknown Origin in Adults - UpToDate (2019) PDFDocument17 pagesEtiologies of Fever of Unknown Origin in Adults - UpToDate (2019) PDFMoisés León RuizNo ratings yet
- Sengupta Et Al., 2022 - COVID-19 & Vitamin CDocument8 pagesSengupta Et Al., 2022 - COVID-19 & Vitamin CDr.Pallav SenguptaNo ratings yet
- Rehabilitation After Amputation of The Lower Limb in The Course of Diabetic Foot SyndromeDocument7 pagesRehabilitation After Amputation of The Lower Limb in The Course of Diabetic Foot SyndromeNoreen PunjwaniNo ratings yet
- TH ND ST RDDocument5 pagesTH ND ST RDJOANA KRIS CABALTERANo ratings yet
- Zuqiaoyin Gb-44: Yin Portals of The FootDocument2 pagesZuqiaoyin Gb-44: Yin Portals of The Footray72roNo ratings yet
- Kriteria 4 Tabel 10 18 - 08 - 2022Document23 pagesKriteria 4 Tabel 10 18 - 08 - 2022harsya Yuli RachmantoNo ratings yet